
Abstract
Gray zone lymphoma, also known as B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma, is a rare malignancy with overlapping features of both diffuse large B-cell lymphoma and classical Hodgkin lymphoma. Most commonly mediastinal involvement is seen. Extranodal involvement is rare. In this case report, we present the case of a 59-year-old male who presented with stress-related left shoulder pain, ultimately diagnosed with gray zone lymphoma. The patient was treated with etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin-rituximab (EPOCH-R) regimen followed by consolidation radiotherapy resulting in complete response. We are highlighting this case as rare and atypical presentation of a rare disease.
Introduction
In 1998, at a workshop on Hodgkin’s disease and related diseases, the term gray zone lymphoma (GZL) was first used to identify lymphomas with mixed features of classic Hodgkin’s lymphoma (cHL) and non-Hodgkin’s lymphoma. 1 In the fourth edition of the Classification of Tumors of Hematopoietic and Lymphoid Tissue, GZL was introduced by the World Health Organization for the first time in 2008 as either B-cell lymphomas unclassifiable (BCLu) with features intermediate between diffuse large B-cell lymphoma (DLBCL) and cHL (BCLu-DLBCL/cHL) and B-cell lymphomas unclassifiable with features intermediate between DLBCL and Burkitt lymphoma (BL; BCLu-DLBCL/BL). 2 Thus, GZLs are tumors that encompass overlapping morphological, immunophenotypic, as well as clinical features of DLBCL and cHL, especially PMBL and nodular sclerosis cHL or DLBCL and BL. 3 GZL most commonly occur in mediastinum and hence are known as mediastinal GZL (MGZL), whereas lymphomas occurring in peripheral lymph nodes are referred as non-mediastinal GZL (NMGZL). MGZL typically occurs in young adults in the third and fourth decades as compared with NMGZL, which typically occurs in older and more often present with advanced-stage disease. Both MGZL and NMGZL when compared with cHL and primary mediastinal BCL are more aggressive with poor clinical outcomes. 4 In this article, we report a unique case of NMGZL with skeletal involvement as initial presentation.
Case Report
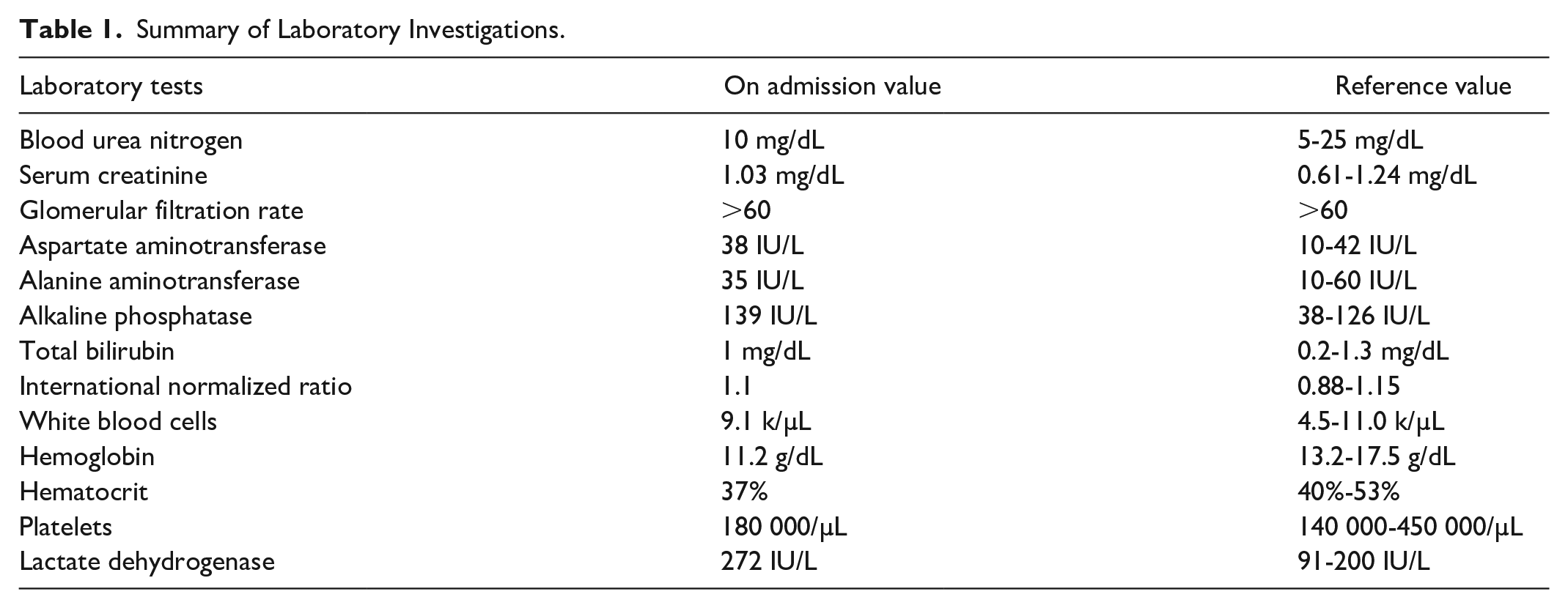
A 59-year-old male presented to the emergency department with complaints of left shoulder pain for 3 weeks. He was moving furniture, which resulted in sudden onset of pain, which was briefly relieved by ibuprofen but became progressive with tingling numbness in the left arm. Eventually, he came to the emergency department for further evaluation. He also mentioned about night sweats. His vital signs in the emergency room showed blood pressure of 106/64 mm Hg, heart rate of 75 beats per minute, respiratory rate of 14 breaths per minute, temperature of 100.6 °F. Physical examination was only remarkable for point tenderness over the left coracoid process with a restricted range of motion and pain on abduction of the shoulder. There was no lymphadenopathy. Initial laboratory investigations revealed mild anemia, elevated lactate dehydrogenase, and alkaline phosphatase, as shown in Table 1.
Summary of Laboratory Investigations.
Computed tomography scan of the left shoulder with contrast demonstrated a 10 × 8 mm lytic lesion along the coracoid of the scapula with enlarged left axillary lymph nodes (Figure 1A). The patient eventually got magnetic resonance imaging of left shoulder, which demonstrated abnormal marrow signal within the coracoid process of the scapula, with a cortical disruption, periosteal reaction, and multiple foci of enhancement within the humerus with no evidence of rotator cuff tear (Figure 1B). Findings were concerning for malignancy. The whole body bone scan showed increased activity in the left glenoid process with no other discrete areas of abnormal uptake (Figure 1C and D). During hospitalization, the patient had a bone biopsy by interventional radiology with histopathology and immunophenotype (Figure 2A-F) showing atypical intertrabecular lymphohistiocytic infiltrate containing small and large lymphocytes in the background of necrosis. Large cells demonstrated marked cytologic atypia with irregular hyperchromatic nuclei and abundant cytoplasm with few showing Reed-Sternberg–like morphology. Neoplastic cells were positive for CD15, CD20, CD30, CD45, CD79a, MUM1, and PAX5 with partial weak staining of BOB1, OCT2, and BCL2. Neoplastic cells were negative for BCL6 and Epstein-Barr virus. Based on the above findings, diagnosis of lymphoma, unclassifiable with features intermediate between DLBCL and cHL was made.

(A) Computed tomography scan of left shoulder showing lytic lesion along the coracoid of the scapula. (B) Magnetic resonance imaging of left shoulder showing abnormal marrow signal within coracoid process of scapula. (C and D) Bone scan showing increased activity in left shoulder region.

(A) Hematoxylin and eosin stain slide showing tumor characteristic. (B) CD15-positive tumor cells consistent with classic Hodgkin’s lymphoma (cHL). (C) CD20-positive tumor cells consistent with diffuse large B-cell lymphoma (DLCBL). (D) CD30-positive tumor cells consistent with cHL. (E) CD79a-positive tumor cells consistent with DLCBL. (F) MUM1-positive tumor cells consistent with cHL.
The patient was started on etoposide, prednisone, vincristine, cyclophosphamide, hydroxydaunorubicin, and rituximab (EPOCH-R) chemotherapy regimen consisting of 6 cycles. Bone scan repeated after chemotherapy showed no evidence of residual disease. The patient subsequently received consolidative radiotherapy for 15 sessions with a dose of 30 Gy in 15 fractions over 3 weeks. The patient currently remains disease-free with complete resolution of shoulder pain.
Discussion
In this article, we report a unique case of skeletal involvement as initial presentation in a patient who presented with shoulder pain and mild fever with eventual workup with imaging and biopsy showed NMGZL. As a group, Traverse-Glehen et al were first to describe GZL as a type of lymphoma with combining features of cHL and DLBCL in the year 2005. 3 Patients with mediastinal involvement usually are young males as described by Wilson et al, who studied 24 patients with a median age of 33 years in which 46% had mediastinal masses ≥10 cm with few patients having extranodal involvement. 5 Few patients may present with compressive symptomatology like dyspnea and superior vena cava syndrome suggestive of bulky (≥10 cm) anterior mediastinal tumors. 2 Similar findings were reported by other researchers.6-8 In a study by Evens et al analyzing 112 patients, 57% were without mediastinal involvement with 50 years being the median age of presentation, 8% cases had a bulk disease, and 27% had >1 extranodal site of disease. 9 Other organ system involvement, including lung, liver, and spleen, has been described.2,3 Our patient presented at 59 years of age with skeletal involvement as an initial presentation without mediastinal or bulk disease, making it a unique case.
Diagnosis of GZL remains challenging as within same tumor sample morphologies usually seen with cHL and DLBCL can be observed. Hence, for correct diagnosis extensive sampling with excisional or incisional biopsy and expert pathological evaluation may be warranted. 4 Confluent sheets of tumor cells in abundance with less inflammatory cells in the background are important for making the diagnosis of GZL; however, eosinophils, histiocytes, and small lymphocytes can be seen with a variable degree of fibrosis and necrosis.10,11 As observed in our case, morphologically neoplastic cells have pleomorphic nuclei, with more infrequent eosinophilic nucleoli than the Reed-Sternberg cells seen in cHL disease. 10 As seen with morphology, GZL immunophenotypically also shows overlapping features between cHL and DLBCL. If morphology is like cHL, expression of CD20 and other B-cell markers like CD79a, PAX5, OCT2, and BOB.1 with variable expression of CD15 or CD30. Similarly, cases with morphology like DLBCL may show expression of CD15 or CD30 with variable expression of B-cell markers with EBER (Epstein-Barr virus-encoded small RNA) being typically negative suggests GZL as diagnosis.11-13 Mostly B-cell markers like CD20, PAX5, CD79a, BCL6, BOB1, OCT2, along with CD30, CD15, MUM1, and EBER are the immunohistochemical panel recommended for diagnosing GZL. 10 Our case also showed a similar immunophenotypic presentation. When relapse occurs testing for PD-L1 should be done to decide further therapy as many cases express PD-L1. 14
Treatment of GZL is not yet standardized due to its rarity creating diagnostic challenges as well as establishing gold standard therapy. 4 In a prospective study of 24 MGZL treatment regimen with DA-EPOCH-R was found to be effective. 5 Another study of 112 GZL patients treated across 19 North American centers, which had 43% patients with MGZL and 57% had NMGZL, the majority of the patients got CHOP+/−R and ABVD+/−R with a few getting DA-EPOCH-R. As part of frontline therapy, rituximab was received by two thirds of the patients. In patients treated with ABVD+/−R and DLBCL-based regimen (ie, CHOP+/−R and DA-EPOCH-R) progression-free survival rate at 2 years was, respectively, 22% and 52% showing superior outcome when treated with DLBCL-specific regimen. However, there was no statistical difference in survival rates between MGZL and NMGZL patients. 9 In a retrospective analysis on 16 patients of MGZL, 5 patients treated with DA-EPOCH-R regimen and 2 patients treated with R-HCVAD/MA regimen had 100% complete response. Complete response for 6 patients treated with CHOP-R regimen and 3 patients treated with ABVD regimen was, respectively, 50% and 33%. Two-year progression-free survival was significantly longer for patients treated with DA-EPOCH-R regimen as compared with other regimen but no difference was found in overall survival. 15 Kritharis et al recommended treatment of MGZL or NMGZL with either R-CHOP or DA-EPOCH-R regimen with use of consolidative radiotherapy for localized and/or bulky tumors having size of >10 cm with consideration for salvage chemotherapy followed by consolidation with autologous hematopoietic stem cell transplantation for relapsed or refractory GZL. 16
Conclusion
We report a rare case of NMGZL with skeletal involvement as an initial presentation with a localized disease, which was treated with EPOCH-R regimen followed by consolidative radiotherapy for localized disease resulting in complete response. Further studies, including large prospective trials, are needed to better understand this disease and fine-tune treatment strategies incorporating the use of novel targeted immunotherapy like brentuximab vedotin and programmed cell death 1 inhibitor for a better outcome.
Footnotes
Author Contributions
IS contributed to case selection, planning and preparing of the manuscript. AA contributed to discussion part and editing of manuscript. VU contributed to case presentation of manuscript. SD and SM contributed with editing of manuscript. TF contributed to pathological slide review. DF contributed to interpretation of radiological images. ML reviewed and finalized the manuscript MAH contributed significantly in preparation of the manuscript, editing, and final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.