
Abstract
Monoclonal gammopathy of undetermined significance is a precursor to multiple myeloma characterized by monoclonal gammopathy without evidence of end organ damage. Some patients with clonal plasma cell disorder that do not meet the requirements for multiple myeloma have been seen to develop pathologic renal disease due to direct effects from deposition of monoclonal protein, referred to as monoclonal gammopathy of renal significance. In this article, we present a rare renal manifestation of monoclonal gammopathy of renal significance as focal segmental glomerulosclerosis.
Case Report
A 73-year-old Caucasian male with a past medical history of hypertension presented to the hospital for progressive lower extremity edema and shortness of breath. Laboratory work showed a worsening of creatinine at 3.1 mg/dL, an increase from 1.1 mg/dL 1 month ago. Twenty-four-hour urine quantification showed nephrotic range proteinuria with 26 g of urine protein, urine albumin to creatinine ratio of 11 791, and serum albumin of 1.8 g/dL. Workup included normal echocardiogram and HbA1c of 5.8. Autoimmune workup with ANA, anti-dsDNA, anti-proteinase 3 antibody (c-ANCA), and anti-myeloperoxidase antibody (p-ANCA) were all negative. He had normal serum C3 and C4 complement levels. HIV screen, hepatitis B surface antigen, and anti-hepatitis C virus antibody were negative. The patient was thoroughly questioned about bisphosphonate use, recent viral illnesses (cytomegalovirus), or recent blood-tinged coughing and prior tuberculosis exposure, all of which were unremarkable according to the patient.
Serum protein electrophoresis showed 2 immunoglobulin G Kappa monoclonal bands (0.2 g/dL and 0.3 g/dL) confirmed with immunofluorescence. Serum free light chain ratio was elevated at 10.96, serum kappa light chain levels were elevated at 521 mg/L, and serum lambda light chains were elevated at 47.6 mg/L. The patient underwent a kidney biopsy and the results showed an acute tubular epithelial cell injury with focal sclerotic glomeruli and mild mesangial hypercellularity (Figure 1). Immunofluorescence on frozen tissue was negative for staining and electron microscopy was negative for immune deposits but showed 40% podocyte effacement (Figure 2). Despite a normal kidney biopsy, a bone marrow biopsy was performed 3 weeks later to investigate the elevated serum free light chain ratio and showed 10% plasmacytosis. Over the course of 2 months, the patient’s kidney function continued to deteriorate. Despite tubular injury justifying worsening renal function, there was still questions of tubular injury causing such massive proteinuria, in addition to the concern that an immunofluorescence paraffin technique had not been performed on the initial biopsy, which can be sensitive to certain light chain tubulopathies.

Initial kidney biopsy showing tubular epithelial cell injury characterized by cellular swelling (a) and collapsing segmental sclerosis of the glomerulus, due to the accumulation of detached, injured podocytes with in Bowman’s capsule (b).

Electron microscopy showing podocyte effacement from the glomerular basement membrane (a). Positive immunofluorescence for deposition of kappa light chain (b) and lambda light chain (c) in the glomerular capillary loops on the repeat kidney biopsy.
As a result, a repeat kidney biopsy was performed showing acute severe tubular injury with collapsing type focal sclerotic glomeruli, electron microscopy demonstrating 90% podocyte effacement, and immunofluorescence with paraffin technique positive for kappa light chain and lambda light chain (kappa greater than lambda). As a result, the diagnosis of focal segmental glomerulosclerosis secondary to monoclonal gammopathy of renal significance (MGRS) was made. Given the patient’s positive result for kappa light chain on immunofluorescence, APOL1 gene testing was not performed given the high likelihood of MGRS. The patient was subsequently started on a CyBorD chemotherapy regimen, and after 6 cycles, the patient’s outpatient laboratory creatinine level was improved to 1.4 mg/dL. Additionally, there was improvement of proteinuria with urine albumin to creatinine ratio decreasing to 7456 and serum albumin improving to 2.9 g/dL.
Discussion
Monoclonal gammopathy of undetermined significance (MGUS) is a precursor to multiple myeloma (MM) characterized by monoclonal gammopathy without evidence of end organ damage. 1 MGUS has a rate of progression to MM of 1% per year.1,2 Diagnosis of MGUS is based off findings of serum monoclonal protein <3 g/dL and bone marrow plasma cells <10%. 1 Some patients with clonal plasma cell disorder that do not meet the requirements for MM have been seen to develop pathologic renal disease due to direct effects from deposition of monoclonal protein, referred to as MGRS. 1
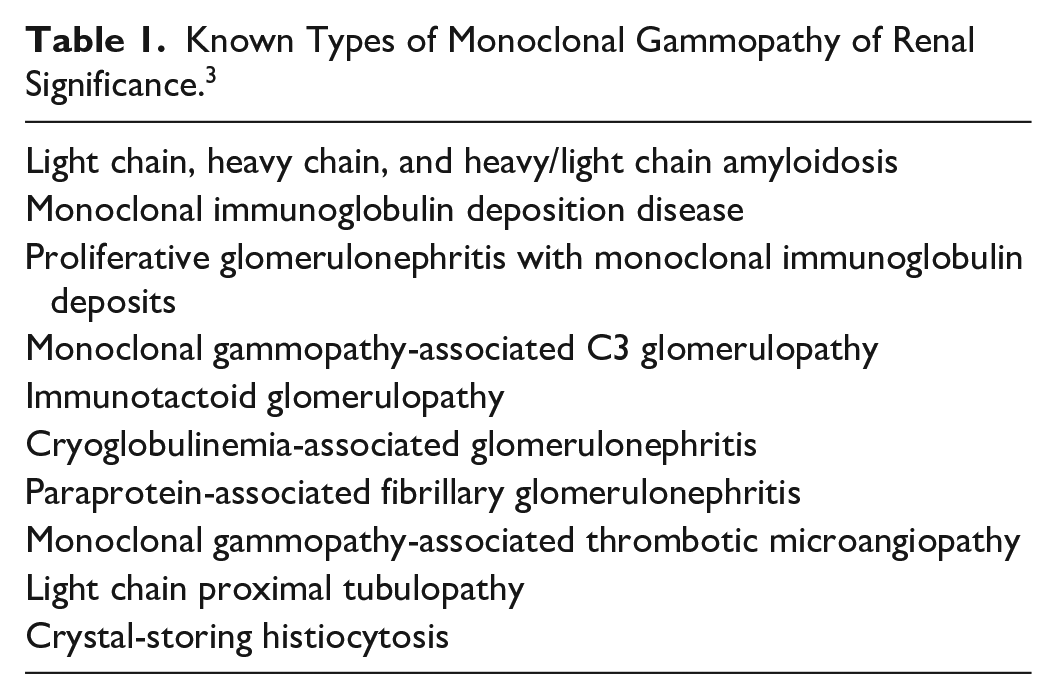
There are several kidney diseases known to be associated with monoclonal gammopathy and the list continues to grow. The incidence and prevalence of the various type of MGRS is generally unknown, as they are only described in various case reports and small case series. 3 A list of various known types of MGRS is shown in Table 1. 3 One potential complication of MGRS is focal segmental glomerulosclerosis (FSGS), a form of glomerulopathy with potential for progression to end-stage renal disease (ESRD). 4 FSGS is considered a podocyte disease leading to effacement of the foot processes causing nephrotic range proteinuria that is typically progressive and irreversible. 5 Typical histologic features include segmental obliteration of glomerular capillaries by extracellular matrix, along with effacement of foot processes and absence of immune deposits on electron microscopy. 5
Known Types of Monoclonal Gammopathy of Renal Significance. 3
FSGS is classified as “primary” or idiopathic, and “secondary,” which is related to an underlying disease state. 2 The list of “secondary” causes of FSGS include genetic causes, virus-associated causes, and drug-induced causes. 5 When considering genetic causes, one gene that has been implicated as having a strong association with FSGS is the Apolipoprotein L1 (APOL1) gene. 5 Investigations have shown this gene to be strongly associated with FSGS in patients of African descent. 5 The mechanism in which the APOL1 gene acts on the podocyte to cause FSGS is currently unknown. 5 Furthermore, a number of viruses have been implicated in FSGS, including HIV and cytomegalovirus. 5 It is thought that viruses act on the podocyte via direct infection or by release of inflammatory cytokines to cause FSGS. 5 Infection with Mycobacterium tuberculosis and the use of certain drugs such as the bisphosphonate pamidronate have been implicated as well.5,6 Initial evaluation of our patient included an HIV screen, as well as thorough questioning regarding his medication history, recent viral illnesses, and whether the patient had known exposure to or symptoms consistent with tuberculosis infection. HIV testing was negative, and the patient denied the use of bisphosphonates, recent viral illness, or symptoms consistent with tuberculosis. After kidney biopsy was performed, and immunofluorescence returned positive for kappa light chain, there was high suspicion that FSGS was due to MGRS. Because of this, and the fact that the patient was not African American, APOL1 testing was not performed.
FSGS due to MGRS is rare; however, few case reports have described the association.2,7,8 Details of the relevant clinical information from these cases are described in Table 2. While these reports describe cases in which there is a possible association between FSGS and MGRS, only one of these reports has addressed potential treatment for the condition. The report by Torun et al utilized immunosuppressive therapy followed by autologous bone marrow transplant as the treatment modality for their patient presenting with elevated creatinine and nephrotic range proteinuria, leading to improvement in the patient’s proteinuria and creatinine levels. 7 Currently, treatment for primary FSGS is well established; however, there is little consensus regarding treatment of FSGS due to MGRS. In fact, many patients with MGRS go untreated due to the practice of using malignancy (MM) as a prerequisite for the use of chemotherapy in these patients, and there are currently no evidence-based recommendations for treatment.1,3
Cases That Included a Differential Diagnosis of FSGS Secondary to MGRS, in Comparison With the Case Presented Here.

Abbreviations: FSGS, focal segmental glomerulosclerosis; MGRS, monoclonal gammopathy of renal significance; SPEP, serum protein electrophoresis; IF, immunofluorescence; EM, electron microscopy; IgG, immunoglobulin G; NA, not applicable.
Conclusion
We present a case of a patient who presented with worsening renal function and nephrotic range proteinuria. Serum electrophoresis, bone marrow biopsy, and renal histology were consistent with FSGS due to MGRS. Without treatment, the patient was at high risk of developing ESRD. Due to the unusual presentation and high risk of progression, nephrology and oncology were consulted and the decision was made to treat with a chemotherapy regimen consisting of cyclophosphamide, bortezomib, and dexamethasone (CyBorD), a common regimen used in the treatment of MM. After 5 months, the patient saw improvement in his creatinine levels, proteinuria, and serum albumin signifying a halt in the progression toward ESRD. The improvement seen in this patient highlights promise for the use of CyBorD in the treatment of FSGS due to MGRS.
Footnotes
Author Contributions
All authors have contributed equally to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information.