
Abstract
The prevalence of serotonin syndrome increases over the past several years as more serotonergic medications are being used in clinical practice. It is a potentially lethal condition caused by excessive serotonergic activity. Common causes of serotonin syndrome are the use of prescription medications, illicit drugs, or a combination of substances, leading to an increase in the activity of serotonin in the central and peripheral nervous system. The clinical symptoms range from mild to severe. We report a case of a 25-year-old woman with polysubstance abuse, including cocaine, who presented with confusion, rigidity, high-grade fever, and reduced biventricular function on echocardiogram. Based on the combination of substance used history, clinical presentation, and echocardiogram findings, she was diagnosed with serotonin syndrome complicated by takotsubo cardiomyopathy. She improved after being treated in the intensive care unit and was discharged from the hospital. This patient demonstrates the importance of recognizing and promptly initiating management of serotonin syndrome in order to improve morbidity and mortality.
Introduction
The prevalence of serotonin syndrome increases over the past several years due to the increased use of serotonergic drugs. 1 The clinical presentation ranges from mild to severe symptoms. The patient with mild symptoms can present with hyperreflexia, tremor, myoclonus, anxiety, restlessness, diaphoresis, mydriasis, and tachycardia. Severe symptoms consist of rigidity, respiratory failure, seizure, alteration of mental state, hyperthermia, and hemodynamic instability. 2 We report a case of a patient with polysubstance abuse who presented with serotonin syndrome–induced takotsubo cardiomyopathy from ingestion of several serotonergic substances.
Case Report
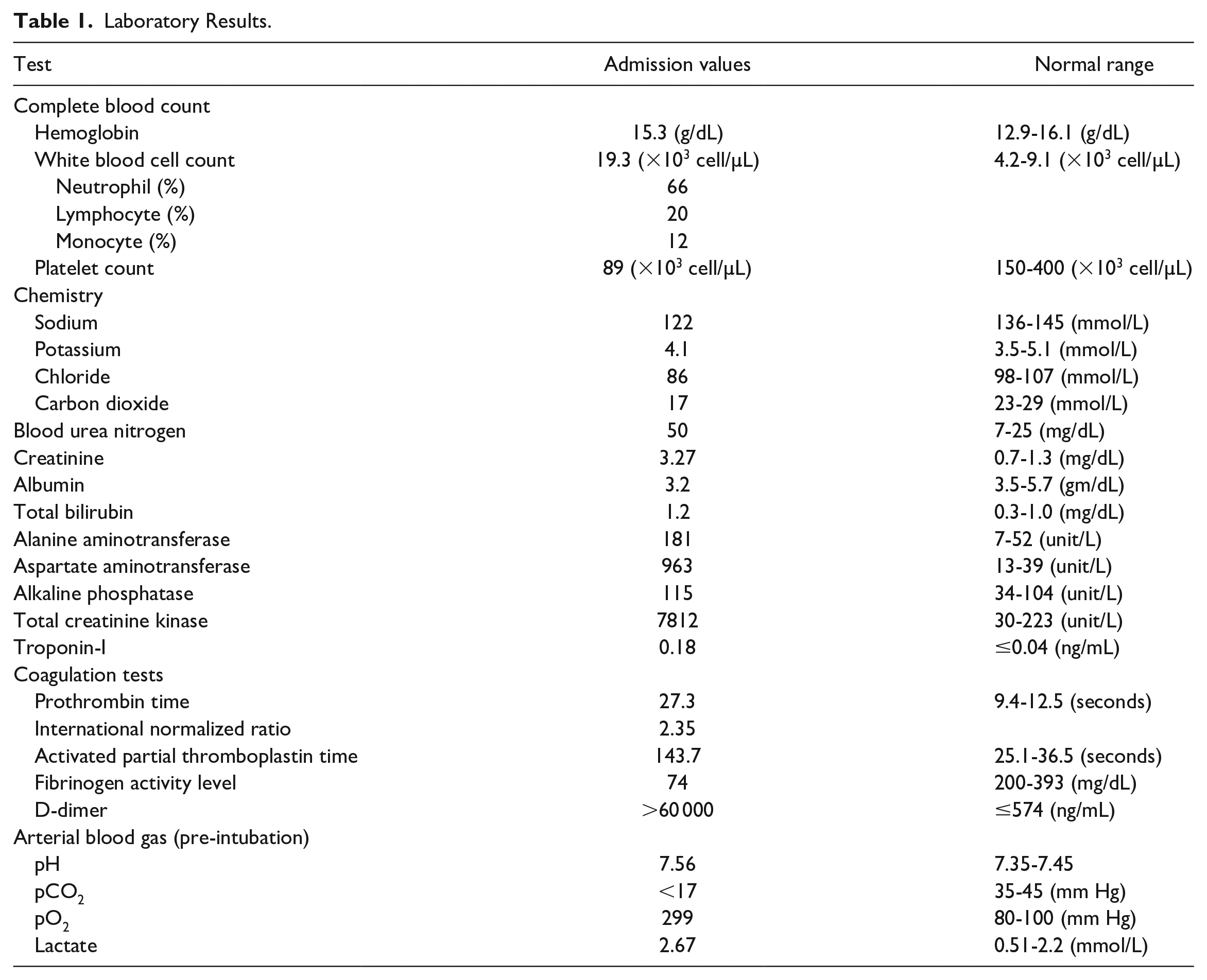
A 25-year-old woman with a history of depression and polysubstance abuse, including heavy alcohol and cocaine use, presented with 1 day of confusion and rigidity in the setting of a month-long episode of labile mood, which began after a change to her antidepressants. Her roommate found empty bottles of zolpidem, lamotrigine, oxycodone, and buspirone next to the patient. Admission vitals revealed hypotension, tachycardia, hypoxia, and hyperthermia to 41.1 °C. Her examination was notable for encephalopathy, flushing, clonus, and rigidity. Admitting laboratory results are detailed in Table 1. Blood cultures were negative. Electrocardiogram (ECG) showed new changes, including a lack of anterior R waves and septal Q waves suggestive of cardiomyopathy. Transthoracic echocardiography (TTE) showed reduced biventricular function with a left ventricular ejection fraction of 25%, and apical hypomobility, consistent with takotsubo cardiomyopathy (Figure 1A and B).
Laboratory Results.

Transthoracic echocardiography (TTE) images at the time of hospital admission and 1 week following hospitalization. TTE with intravenous contrast performed early in the hospitalization course (A and B) shows a classic mid-chamber ballooning of the left ventricle. White arrows in panel A show severe hypokinetic of the apical portion of the left ventricle. Yellow arrows in panel A show relatively preserved basal segment contractility of the left ventricle. TEE performed a week later (C and D) shows normal contractility. Panels A and B represent 4-chambers views. Panels C and D represent Subcostal views.
The patient was diagnosed with severe serotonin syndrome resulting in multisystem organ failure including mixed distributive and cardiogenic shock, acute respiratory failure, acute renal failure, acute liver failure, and disseminated intravascular coagulation. She was treated with cyproheptadine (a serotonin antagonist), sedated with midazolam and hydromorphone, and paralyzed with neuromuscular blockage agents. She had labile hemodynamics with episodes of hypotension and hypertension. She was started on renal replacement therapy for acute renal failure secondary to rhabdomyolysis. The creatine kinase levels peaked at 22 000 U/L. She required 5 days of mechanical ventilation. A follow-up TTE 1 week after initial presentation (Figure 1C and D) showed normal systolic ejection fraction without morphologic changes. The patient was discharged to a rehabilitation facility.
Discussion
Serotonin syndrome has become increasingly prevalent as more serotonergic medications are being used in clinical practice. The clinical presentations vary greatly, ranging from mild to severe.1,3 The triad of clinical presentations are altered mental status, neuromuscular abnormalities, and autonomic hyperactivity. 3 Laboratory abnormalities can include metabolic acidosis, transaminitis, renal failure, rhabdomyolysis, and disseminated intravascular coagulation, which were seen in our patient.
There are at least 3 published diagnostic criteria for serotonin syndrome, including Sternbach’s criteria, 4 Radomski’s criteria, 5 and Hunter’s criteria. 6 Our patient was diagnosed with serotonin syndrome based on Hunter’s criteria in association with the appropriate clinical history and negative blood culture result. Our patient was treated with lamotrigine for her depression and was reported to have “labile mood” preceding the current presentation. Lamotrigine is a known mild 5-HT3 receptor inhibitor, and the reported “labile mood” might have been a mild presentation of serotonin syndrome that was unrecognized. 7 The severity of the serotonin syndrome in our patient is likely caused by a combination of cocaine use and the exposure to higher than prescribed doses of lamotrigine. To our knowledge, our present case is the second reported case of serotonin syndrome associated with lamotrigine in combination with cocaine use. 8
Takotsubo cardiomyopathy is characterized by transient mid segment left ventricular wall motion abnormalities, with or without apical involvement, in the absence of the obstructive coronary disease. Changes in the ECG, along with mild elevation of the cardiac troponin level, were observed. 9 It is also essential to rule out the presence of pheochromocytoma and myocarditis. 9 Our patient was diagnosed with takotsubo cardiomyopathy based on the lack of risk factors for obstructive coronary disease, mild troponin elevation, changes on ECG, and changes observed on TTE. The reversibility of the cardiac dysfunction, including an improvement in ejection fraction from 25-30% to 55-60% on the follow-up TTE, further confirmed our diagnosis. There are at least 4 case reports associating serotonin syndrome with takotsubo cardiomyopathy.10-13 The causes of serotonin syndrome in these case reports are concomitant used of several serotoninergic and/or dopaminergic agents, including a combination of maprotiline (a tetracyclic antidepressant) and dextromethorphan, 13 venlafaxine, 12 phenethylamine, isocarboxazid (a monoamine oxidase inhibitor) and lithium, 11 and venlafaxine, tianeptine sodium, ropinirole, carbidopa/levodopa, bromocriptine mesylate, and methylphenidate. 10 The mechanism by which serotonin syndrome–induced takotsubo cardiomyopathy is likely a result of the hyperadrenergic state. 14 The surge in catecholamines can lead to excessive stimulation of β1-adrenergic receptors, increased production of the extracellular matrix, contraction band necrosis, and disturbance of the calcium regulatory protein (ie, sarcolipin). 14 The prognosis of takotsubo cardiomyopathy and serotonin syndrome is favorable if recognized early and treated with supportive care. However, in patients with cardiogenic shock as in our patient, short-term mortality (28-30-day mortality) can be as high as 5.9% (range between 4.1% and 5.9%). 15 Accordingly, it is important to recognize the diagnosis of takotsubo cardiomyopathy and its trigger for appropriate management in a timely fashion.
As the prevalence of serotonin syndrome increases, it is important to recognize the potential life-threatening condition associated with it, including takotsubo cardiomyopathy, as in our patient. The treatment includes removal of the offending agent and supportive therapies, including sedation with benzodiazepines, the use of serotonergic antagonists, and in severe cases, paralysis with external cooling.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval or a consent from a patient for reporting an anonymized individual case.
Informed Consent
Informed consent for patient information to be published in this article was not obtained. The patient’s information was altered to protect the patient’s privacy.