
Abstract
Acute interstitial nephritis is a well-known cause of acute kidney injury, but its association with cocaine use is extremely rare. In this article, we chronicle the case of a patient who developed acute interstitial nephritis secondary to cocaine insufflation. Furthermore, we conducted a systematic literature search of MEDLINE, Cochrane, Embase, and Scopus databases regarding cocaine-induced acute interstitial nephritis. A comprehensive review of the search results yielded a total of 7 case reports only. The data on patient characteristics, clinical features, biochemical profiles, treatment, and outcomes were collected and analyzed. This paper illustrates that acute interstitial nephritis may be added to the list of differentials in patients with acute kidney injury and a history of cocaine use. The therapeutic approach for cocaine-related kidney disease may be different than other etiologies responsible for acute renal insult. Prompt recognition of this entity is crucial because such patients may ultimately develop severe deterioration in renal function.
Introduction
Acute interstitial nephritis is an underrecognized cause of acute kidney injury. It leads to decreased creatinine clearance and is characterized by an inflammatory infiltrate in the kidney interstitium, sparing the glomeruli. 1 The occurrence of this entity has been described in association with a multitude of diseases ranging from intrinsic kidney pathologies to systemic diseases involving immune alterations like systemic lupus erythematosus, sarcoidosis, several infections, or following the use of certain medications.2,3 Notably, physicians also encounter difficult-to-diagnose cases of acute interstitial nephritis where a precise etiology cannot be deciphered. In such cases, the underlying pathogenesis has mostly been attributed to aberrant autoimmune mechanisms. 4 In this article, we describe an interesting case of a young patient who was eventually diagnosed with acute interstitial nephritis secondary to cocaine use. He showed clinical improvement, and his biochemical profile normalized with conservative management and cocaine cessation.
This article highlights acute interstitial nephritis as a possible cause for acute kidney injury in patients having a history of cocaine use. Clinicians should maintain a high index of suspicion for cocaine-associated acute interstitial nephritis, particularly due to its nonspecific clinical presentation and potential to cause severe renal dysfunction. This paper also serves the purpose of community awareness regarding this unusual association between acute interstitial nephritis and cocaine use. Population-based studies are warranted to assess the magnitude of this pathologic relation. It will not only broaden the scope of our knowledge on this issue but will also help frame guidelines to standardize the care of such patients.
Case Presentation
This case study involves a 27-year-old Caucasian male who developed a dull aching type of abdominal pain, fever, cough, and chest congestion with flu-like illness over the past 5 days. He used ibuprofen 200 mg 2 times a day for the past 2 days, with brief improvement in his symptoms. Subsequently, he experienced a focal to bilateral tonic-clonic seizure while working at a hardware store 1 day ago. He was initially brought to a nearby satellite facility. His biochemical profile was unremarkable, except for a deranged renal function. He was initiated on 500 mg levetiracetam twice daily, and magnetic resonance imaging of brain with gadolinium and electroencephalography were planned. He had been having occasional seizure episodes for the past 7 years, but he refused to start anticonvulsant therapy. He remained seizure-free for 24 hours after initiation of levetiracetam at the facility. The patient was then transferred to our hospital for further evaluation and management of his worsening renal function.
On detailed inquiry, he admitted having large amounts of daily intranasal cocaine 1 week ago, immediately preceding his clinical symptoms. He had been smoking marijuana and snorting cocaine 3 to 4 times per week for past several months but denied intravenous drug use. He chewed tobacco for 4 years but suspended its use 1 year ago. He also reported binge alcohol consumption. He denied stabbing chest or flank pain, nausea, vomiting, or change in bowel habits. There was no history of sore throat, joint swelling, skin rash, dysuria, or hematuria. Family history was negative for autoimmune diseases and tuberculosis. Abdominal examination was remarkable for diffuse tenderness with normal bowel sounds.
Investigations
Laboratory evaluation revealed elevated serum creatinine levels, 2.8 mg/dL (baseline: 1.1 mg/dL), normal creatine phosphokinase, 226 U/L (39-308 U/L), and insignificant peripheral eosinophil count, 2%, consistent with acute kidney injury. The details of the laboratory studies are provided in Table 1. Urinalysis revealed pH 5.5, specific gravity 1.015, and proteinuria 30 mg/dL. A trace amount of blood was present, but ketones, nitrates, and leukocyte esterase were absent. Urine microscopy showed 4 to 5 white cells per high-power field and a few scattered red cells. It was negative for leukocytes, including eosinophils by special stain, pigmented granular casts, and bacteria. Urine culture also came out negative. Urine toxicology screen was positive for cocaine.
Laboratory Investigations of the Patient With Respective Reference Ranges.
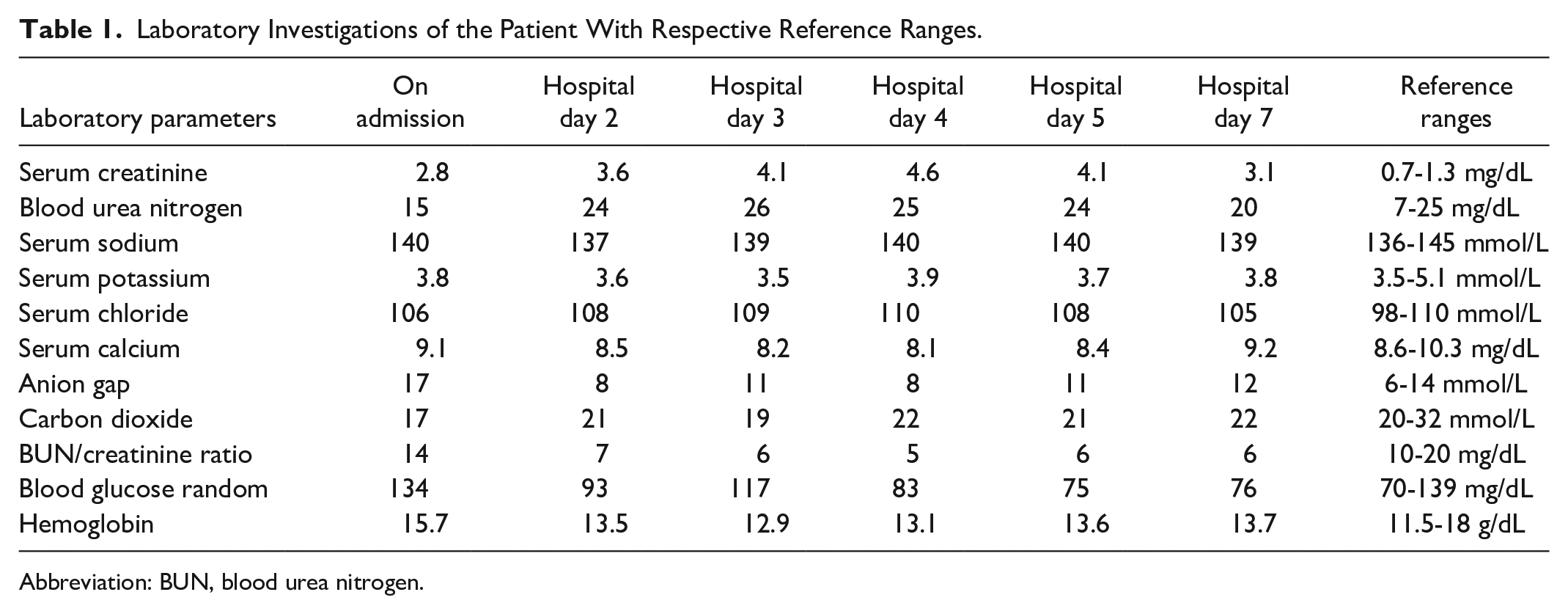
Abbreviation: BUN, blood urea nitrogen.
His hemoglobin A1c, serum lipase, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, and total bilirubin were unremarkable for abnormalities. The measurements of serum complement levels were within normal limits. Tests for cytoplasmic-antineutrophil cytoplasm antibodies (c-ANCA), perinuclear-ANCA (p-ANCA), myeloperoxidase-ANCA (MPO-ANCA), and antiproteinase 3-ANCA (PR3-ANCA) were negative. Furthermore, rheumatoid factor, anti-glomerular basement membrane (anti-GBM), anti–Sjögren’s-syndrome–related antigen A (anti-SSA), anti-apoptosis signal-regulating kinase 1 (anti-ASK1), anti–double stranded DNA (anti-dsDNA), anti-smooth muscle (anti-SM), anti-streptolysin O (ASO) titer, and anti-ribonucleoprotein particles (anti-RNP) antibodies were also negative. Serology for human immunodeficiency virus, and hepatitis B and C were negative for an active infectious process.
Computed tomography scan of the abdomen and pelvis without contrast showed nonspecific bilateral perinephric stranding, with a thickening along the anterior portion of the Gerota’s fascia. Renal Doppler ultrasonography ruled out renal artery stenosis and aortic dissection. Transthoracic echocardiogram showed normal wall motion and ejection fraction. Electrocardiogram was also normal. Chest radiograph was negative for hilar nodules. Subsequently, an uneventful renal biopsy was performed. The histopathologic examination of the biopsy specimen revealed normocellular glomeruli (Figure 1). An interstitial inflammatory infiltrate composed of mononuclear cells was present, with no pathologic alterations in the arteries (Figure 2). Patchy interstitial edema along with inflammation was also identified (Figure 3). The biopsy findings ruled out the presence of mitotic figures and tubular necrosis, with no evidence of tubulitis or granulomas (Figure 4). The presence of eosinophils was confirmed, which was suggestive of acute interstitial inflammation (Figure 5).

Pathologic examination of the renal biopsy specimen showing normocellular glomeruli (periodic acid-Schiff staining; 20×).

Histopathologic analysis of renal biopsy showing mononuclear inflammatory cells. The arterial wall abnormalities were absent (hematoxylin and eosin staining; 20×).

Pathologic examination of the biopsy specimen showing interstitial inflammation and edema (hematoxylin and eosin staining; 20×).

Histopathology of renal biopsy demonstrating interstitial edema with no mitotic figures and no tubular necrosis. No evidence of tubulitis or granulomas was present (trichrome staining; 20×).

Pathologic examination showing eosinophils, suggestive of acute interstitial inflammation (hematoxylin and eosin staining; 20×).
Differential Diagnoses
In terms of possible causes of his acute kidney injury, certain etiologies related to cocaine use were high on the list that can cause rhabdomyolysis, vasculitis, renal infarction, and thrombotic microangiopathy. A variety of autoimmune disorders and infectious etiologies were also considered plausible. Based on the clinical history, extensive diagnostic workup, biopsy findings, and exclusion of the probable etiologies, the patient was diagnosed with acute interstitial nephritis secondary to cocaine use.
Treatment
With regard to the treatment, he was initiated on conservative management with intravenous hydration and maintenance of hemodynamics. Given his relatively mild initial presentation of acute interstitial nephritis and subsequent signs of early recovery, steroid therapy or hemodialysis were not required. He was educated about his disease and was directed to seek professional help for substance use disorder. He was also counseled regarding the importance of continuation of levetiracetam as well as future avoidance of nephrotoxic medications.
Outcome and Follow-Ups
On day 7 of admission, his recovery was good with gradual improvement in renal function. He was discharged from the hospital in a stable condition under ongoing anticonvulsant therapy with levetiracetam 500 mg twice daily. At the 1-week follow-up visit, his renal function showed significant improvement. His serum creatinine trended down to 1.7 mg/dL, and he reported no neurological issues. On subsequent follow-ups, his renal function returned to baseline. The patient has been receiving regular cognitive behavioral therapy sessions for substance use disorder. He has had urine toxicological screens performed, confirming that he has remained abstinent from cocaine. He continues to do well on levetiracetam without any renal or neurological complications to date.
Discussion
Cocaine-associated acute interstitial nephritis is an extremely rare clinicopathologic entity. We conducted a comprehensive search of MEDLINE, Cochrane, Embase, and Scopus databases from inception to date. Search terminologies such as “acute interstitial nephritis,” “acute kidney injury,” “cocaine,” “substance use disorder,” “renal dysfunction,” and the abbreviations (ie, AIN, AKI), were combined using the Boolean operators “AND” and “OR” with the terms “diagnosis,” “management,” and “recovery.” A total of 32 articles consisting of but not limited to original articles, case series, and case reports were initially obtained using the above-mentioned search strategy. The titles and abstracts of all these articles were carefully reviewed for their relevance to our study. A total of 13 articles were first enlisted for rereview, whereas 19 studies were excluded as they were not related to our topic, were in a language other than English, and/or full-text versions were not available. After removing duplicate and redundant articles, 7 case reports only were identified and included in the present article for the final review and analysis.5-11 The data of individual cases of cocaine-related acute interstitial nephritis regarding patients demographics, clinical presentation, laboratory parameters, biopsy status, management, and outcomes are summarized in Table 2.
Literature Review on Cocaine-Induced Acute Interstitial Nephritis.

Abbreviations: BUN, blood urea nitrogen; IV, intravenous; NR, not reported.
Kidney function recovered but patient eventually succumbed to multi-organ failure after subsequent 3 episodes of cocaine-related acute interstitial nephritis.
The data analysis demonstrated that all patients were males with the mean age of 41 years (range: 28-49 years). Of the total 7 patients, 5 were African Americans. The presentation patterns of acute interstitial nephritis were mostly related to nonspecific symptoms like abdominal pain, fatigue, malaise, anorexia, nausea, and vomiting. Urinalysis frequently showed the findings of hematuria and proteinuria. In a majority of patients, serum creatinine levels were considerably elevated, indicating the onset of cocaine-related kidney injury several days prior to hospital admission. The features of an allergic-type reaction, including rash, hives, itching, fever, and eosinophilia, were absent in these patients. The initial presentation of this patient was dominated by abdominal pain and fever, but other classic clinical features of drug-induced acute interstitial nephritis such as rash and eosinophilia were absent. However, it is notable that the published medical literature now denotes acute interstitial nephritis as a heterogeneous disorder with the classic triad of rash, fever, and eosinophilia present in only 10% of cases. 12 Based on his renal function tests, his renal insult was found to be relatively less severe than most of the previously reported similar cases.
In this patient, rhabdomyolysis was considered unlikely due to normal serum creatine phosphokinase levels. Vasculitis was ruled out based on his acute presentation and negative ANCAs. Renal Doppler ultrasound excluded a vascular abnormality or infarction. Furthermore, a transthoracic echocardiogram was inconclusive for cardiac pathologies and embolic phenomena. Thrombotic microangiopathy was not considered based on the findings of his serial testing of serum creatinine, urinalysis, electrocardiography, troponin levels, and liver enzymes. The workup for relevant infectious etiologies was also negative. In terms of prerenal causes of acute kidney injury, he had no evidence of significant volume depletion, hypotension, or renal hypoperfusion. Urine microscopy showed bland sediment with no muddy brown granular casts. Computed tomography scan of the abdomen was unremarkable for urinary obstruction, ruling out the postrenal disease. The absence of a compatible clinical picture, negative serological testing, normal chest radiography, and normal serum calcium levels excluded the possibility of sarcoidosis. Additionally, systemic lupus erythematosus, Sjogren’s syndrome, and infectious etiologies like poststreptococcal glomerulonephritis were also excluded on the standard set of investigations. In light of the clinical and workup findings, intrinsic kidney pathology was considered probable. Thereafter, the pathologic examination of the renal biopsy specimen confirmed acute interstitial nephritis.
Nonsteroidal anti-inflammatory drugs (NSAIDs) also show a propensity to cause acute interstitial nephritis. However, the occurrence of this adverse event is delayed, requiring a prolonged exposure, ranging from several weeks to months. On biopsy, the absence of eosinophils in interstitial infiltrates is the salient pathologic feature in such patients.11,13 In a retrospective study, Schwarz et al 14 demonstrated that NSAIDs-induced disease predominantly causes nephrotic-range proteinuria compared with other causes of interstitial nephritis (38% vs 14%, respectively). Finally, NSAIDs-associated interstitial nephritis typically involves patients older than 60 years, with a female gender predominance having a male-to-female ratio of 1:2. 15 Conversely, the overall presentation of this patient did not fulfill the typical features of NSAIDs-related renal insult. He is a young male who used ibuprofen only for 2 days, and his biopsy findings confirmed the presence of interstitial eosinophilic infiltration. Although his initial urinalysis showed 30 mg/dL proteinuria, it resolved in the subsequent testing. Notably, the timing of the onset of his symptoms was a vital clue to exclude NSAIDs-associated renal pathology in this patient. He developed clinical symptoms after intranasal cocaine binge but before starting the use of ibuprofen. Thus, ibuprofen as the cause for acute interstitial nephritis was unconvincing.
This patient was also initiated on levetiracetam for his focal to bilateral tonic-clonic seizure. However, the medical literature regarding the association between this drug and interstitial nephritis remains limited to anecdotal reports.16,17 In a population-based study, Yau et al 18 showed that the use of levetiracetam was not associated with a higher risk of interstitial nephritis within 30 days (0.33% in levetiracetam users and 0.26% events in nonusers [odds ratio = 1.24; 95% confidence interval = 0.62-2.47]). This patient used levetiracetam only for 1 day before this admission. However, despite continuation of anticonvulsant therapy, his acute kidney injury improved, which was compelling evidence that levetiracetam was not related to his acute interstitial nephritis. At the follow-up visits, he has been tolerating levetiracetam well without any subsequent seizure episodes and his renal function has remained normal thus far. Eventually, after exclusion of all the probable etiologies, the only credible cause was cocaine abuse in this patient. However, it is unclear whether cocaine itself or any of its impurities caused the acute renal injury in this patient.
The exact pathogenesis of drug-induced acute interstitial nephritis remains to be determined. However, an immunologic disturbance, possibly a delayed hypersensitivity T-cell response, appears to be plausible. 19 The main pathogenetic mechanisms may involve molecular mimicry or direct binding of the drug to the tubular basement membrane. 19 The dose-independent nature of the presentation patterns, the extrarenal manifestations of hypersensitivity, and the recurrence of symptoms on reexposure favor this theory. 20 Renal biopsy remains the gold standard for definitive diagnosis in such patients. Pathologic finding of interstitial inflammatory infiltrates of lymphocytes, plasma cells, and eosinophils with normal glomeruli is the hallmark of this disease. 20 Prompt and accurate recognition of acute interstitial nephritis as a cause of acute kidney injury in cocaine users should be considered as imperative. A significant history of cocaine abuse or positive screening test for cocaine, clinical symptoms of abdominal pain or hematuria, and biochemical profile showing elevated levels of serum creatinine are key diagnostic clues for cocaine-associated acute kidney injury.
With regard to the treatment of drug-induced acute interstitial nephritis, withdrawal of offending agent alone may result in rapid recovery of renal function. Corticosteroids are used if drug cessation alone fails to improve renal function in 3 to 7 days. 20 Although the outcomes in patients with severe disease treated with steroids are not extensively investigated, a delay in corticosteroid therapy may result in the worse recovery of kidney function.21,22 The outcomes of both oral and intravenous corticosteroids are comparable with prompt administration. 23 It is notable that the patients with severe acute interstitial nephritis or NSAIDs-related renal syndrome may show suboptimal response to steroids.24,25 In the present data regarding cocaine-induced acute interstitial nephritis, 6 out of 7 patients received steroid therapy. Although they received urgent dialysis, their kidney function improved over the next several weeks. The present patient was unique in this regard as neither had he received dialysis nor steroid therapy. We speculate that his diagnosis was established early in the course of the disease, and his nephritis presentation was not severe compared with previously reported patients. Therefore, his kidney function recovered with conservative management and cocaine cessation.
Learning Points
This study represents the eighth reported case describing the association between acute interstitial nephritis and cocaine use.
An updated knowledge of this possible causal link is imperative for early diagnosis and necessary holistic clinical management.
Detailed drug history is a prudent endeavor in patients with suspicion of acute interstitial nephritis.
In patients with cocaine-induced disease, a timely administration of corticosteroid therapy may hasten the recovery of kidney function.
The identification of more cases of this potential duo will help understand the pathogenesis, which may provide the basis for improvisation of appropriate treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.