
Abstract
Aim:
The authors of the present study speculate that metastasis of breast cancer cells to the temporomandibular joint (TMJ) region mimics classical signs and symptoms of temporomandibular disorders (TMD). The aim of this mapping review was to investigate the association between metastatic breast cancer (MBC) and TMD.
Materials and Methods:
The focused question was, “Is there an association between MBC and TMD?” Indexed databases (PubMed/Medline, EMBASE, OVID, Scopus, Google Scholar, and Web of Science) were electronically searched up to and including March 2022. These databases were searched using different combinations of the following keywords: cancer, carcinoma, temporomandibular disorders, temporomandibular joint, disc displacement disorder, nociception, and tumor. Original clinical studies that meet the inclusion criteria were included. The risk of bias (RoB) was assessed using the Joanna Briggs Institute Critical Appraisal Checklist for case reports. The structure of this current evidence-based review was tailored to primarily condense the relevant information.
Results:
Fifteen case reports were selected after screening the retrieved records from the electronic search. Fifteen out of 16 patients were women aged between 32 and 78 years. All patients were diagnosed with MBC, and most presented with adenocarcinoma. The symptoms identified in patients with TMD included: (a) preauricular pain; (b) preauricular swelling; (c) limited mouth opening; and (d) malocclusion. Fourteen of the included studies had a low RoB, while one had a moderate RoB.
Conclusion:
Based on the currently available evidence, a direct association between TMD and MBC or vice versa cannot be established. Routine visits to medical and oro-dental healthcare providers can contribute toward early diagnosis and management of TMD and MBC.
Introduction
Temporomandibular joint disorders (TMD) encompass nociception and dysfunction of the muscles of mastication and the temporomandibular joint (TMJ). 1 It is also a frequent cause of orofacial pain (OFP).2, 3 The etiopathogenesis of TMD is multifactorial and multifaceted; however, risk factors that are commonly associated with TMD include bruxism, 4 trauma, 5 psychological stress (such as anxiety and/or depression),6, 7 and disk and TMJ morphology and positioning. 8 Patients with TMD often present with symptoms such as preauricular pain (PP) and swelling.9, 10 Nevertheless, such symptoms may also be caused by ganglion cysts of the TMJ and systemic conditions, including metastatic tumors or cancers.11–13
Regardless of its origin, the diagnosis of cancer is debilitating, and its metastasis to other tissues such as bone is even more anguishing as therapeutic prognosis and life expectancy are often compromised. Breast cancer (BC) stands as the most prevalent malignancy in women and serves as a significant contributor to mortality in this population. 14 It has been estimated that by the year 2030, the prevalence of metastatic BC (MBC) would increase by ~55% compared with the year 2015. 15 Osseous metastasis is a common manifestation in patients with MBC. 16 Metastasis to the jaws with emphasis on the mandibular condylar region is relatively uncommon, accounting for <1% of metastatic osseous lesions.17, 18 Studies have shown that MBC may “mimic” signs and symptoms of TMD such as limited mouth opening (LMO), PP, preauricular swelling, and headache.12, 19, 20 According to some reports,12, 21–23 TMD may even present as an early sign of MBC. For instance, in a case report, a 48-year-old female presented with a 12-year history of adenocarcinoma of the left breast. 12 The patient had signs and symptoms of PP, LMO, swelling, and clicking in the TMJ. Radiographic findings suggested cancer metastasis of the bilateral TMJ, as a biopsy was not performed. 12 In another case report, a female with a history of adenocarcinoma of the breast presented with complaints of LMO of up to 2 mm. 20 Following the surgical removal of fibrous tissues and their histopathological examination, islands of breast adenocarcinoma that infiltrated into the TMJ meniscus were evident. 20
Based on the currently available indexed evidence, the authors of the present study speculate that metastasis of BC cells to the temporomandibular region (TM region) mimics classical signs and symptoms of TMD. However, there are no studies that have reviewed the subject. The aim of the present mapping review was to investigate the association between TMD and MBC.
Materials and Methods
Focused Question
The focused question is, “Is there an association between MBC and TMD?” This review was formulated according to the latest Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) guidelines. 24
Inclusion and Exclusion Criteria
Original clinical studies and case reports/series that assessed the association between MBC and TMD were encompassed. Commentaries, perspectives, in vitro/ex vivo studies, studies on animal models, letters to the editor and review articles were excluded.
Database Search Protocol
Two independent investigators (MSS and FJ) searched indexed databases [PubMed (National Library of Medicine), Scopus (Elsevier), Web of Science (Clarivate), and Medline (Ovid)] without any language restriction. Databases were searched up to and including March 2022 using different combinations of the following free text keywords: “breast cancer” or “breast carcinoma” or “metastatic breast cancer” and “temporomandibular disorders” or “temporomandibular joint pain” or “disc displacement disorder” or “mandibular metastases.” Disagreements were resolved via discussion and consultation with a third author (MSZ).
Data Extraction
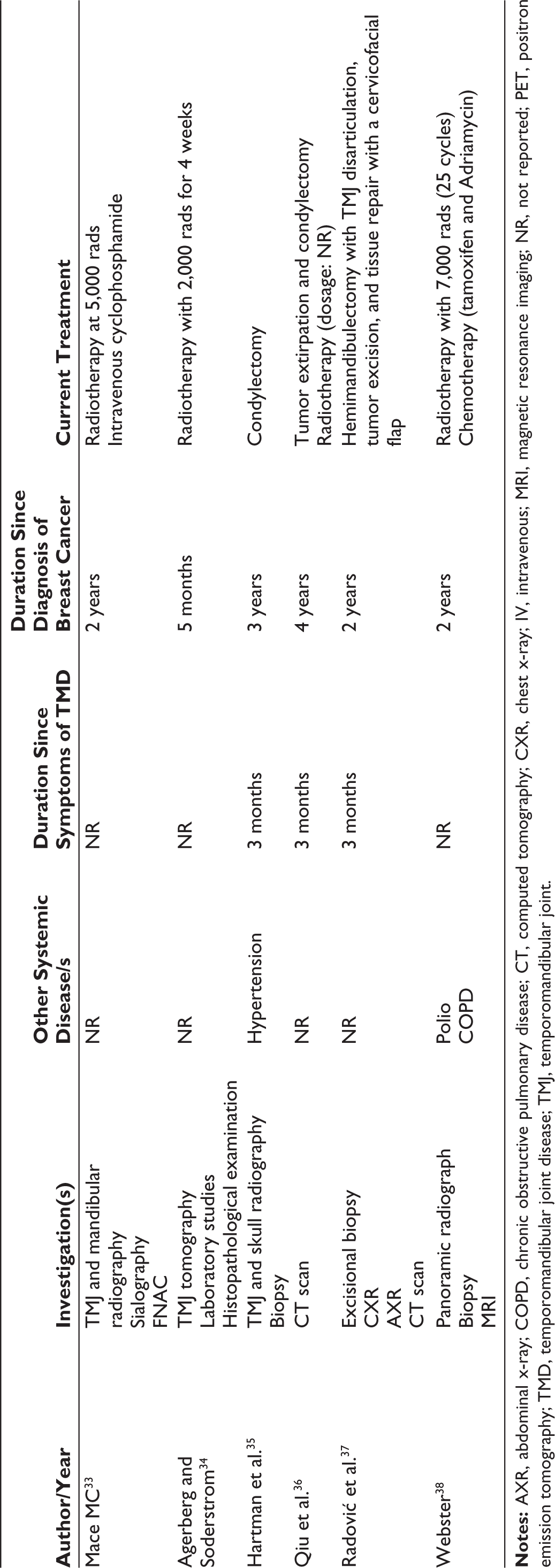
Data extraction comprises the following parameters: (a) author and year; (b) study design; (c) age and gender of participant/s; (d) type of MBC; (e) presenting complaints related to TMD; (f) investigation/s; (g) other systemic disease/s and social history; (h) duration since symptoms of TMD and diagnosis of MBC; and (i) current treatment.
Quality Assessment
The Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports (CACCR) was used to assess the quality of the included studies. 25 This tool consists of eight questions with the following response options: yes, no, and unclear. The following categories were created to summarize the overall quality of the included studies: (a) low probability of bias (studies that achieved a minimum of 75% of the quality criteria); (b) bias potential is moderate (studies that attained a score of 50%–74% of the quality criteria); and (c) high potential for bias (studies that achieved <49% of the quality criteria). 26
Results
Search Results
The initial search yielded a total of 2,507 studies. Duplicates (n = 114) and studies that did not address the focused question (n = 2,378) were excluded (Figure 1). In total, 14 case reports with a single case12, 19, 20, 27–37 and one case report with two cases 38 were included and processed for data extraction. A supplemental file contains search tracking for several databases.
PRISMA 2020 Flowchart.

Demographics
Females with age ranging between 32 and 78 years were examined in 13 case reports.12, 20, 27–37 In a study by Gonzalez-Perez et al., 19 a case of a 73-year-old male was presented. In a study by Webster, 38 cases of a 52-year-old female and a 54-year-old female were presented. All cases were reported from diverse geographic locations, namely, Australia, Brazil, China, Japan, Serbia, Spain, Sweden, Switzerland, the United Kingdom, and the United States (Table 1).
Characteristics of Included Case Reports.

Diagnosis of Breast Cancer
In four studies,19, 27, 31, 37 patients had a diagnosis of invasive ductal carcinoma (IDC). Patients had a diagnosis of adenocarcinoma (undefined type) in six studies.12, 29, 30, 32, 33, 38 In two case reports,20, 28 patients had invasive lobular adenocarcinoma (ILA). In the study by Hartman et al., 35 the patient had intraductal carcinoma. In one study, 36 a precise diagnosis of the type of breast carcinoma was not reported (Table 1). In all included studies,12, 19, 20, 27–38 the duration since the diagnosis of MBC ranged between 1 month and 19 years.
Symptoms in the Temporomandibular Region
In five studies,27, 34–36, 38 patients complained of pain in the unilateral preauricular region, and in four studies,12, 19, 29, 37 patients complained of localized unilateral swelling in the preauricular region. In the study by Stavropoulos and Ord, 28 “altered bite” was reported by a patient with ILA. In the case report by Chang and Thambar, 31 a condylar lesion was incidentally identified in a female patient with IDC of the breast. In three case reports,20, 33, 35 patients complained of LMO. In the case report by Cuttino and Steadman, 32 a patient with adenocarcinoma of the breast presented with pain in the left temporalis muscle. The duration of TMD varied between an unspecified duration (referred to as “several months”) and 7 years.
Other Systemic Conditions in Patients with Metastatic Breast Carcinoma
Six case studies19, 20, 30, 32, 33, 38 reported other systemic conditions in patients with MBC. One patient had a history of ovarian tumor, which had been surgically removed. 30 In three case reports,19, 20, 33 patients had a history of hypertension. In studies by Webster 38 and Cuttino and Steadman, 32 patients had a history of ascites and chronic obstructive pulmonary disease, respectively (Table 2).
Investigations, Other Systemic Disease/Social History, Duration Since Symptoms of TMD and Diagnosis of Breast Cancer, and Current Treatment.

Quality Assessment
Of the 16 cases presented in 15 case reports,12, 19, 20, 27–38 1412, 19, 20, 27–37 had a low and one 38 had a moderate risk of bias (Table 3).
The Joanna Briggs Institute Critical Appraisal Checklist for Case reports.

Q2: Was the patient’s history clearly described and presented as a timeline?
Q3: Was the current clinical condition of the patient on presentation clearly described?
Q4: Were diagnostic tests or assessment methods and the results clearly described?
Q5: Was the intervention(s) or treatment procedure(s) clearly described?
Q6: Was the post-intervention clinical condition clearly described?
Q7: Were adverse events (harms) or unanticipated events identified and described?
Q8: Does the case report provide takeaway lessons?
RoB: risk of bias.
Discussion
Although metastasis of systemic cancers to the jaws is relatively uncommon,17, 18 it has been reported that nearly 30% of breast carcinomas metastasize to the jaws 39 and often spark symptoms in the TM region including PP, LMO, and pre-auricular swelling.30, 32, 36, 37 Therefore, the authors of the present study speculated if there is a bidirectional relationship between TMD and MBC; that is, either TMD may be indicative of MBC in undiagnosed patients, or MBC may elicit TMD symptoms. A vigilant review of pertinent indexed literature was performed with an expectation to retrieve longitudinal and retrospective studies with an adequate sample size that could help address the focused question. However, 14 case reports with a single case12, 19, 20, 27–37 and 1 case report with two cases 38 fulfilled the eligibility criteria, in which all patients presented symptoms of TMD including LMO, PP, and pre-swelling around TMJ. The available evidence is solely based on case reports, which precludes confirming that cancer metastasis to the TM region elicits symptoms of TMD.
In the included case reports,12, 19, 20, 27–38 all patients (aged between 32 and 78 years) had a history of MBC, which ranged from 30 days to up to 19 years. Moreover, nearly 50% of the case reports did not report the time frame after which symptoms of TMD emerged in patients with diagnosed MBC.19, 27, 29, 32, 34, 35 These results suggest there is no threshold in terms of the initiation of symptoms of TMD, and factors such as patients’ age and duration since the diagnosis of cancer are rather secondary. In all case reports,12, 19, 20, 27–38 a variety of investigations such as two- and three-dimensional imaging and histology were performed to validate the metastasis of MBC into jaw bones. However, from the authors’ perspective, nominating cancer metastasis with TMD symptoms is challenging. It is pertinent to mention that additional factors may potentially contribute toward initiation and progression of symptoms of TMD in patients with cancer. Diagnosis of cancer is a source of anxiety and psychological stress in susceptible contribute towards either initiating and/or aggravating patients, 40 and it is likely that such a diagnosis may TMD symptoms in cancer patients. In the case reports included12, 19, 20, 27–38 in the present study, a history of anxiety or depression was not documented in any of the patients; however, the potential role of such risk factors in initiating and presumably worsening TMD symptoms cannot be overlooked.41, 42 Moreover, it is pertinent to mention that in the included case reports,12, 19, 20, 27–38 there was a paucity of specific diagnostic tests that could have helped with the precise diagnosis of TMD in patients with MBC. Future studies focusing on the precise diagnosis of TMD using standardized methods such as magnetic resonance imaging and arthroscopy in patients with MBC are needed to further comprehend the association between TMD and MBC. Furthermore, laboratory-based investigations such as the assessment of destructive inflammatory cytokines in the synovial fluid of patients with TMD may also help understand the pathophysiological mechanisms associated with TMD in patients with MBC.
In a recent case report, 31 the authors indecently identified a preauricular swelling in a patient with a history of MBC. This suggests that patients with a history of cancer may present with symptomless manifestations, which may elicit dento-facial complications in the future. Likewise, incidental findings in craniofacial regions (such as LMO and pain in the preauricular region) may “hint” at systemic diseases including MBC in undiagnosed patients. It is suggested that in routine oral/dental healthcare settings, patients’ medical histories should be kept dated and vigilantly reviewed by providers prior to facial and/or oral examination/treatment. Ideally, patients presenting with anomalies in the TM region should be referred to operators who have undergone specialized training in the management of TMD; however, general dental practitioners may also be able to manage such disorders at least to an extent by keeping themselves updated through routine continuing education programs. A timely diagnosis and management of TMD can lead to effective palliation and improved patient quality of life.
Most of the case reports included in this evaluation scored 75% or more “yes” on case report checklists, indicating that the studies were of high quality. Despite the fact that the quality appraisal of the included case reports was judged to be of low risk, case reports overall do not provide solid evidence due to several factors, including (a) lack of generalizability, (b) inability to demonstrate a cause-and-effect link, (c) risk of over-interpretation, (d) publication bias, (e) retrospective design, and (f) reader’s attention while focused on the uncommon. 43 Based on such limitations, it is demanding to ascertain an association between TMD and MBC. The authors speculated that longitudinal studies involving patients diagnosed with MBC may assist in evaluating the onset and progression of TMD in these patients; however, from an ethical perspective, such a study seems difficult to execute.
Constructing a systematic review of the subject under investigation proved challenging. This difficulty arose primarily due to the exhaustive literature review, which revealed that the only studies that met eligibility criteria were either case reports or case series. The conventional approach of formulating a patient, intervention, comparison, and outcome (PICO) question, recognized as crucial in systematic reviews, proved impractical given the nature of the included studies. Consequently, this limitation hindered the feasibility of conducting a quantitative evaluation of the included studies. To address these challenges, it is recommended that future research incorporate power-adjusted longitudinal studies to further elucidate the potential association between metastatic breast cancer and temporomandibular disorders. In the interim, based on the existing evidence, it is advisable for patients, particularly females, experiencing temporomandibular disorders to consult healthcare providers to ensure a comprehensive assessment and rule out latent systemic malignancies.
In conclusion, based on the currently available evidence, a direct association between TMD and MBC or vice versa cannot be established. Routine visits to medical and oro-dental healthcare providers can play a role in early diagnosis and management of TMD and MBC.
Footnotes
Authors’ Contribution
FJ designed the study and wrote the manuscript; MSS, MSZ, DM, PER, NC, and KIA wrote the manuscript and revised it prior to submission; MSS, MSZ, and FJ created the tables and figures.
Data Availability Statement
Data is available upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Policy and Institutional Review Board Statement
This study constitutes a mapping review of relevant indexed literature. As a result, formal approval from an institutional review board was unnecessary.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.