
Abstract
Aim:
Effective toothbrushing is the most simple way to maintain a child’s oral hygiene for a cavity-free mouth. Yet, most children find it an uninteresting task and they fail to understand its scientific basis. Augmented reality (A-R)-assisted toothbrushes for pediatric population are commercially available to make toothbrushing interactive, interesting, and educative for the child, aided by gamification providing an interactive videogame platform between the real and the virtual world. The aim of the study was to evaluate the efficacy of A-R-assisted brushing experience of children with respect to fluorescence imaging data and plaque Streptococcus mutans count at clinical and microbiological levels, respectively.
Materials and Methods:
A total of 32 children in the age group of 6-8 years were included and allocated in two study groups (A-R-assisted toothbrushing and manual toothbrushing). Fluorescence-based lesion area scoring was done using FC, Duerr Dental, Vistaproof, Germany. Microbiological analysis of plaque Streptococcus mutans was done to evaluate change in bacterial count. The parameters were recorded again after two weeks. Pre- and post-intervention scores were subjected to statistical analysis.
Results:
Significantly higher reduction of fluorescent scores and mean bacterial count were found in A-R-assisted tooth-brushing group when compared to that of manual toothbrushing.
Conclusion:
Based on the findings of the study, A-R-assisted toothbrushing proves to be an effective tool for motivating and maintaining oral hygiene among children and efforts should be made in incorporating this practice in daily domestic healthcare.
Introduction
Dental caries is at the forefront among various oral health problems affecting children in their growing years. It affects a vast majority of schoolchildren globally, mainly in developing countries resulting in pain, infections, undernutrition thereby affecting growth and development, and decrease in overall quality of life. 1 It is a multifactorial disease that initiates with the formation of plaque biofilm on tooth surfaces with Streptococcus mutans playing the most pivotal role in its progression. Effective toothbrushing to remove daily accumulation of plaque on tooth surfaces to maintain a good oral hygiene is the most simple and straightforward method of controlling caries. 2
However, most children fail to adapt a regular habit of brushing effectively due to lack of interest or knowledge about the consequences. Recent technological advancements have introduced the concept of augmented reality (A-R)-assisted toothbrushes for the pediatric population, which are commercially available to make toothbrushing interactive, interesting, and educative for the child. 3 A-R is a type of technology in which an environment is enhanced through the process of superimposing computer-generated virtual content over real structure, 4 enhancing the sensory perception of reality. 5 A-R and gamification provide an interactive videogame platform between the real and the virtual world through a medium (such as a smartphone), which helps to keep the child entertained and enhances brushing experience. 6 It proves useful for working parents also who may not be able to dedicate time critically to their child’s all-round development. 7 So, the gaming software stores data for the parents to review their child’s progress periodically.
Indices and microbiological assay have been considered by authors as indicators of oral hygiene status and tooth brushing efficiency. 8 Furthermore, newer diagnostic aids like light-induced fluorescence imaging of tooth surfaces or carious lesions have shown promising results and can be considered as an auxiliary non-invasive method. 9
In the current study, we have evaluated the efficacy of A-R-assisted brushing experience of children through the usage of a smartphone application combined with a sensor-assisted toothbrush in terms of a novel method of fluorescence imaging aided by plaque Streptococcus mutans levels, that is, co-relating at both clinical and microbiological levels.
Materials and Method
Study Design and Study Setting
The clinical study is an Experimental non-randomized Concurrent parallel single-blinded design, which was carried out after obtaining clearance from the Institutional Ethical Committee.
Children in the age group of 6-8 years (Frankel Behavior rating of definitely positive and positive) visiting the Department of Pediatric and Preventive Dentistry were included in the study. Table 1 describes the demographic details of the participants. Those with physical/mental disabilities, uncooperative behavior, extensive untreated caries, and undergoing orthodontic therapy were excluded.
Demographic Details of Children.

Methodology
The selected participants along with their parents were explained about the study and enrolled only after getting informed consent from their guardians. The participants were allocated in two groups: Group I (A-R-assisted brushing) and Group II (conventional brushing technique) with a sample size of 16 individuals per group determined using the formula based on the means. The mean values were obtained from the literature. The following formula was used for determining the sample size.
where n = sample size, Zα = constant of 1.96 for two tailed study for confidence level of 95%, Zβ = constant of 0.8 at 80% power of study, S = standard deviation, and d = mean difference.
A briefing of the procedure was done after taking informed consent from the parents. A fluorescence scoring was done by recording an intraoral image with respect to the labial surface of the upper right primary canine for all the participants using a Fluorescent Camera (DuerrDental, Vistaproof, Germany). This intraoral camera color codes bacterial porphyrins on the tooth surface and gives a quantitative value of mean area signifying bacterial activity. 10 Plaque sample was collected from buccal and palatal/lingual surfaces of all teeth with the help of hand scaler and dispensed into Eppendorf tubes. The participants were advised to refrain from eating anything 2 h prior to clinical examination and scoring. Data collection was done during morning appointments. The collected plaque sample was sent to microbiological laboratory personnel who were blinded to the two groups, for determination of S. mutans level in plaque.
Thereafter, participants were educated on oral hygiene practices and brushing technique (Fone’s method). The subjects in Group 1 received a manual toothbrush and a fluoridated toothpaste (Colgate Strong Teeth), while Group 2 subjects received an A-R-based sensor-assisted toothbrush supported with an interactive videogame application (Colgate Magik) downloaded on their parent’s smartphone along with the same toothpaste as of the control group. The virtual environment of the videogame guides the user to brush efficiently covering all tooth surfaces following a particular pattern for a specified time. As the child finishes the task, his progress is stored in the application and he gains points to move to the next level.
The participants were advised to follow the brushing techniques two times daily for 15 days. At the end of 15 days, the participants were called for follow up to assess their fluorescence values and plaque S. mutans count again.
Laboratory Method
The samples were collected aseptically in pre-weighed sterilized Eppendorf tubes. The tubes were weighed again after the collection of sample. One milliliter of physiological saline was added to the tube containing sample and thoroughly mixed. The sample was then serially diluted up to 10-4 dilution. The sample was then spread on Sanguis mutans agar medium. The plates were incubated in an anaerobic condition at 37° for 72 h. After incubation, the plates were observed for S. mutans colonies and CFU were recorded.
Statistical Analysis
The data obtained pre- and post-intervention was entered into excel sheets. All the analyses were performed using SPSS ver 26.0 (IBM Corp. USA) and the statistical significance was tested at 5% level.
Results
The difference between two groups at each time point was performed using t-test for independent samples, while the pre-post comparison within the group was carried out using paired t-test. The bacterial count data was log-transformed and the pre-post comparison was performed using paired t-test. The change in the bacterial count from pre- to post-stage was compared between two groups using t-test for independent samples. Figure 1 describes the comparison of fluorescent images before and after the practise of AR asssited tooth brushing.
Abbreviation: A-R, augmented reality.
Table 2 and Figure 2 provides the comparison of fluorescent value between two groups at pre- and post-intervention stages. The mean fluorescent value at pre-intervention stage differed non-significantly between two groups (p = .644); however, post-intervention, the mean for TEST group (25081.31 SD: 9469.63) was significantly lower than that of CONTROL group (58094.38 SD: 26855.41), as indicated by a p-value < .0001.
Comparison of Parameters Before and After Intervention in Each Group.
Column Chart Showing Mean Fluorescent Value for Children in Test and Control Groups at Two Time Points.
Table 3 shows the mean bacterial counts (log-transformed) before and after treatment in each group. In the experimental group, the mean before treatment was 4.89 (SD: 0.19), while after treatment was 4.61 (SD: 0.19), and the mean difference between two times was statistically significant (p < .0001). Similarly, in the control group, the mean log-count before treatment was 4.9 (SD: 0.21), while after treatment was 4.74 (SD: 0.23), and the mean difference was statistically significant (p < .0001).
Comparison of Mean Bacterial Count (Log-transformed) within Groups.

Figure 3 shows the comparison of mean change of bacterial counts before and after treatment in two groups. The difference of mean change between two groups was statistically significant with a p-value of .023.
Column Chart Showing Mean Change of Bacterial Counts, Before and After Treatment, in Two Groups.
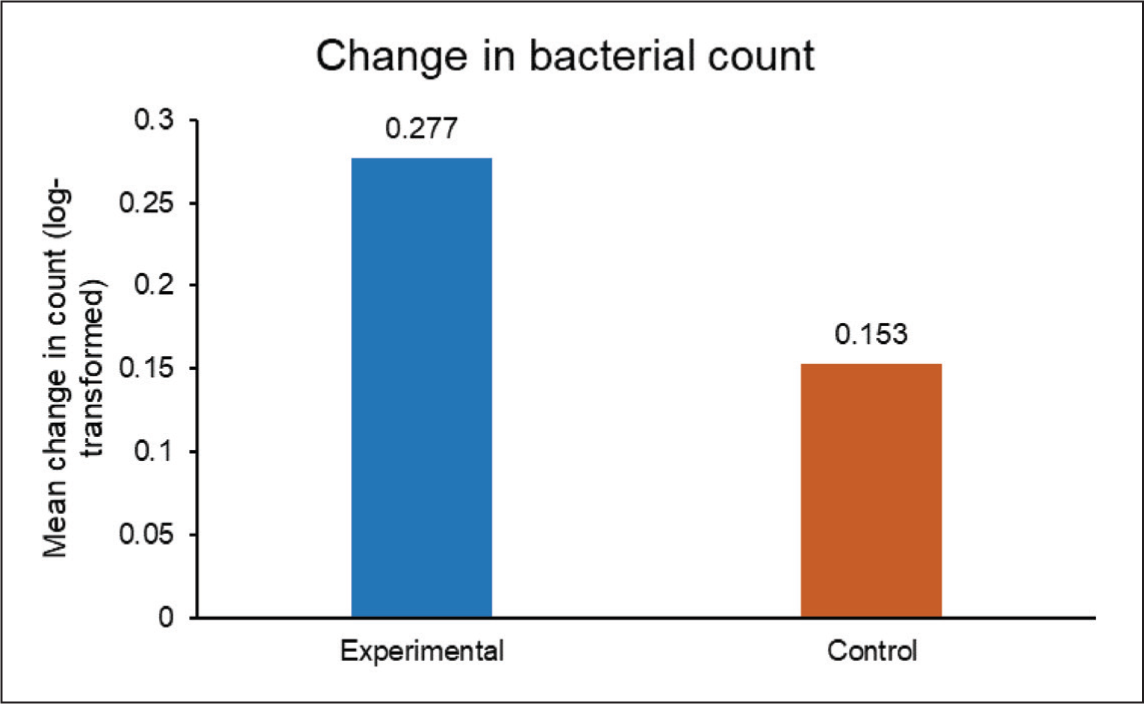
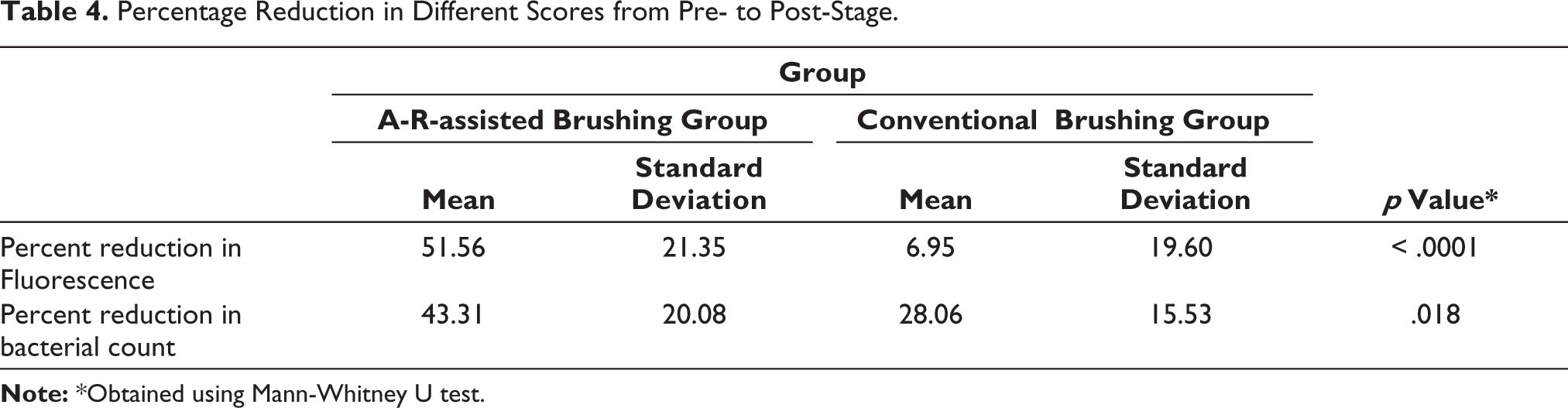
Table 4 shows significantly higher percentage reduction of the scores in A-R-assisted brushing group was obtained as compared to conventional brushing group.
Percentage Reduction in Different Scores from Pre- to Post-Stage.
Discussion
Prevention is a major health priority for the pediatric population. Effective toothbrushing is the most common and simple way to maintain one’s oral hygiene and have a cavity-free mouth. Yet, for most children, this becomes a task as they find it uninteresting and fail to understand its scientific basis. 11 Inculcating this activity during the formative years in a child is of utmost importance to prevent and avoid the complications associated with dental caries. Children have a short attention span when it comes to oral hygiene practices and usually require guided supervision. Average brushing time manually in children from 3 to 11 years age was found to be 36 sec in a study by Mentes et al. 12 Even if some children adapt the habit, they may fail to clean all surfaces of the teeth due to lack of awareness. 13 Therefore, oral health education becomes an essential part of a growing child’s curriculum to make them understand its importance and adapt appropriate measures of maintaining oral hygiene from their early years. Thus, in our ever-expanding technological world, the boon of A-R can be utilized in this context. 14 The A-R-assisted toothbrush linked with the videogame guides and reinforces the correct movement of the brush in all areas and functions for an ideal brushing time period. The application keeps a log of the duration of time spent in executing the activity daily so that parents are able to keep a track of the frequency and duration their child has spent on brushing. The motion sensor unit ergonomically advises the child on areas such as the correct posture to assume during the activity, how to effectively grip the toothbrush, ideal angulation of the toothbrush, and speed of brushing.
The chosen age group of 6-8 years gives an advantage as children start to adapt motor skills during this time, while also showing signs of cognitive development. 15 So, this becomes an ideal period for them to adapt a learning activity through daily practice and instill it in their conscience as a routine habit. A follow-up period of two weeks provides adequate time for measurable plaque build-up without much wear of the bristles of the toothbrush. 16 A-R combines real and virtual objects in a single environment, runs interactively in real time, and it registers virtual and real objects reciprocally. 17 A-R has been commercialized and widely used in different industries such as retail, real-estate, academics, and healthcare although gaming remains as one of its primary applications. 18 The term “Augmented reality” was originally coined by Caudell and Mizell during 1990s but its origin dates back to the time of World War II, while the first system recognized as A-R was in 1968. 19 Apart from its applications in various medical and surgical fields, A-R has also found to be useful in the treatment of psychologic disorders, cognitive impairment, and motor rehabilitation.20,21 Kwon et al. wrote about advent of A-R in various fields of dentistry and in dental education. 22 A study on “intelligent toothbrush” using a vision-based toothbrush tracker was done on adult and geriatric patients with conditions like dementia. 23 Another study showing that training of A-R-assisted smart toothbrushing for the intellectually disabled can be beneficial was also done recently. 24 In another survey, Kanoute et al. assessed the quality of different mobile game applications currently available that are linked to oral hygiene measures for children through a survey among oral health professionals who recommended their use and rated them positively. 25 A recent study investigated the usage of a smartphone app for improving manual toothbrushing via a gravitation sensor by measuring the plaque and gingival indices through a randomized controlled trial, showing promising results. 26 Similarly, comparison of A-R-assisted toothbrushing via a mobile app with manual brushing was done among 247 children by assessing plaque scores and Visual biofilm index by Desai et al. 27 and measuring toothbrushing duration and distribution by Jacobson et al. 28
However, to the best of our knowledge, none of the recent studies have evaluated microbiological evidence of bacterial load reduction via A-R-assisted toothbrushing with a supporting fluorescence data added as a measurable outcome. Bacterial lesions fluoresce differently from healthy tissues when excited by light in specific wavelengths. The Vista Proof fluorescence camera uses GaN LEDs that emit blue light at 405 nm on the teeth surface that stimulate porphyrins in bacteria. 29 This will help in co-relating the qualitative data with the quantitative findings. Also, a recent study on the effectiveness of chewable toothbrushes has assessed the outcome based on reduction in salivary S.mutans level. 30 According to literature, fluorescent-based optical systems are capable of improving diagnosis of “hidden caries.” 31 In our results, there was significant reduction and higher differences in bacterial load and fluorescent lesion area in the A-R-assisted group compared to the conventional brushing group. The conventional brushing group showed a slight improvement in the scores, whereas the A-R-assisted group showed significantimprovement compared to their first scoring sessions.
Although the study shows favorable results, it involves some limitations. Accessibility and understanding of the product and technology seem to benefit only a particular economic section of the society. Individuals from lower socio-economic background may find difficult in affording or understanding the instructions and usage. The facility will be limited only to smartphone users. The sample of participants may not be representative as this as a pilot trial conducted to test the efficacy of fluorescence imaging asa novel technique for assessing A-R-assisted brushing. Also, a longer follow-up period may provide a clearer idea about its acceptance among users. However, considering all these factors, we can still anticipate a good patient acceptance of this technology as it is attractive and enjoyable for the child and indirectly educative to help them learn correct toothbrushing method. Even if the application use is discontinued, the technique learnt remains instilled in their conscience through practice and a positive outcome can be expected through future research in this field using different variables.
Conclusion
Based on the findings of the study, A-R-assisted toothbrushing proves to be an effective tool for motivating and maintaining oral hygiene among children. Incorporating this practice in daily domestic healthcare will yield positive results in encouraging children and help them to adapt effective toothbrushing as a regular habit. Further studies are needed to yield a clearer picture on various outcomes of A-R-assisted toothbrushing.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance (ref: JSSDCH IEC/ 61/2022) was obtained from the Institutional research board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.