
Abstract
Aim:
The aim of this study was to evaluate trauma from occlusion in patients undergoing orthodontic treatment through assessment of fremitus, pocket depth, gingival biotype, and occlusal contacts pre-orthodontic treatment (T0) and post-orthodontic treatment (T1).
Materials and Methods:
This prospective randomized trial included 40 participants selected based on a simple random sampling method, of which 27 were women and 13 were men with ages ranging from 25 to 40 years. All the participants were clinically checked for gingival recession, fremitus, pocket depth, gingival biotype, and occlusal contacts obtained via digital intraoral scans and fed to 3Shape software to perform the occlusal mapping analysis for pre-orthodontic treatment (T0) and post-orthodontic treatment (T1). T-Scan occlusal analysis was performed to check the force levels pertaining to each tooth. A paired t-test was done to find out the changes in fremitus, pocket depth, gingival biotype, and number of occlusal contacts between T0 and T1.
Results:
Results of paired t-tests showed a statistically significant difference for fremitus between T0 and T1 (p < .05). Gingival biotype and pocket depth did not show any improvement post-orthodontic treatment (T1) (p > .05). Number of traumatic occlusal contacts reduced at T1 for incisors and canines showing a statistically significant difference between T0 and T1 (p < .05).
Conclusion:
Orthodontic treatment helps in relieving the traumatic occlusal contacts, especially in the incisors and canine regions. As the teeth are relieved from traumatic occlusal contacts, fremitus also has shown to have drastically improved at the end of orthodontic treatment. Gingival biotype and pocket depth might take a longer time to regenerate and improve, which requires long-term observation.
Keywords
Introduction
Trauma from occlusion (TFO) has been defined as periodontal injury resulting from occlusal forces that exceeds the reparative capacity of the attachment apparatus. 1 Traumatic occlusal forces were considered the preceding cause of periodontal disease. 2 According to Glickman and Smulow, 3 excessive occlusal forces, particularly pressure, could be a factor in the etiology of infrabony pockets and angular bone loss by an altered path of gingival inflammation and periodontal bone loss. Traumatic occlusal forces can be acute or chronic depending on the duration of the aberrant occlusal force imposed onto the teeth.
TFO deteriorating periodontium shows various signs that help in early diagnosis. The most common sign of TFO is tooth mobility.4,5 Fremitus is another symptom where the opposing tooth exhibits a palpable vibration when subjected to occlusal forces. 6 Pain in the masticatory muscle area and wear facets if noticed should give a sign of occlusal disharmony leading to the habit of bruxism and temporomandibular joint problems. Increased probing pocket depth (PPD), loss of clinical attachment level, absence or widening of periodontal ligament, discontinuation or absence of lamina dura, bone loss in the region of trauma, and gingival recession are the radiographic signs of TFO.7–9
TFO in orthodontics should be diagnosed and treated as early as possible to prevent further deterioration of the periodontium. Orthodontic treatment results in changing the positions of teeth by tipping or by bodily movement, which can give rise to occlusal discrepancies that are only temporary. Lighter orthodontic forces when applied and dissipated slowly cause no harm to the affected tooth from TFO. 10 A case report by Thierens et al. 11 showed that a maxillary central incisor that was periodontally affected by TFO was reversed to normal with reduced PPD and recession decreased after 12 months of orthodontic treatment. This gives an insight on orthodontic treatment also being therapeutic to eliminate symptoms of TFO.
This study focuses on the orthodontic treatment in decreasing the harmful effects of TFO by comparing the signs such as fremitus, PPD, gingival biotype, and occlusal contact changes pre-orthodontic treatment (T0) and post-orthodontic treatment (T1). The null hypothesis of the study is that there is an improvement in the signs of TFO post-orthodontic treatment (T1). An alternate hypothesis of the study is that there is no difference between T0 and T1 regarding the signs of TFO.
Materials and Methods
Setting and Design
The study was approved by the Institutional Human Ethical Committee of Saveetha University with the approval number of IHEC/SDC/ORTHO-2001/20/575. A total of 40 participants were included in the study 27 women and 13 men of age 25–40 years reporting to the outpatient department of orthodontics of Saveetha Dental College, Chennai. The study was started in September–October 2020 and completed in March–April 2022.
Sampling Criteria
The participants reported to the department were screened for signs and symptoms of TFO in the upper and lower anteriors by the primary investigator. Patients with debilitating disease, progressive periodontal disease, gingival recession or periodontal conditions, tooth mobility due to periodontal disease, anterior or lateral open bite conditions, and temporomandibular joint disorder (TMD) not pertaining to traumatic occlusion such as stress or psychological problems as a cause for TMD, systemic conditions leading to periodontal problems, postmenopausal women were excluded from the study. Participants of age 18–45 years, both men and women, with gingival recession, deep bite, and anterior crossbite due to traumatic occlusion were included in the study.
Abiding to the inclusion criteria, initially 42 participants were selected. On the calculation of sample size with G*Power 3.1.9.4 software (Germany) with a significance of less than 5% (<0.05) and a power of 90%, we arrived at a sample size of 40. Finally, 40 participants were recruited to take part in the study by random selection process. Written and informed consent was obtained from all the participants of the study.
Methodology
Clinical examination of all the participants was done by the clinician (primary investigator). Eligible participants were provided orthodontic treatment by an orthodontist who was not a part of the trial. Of the 40 patients, 23 underwent non-extraction treatment 17 underwent extraction treatment and all of them were either average or high-angle patients. With regard to bracket prescription, all the patients were given Mclaughlin Bennet and Trevisi (MBT) prescription, and only friction mechanics were used to avoid bias. All the first and second molars were bonded as molar bands would interfere with T-scan recordings. Fremitus, gingival biotype, PPD, gingival recession, and occlusal contacts were recorded for each participant before starting orthodontic treatment (T0) and after completion of orthodontic treatment (T1) with the mean orthodontic treatment duration of 12–18 months. The obtained values were recorded in Excel spreadsheets.
Fremitus was checked in the upper anterior region by placing the index finger on the facial surfaces of maxillary anterior teeth during repeated habitual centric closure. 12 This helped to evaluate the functional mobility of the teeth during mastication. Fremitus if present was recorded as “yes” and if absent was given as “no” while entering in the spreadsheet.
Classification of gingival biotypes by Fu et al. 13 was applied in this study categorizing the gingival biotypes into two types as “thin” (probe seen through the gingiva) and “thick” (probe not seen through the gingiva). This probe transparency method is minimally invasive and has good accuracy. William’s Periodontal probe (Polodent, India) is inserted into the sulcus of the midfacial aspect of the tooth and checked for transparency of the probe and identified as thin or thick biotypes.
PPD according to the Community Periodontal Index of Treatment Needs (CPITN) is categorized as pocket depth of 0–3 mm as no/mild periodontitis, at least one pocket ≥4 mm and <6 mm as moderate, and with at least one pocket ≥6 mm as severe periodontitis. 14 William’s periodontal probe with markings 1, 2, 3, 5, 7, 8, 9, and 10 mm markings were used to record the PPD. The probe was inserted into the sulcus in the mesial, distal, midfacial, and lingual/palatal sides of the traumatized tooth. The greatest pocket depth recorded from all four regions is taken as the average PPD value for that particular tooth. The PPD recorded is entered in the Excel spreadsheet.
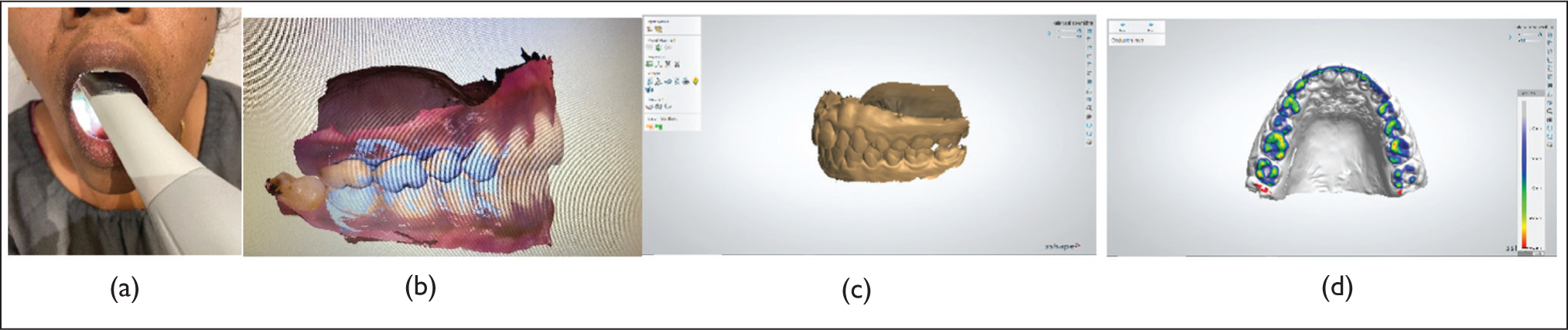
To evaluate the occlusal contacts, intraoral scans at T0 and T1 were recorded, using TRIOS 3Shape intraoral scanners, in Copenhagen, Denmark. The intraoral scanning of the teeth was done starting from the second molar on the left to the second molar on the right covering the labial, buccal, and palatal/lingual sides of the upper and lower arches. Finally, the patient is instructed to bite and the left and right-side occlusion is recorded. Any incomplete portion is rescanned to avoid any errors in the models. The scanned models were imported to 3Shape OrthoAnalyzer dental system software to perform the occlusal mapping analysis (Figure 1). There is an option in the software to perform the occlusal mapping analysis which has an occlusal map available in a scale of different spectrum of colors amounting to the distance from the surface of the tooth to the opposing tooth in the opposing arch. This helps to find the teeth in traumatic contact represented by the red color spectrum of the scale to the teeth with the least traumatic contact that is shown as the gray to white scale spectrum in the map. To measure the red-colored occlusal contact areas manually on digital models, the image analysis software Image J (version 1.52a for Macintosh, National Institutes of Health, Bethesda, MD, USA) was used. The images were taken from 3Shape separately for all teeth and calibrated to the imaging software Image J with the distance measured between two points in mm dimensions. The outlines of the occlusal contact areas were traced using the freehand preselection tool using the computer mouse, and the Image J program will automatically calculate the traced area in mm 2 dimensions. The occlusal contact areas averaged for incisors, canines, premolars, and molars were tabulated.
(a) Intraoral Scanning Using 3Shape Scanner System. (b) Digitally Scanned Occlusion Obtained from the Patient Will Appear on the Viewer Screen. (c) Obtained Occlusion Is Transferred to 3Shape OrthoAnalyzer Software to Perform the Occlusal Mapping. (d) Digital Models Undergo Occlusal Mapping Analysis.
Observational Parameters
After occlusal mapping of the digital scans, participants underwent T-scan Digital Occlusal analysis to quantify the extent and timing of forces acting on distinct teeth as well as the stability of the occlusal contact of the overall bite. Digital quantification of bite forces was recorded using T-scan Novus sensors (TEKSCAN, Inc., Boston, MA, USA). Recent investigations on articulating paper have shown that the markings on the paper are not accurate markers of different occlusal force levels.15,16 Using the T-scan system both static and dynamic movements of the jaw can be recorded. The participant was seated upright in the dental chair chicagosoftware package with real-time data on occlusal contact and force. These data are shown as a continuous force “movie” of the whole acquired occlusal contact event in both two and three dimensions.
Statistical Analysis
All the recorded values were entered in an Excel spreadsheet and imported to SPSS software version 23.0 (IBM, Chicago, IL, USA) with a significance of 5% (0.05), a confidence interval, and power (1 – β) of 95%. A paired t-test was done to find the difference in fremitus, gingival biotype, PPD, and occlusal contact changes between T0 and T1.
Results
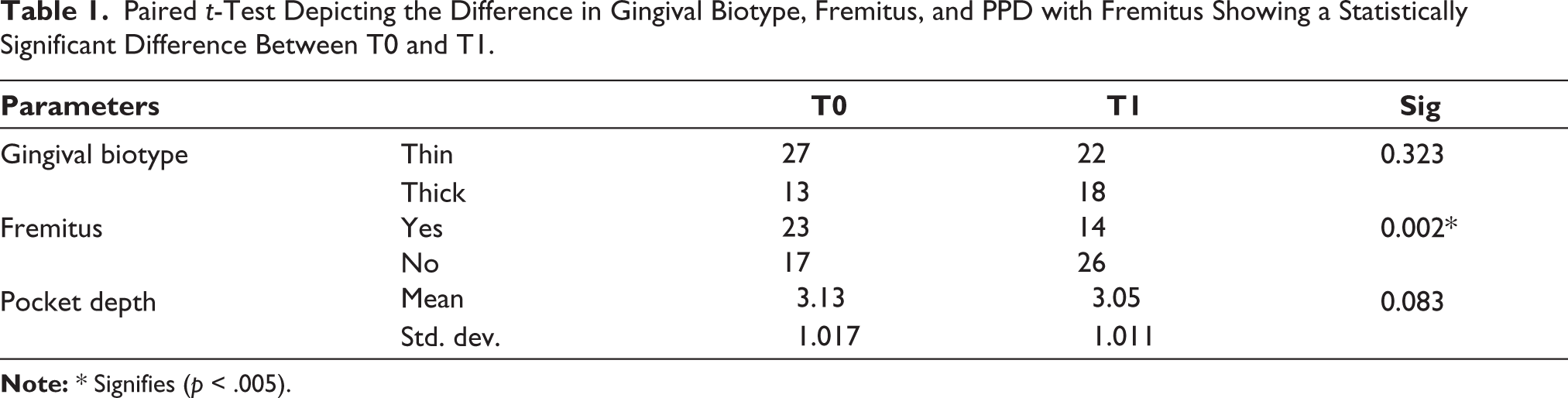
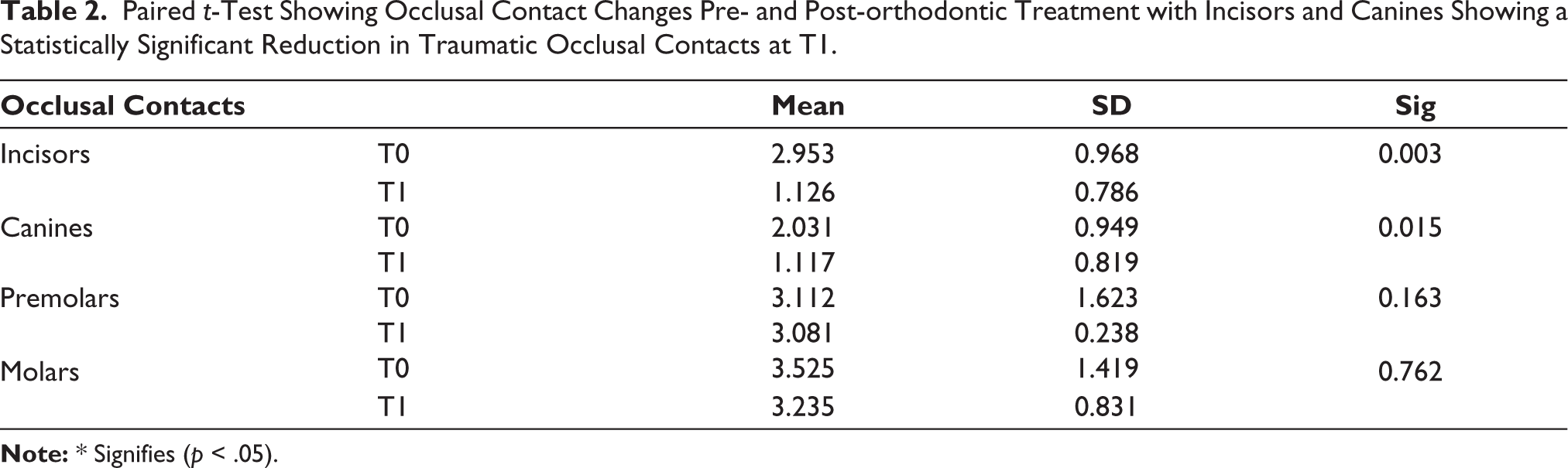
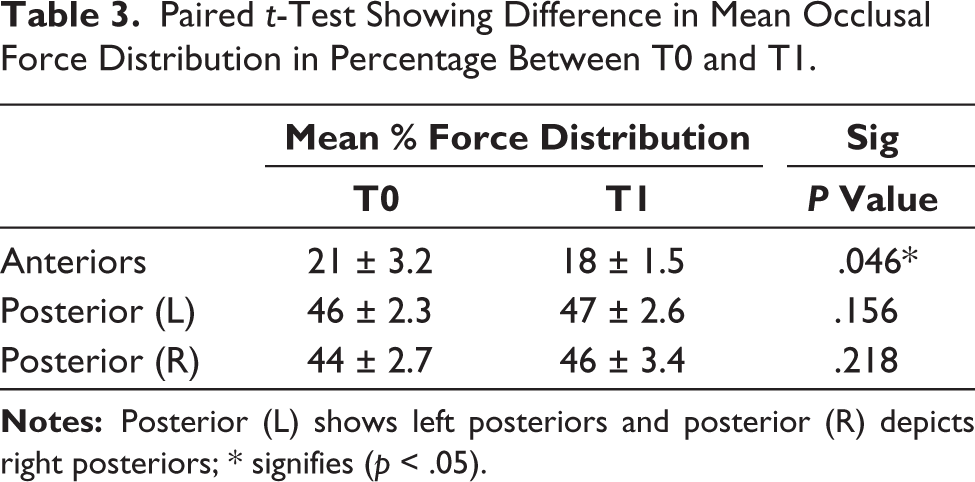
A paired t-test done for determining the changes in the gingival and occlusal parameters assessed at T0 and T1 showed a statistically significant difference for fremitus (p < .05) which decreased at T1 in most of the participants (Tables 1 and 2). At T0, 23 participants were found to have fremitus in the upper incisor region which in T1 was reduced in only 14 participants, so this means 9 participants did not have fremitus at T1. PPD and gingival biotypes did not show much of difference at T1 as out of 27 participants who had thin gingival biotypes at T0 in the tooth which had a gingival recession or a traumatized tooth, 22 of them still had the same thin gingival biotype at T1 showing insignificant difference (Table 1). Occlusal contact changes showed a statistically significant difference in the reduction of traumatic contacts in the region of incisors and canines (p < .05). Molars and premolars did not show a significant difference at T1; however, there was a reduction of traumatic occlusal contacts although insignificant (Table 2). Difference in occlusal force distribution shows a statistically significant difference in occlusal contacts between T0 and T1 for anteriors (p < .05) (Figure 2 and Table 3).
Paired t-Test Depicting the Difference in Gingival Biotype, Fremitus, and PPD with Fremitus Showing a Statistically Significant Difference Between T0 and T1.
Paired t-Test Showing Occlusal Contact Changes Pre- and Post-orthodontic Treatment with Incisors and Canines Showing a Statistically Significant Reduction in Traumatic Occlusal Contacts at T1.
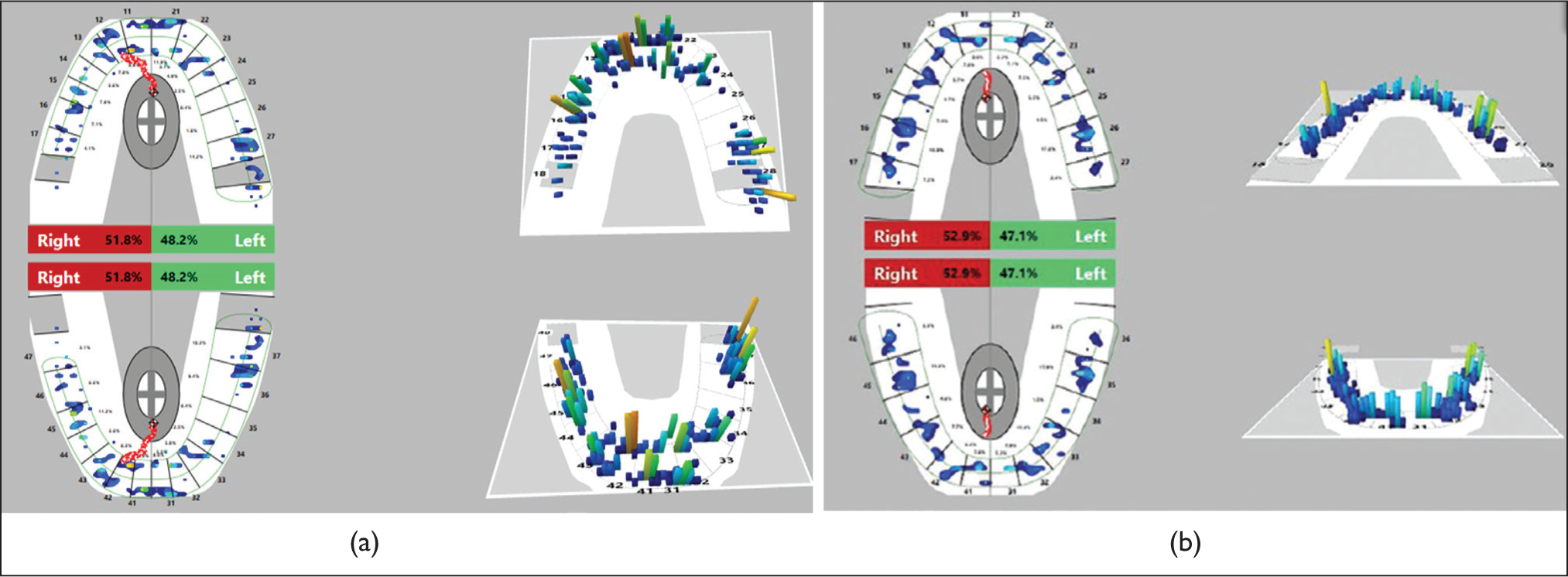
Paired t-Test Showing Difference in Mean Occlusal Force Distribution in Percentage Between T0 and T1.
Discussion
TFO being an important factor that is to be focused upon, especially for an orthodontist is never to be ignored and should be treated at the earliest with continuous monitoring during the treatment. According to Saravanan et al., 1 before debonding of brackets the clinician should make sure that there are no occlusal interferences both in static and functional excursions, and also during the retention period, retainers should be customized according to the initial malocclusion and periodontal status of the patient.
According to the results of our study, a statistically significant difference was observed for fremitus accounting for approximately nine participants who had been detected with absence of fremitus post-orthodontic treatment (T1). This shows that orthodontic treatment has effectively worked in reducing the traumatic occlusion thus preventing further deterioration of the supporting structures. Also, in this study not all the 40 participants were detected with fremitus, it was only 23 participants who did have fremitus although they had a traumatic occlusal contact that was proven with further clinical diagnosis and occlusal mapping. Of the 23 participants, 14 of them still had fremitus at the end of the orthodontic treatment (Table 1). According to a study by Kundapur et al., 12 fremitus was associated with gingival recession in almost 59.1% of patients and was not significantly related to gingival recession. The results of our study show that the fremitus may or may not be eliminated after orthodontic treatment, thus helping in the reduction of TFO and not completely eliminating it.
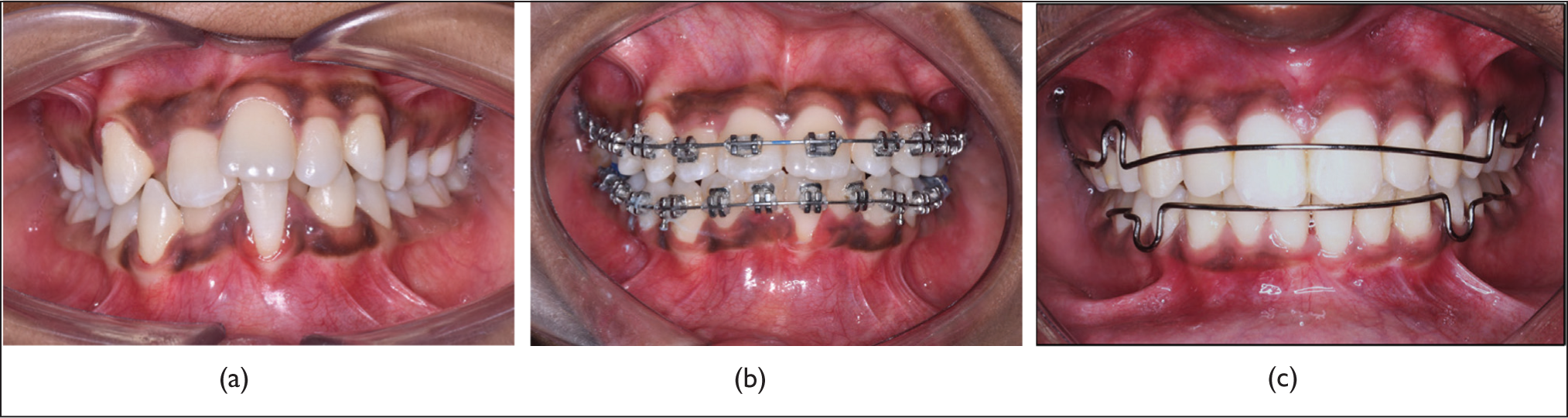
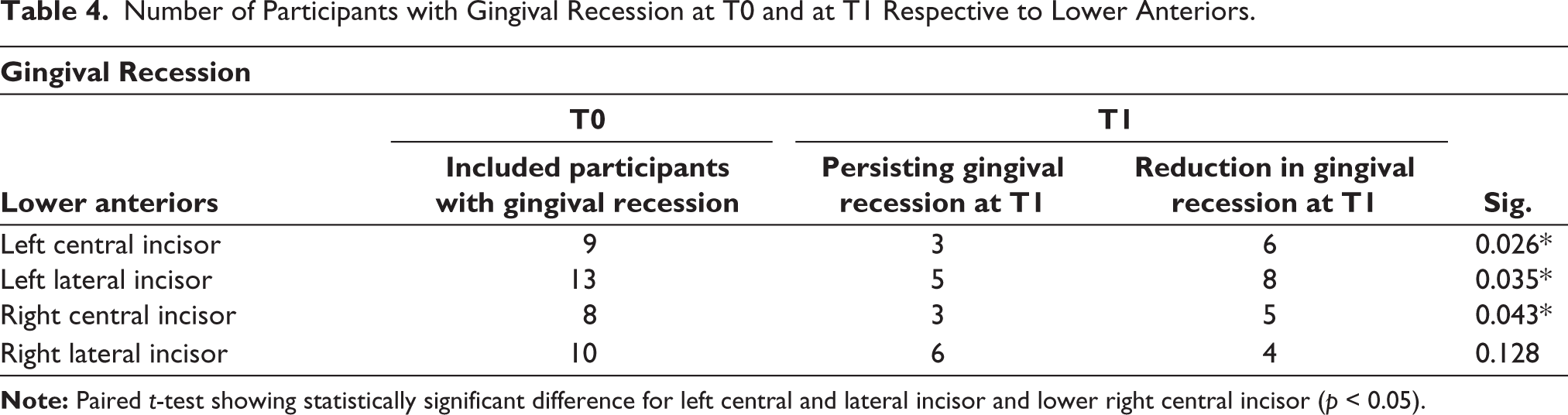
Gingival biotype of lower anteriors was thin for almost 27 participants and thick for 13 participants which after orthodontic treatment showed that five participants had their gingival biotype reversed to normal from a thin biotype and the others did not have any difference at T1 (Table 1). A systematic review by Amid et al. 17 studied the effects of orthodontic treatment on the periodontium and concluded that orthodontic treatment did have some mild detrimental effects on the periodontium especially in patients with thin gingival biotype. From Figure 3a–c, it is observed that the loss of gingival keratinization and thin gingival biotype with respect to the traumatized left central incisor has not reversed at the mid as well as post-orthodontic treatment (T1). Gingival recession with respect to Table 4 shows a significant reduction in gingival recession in most of the participants with respect to lower left and right central and lateral incisors except for lower right lateral incisor. Although there is a reduction in gingival recession with respect to the elimination or reduction of traumatic occlusion, the biotype did not improve in most of the patients. Average gingival recession observed in included participants with traumatic occlusion in lower anteriors ranged from 1 mm ± 0.25 to 2 mm ± 0.69. We could observe only an improvement with respect to recession of gingiva but it was not completely reversed back to normal gingival architecture at the end of the treatment in almost all the participants. The results of this study showed that it may take a longer time for the reversal of normal gingival biotype after completion of orthodontic treatment which requires longer follow-up.
(a) Pre-orthodontic Treatment (T0). (b) Six Months After Orthodontic Treatment. (c) Post-orthodontic Treatment (T1).
Number of Participants with Gingival Recession at T0 and at T1 Respective to Lower Anteriors.
With PPD, no significant difference was observed between T0 and T1. Although the participants included in the study had an average or close to average pocket depth which was gauged according to CPITN. An average of 3.13 mm was observed from the mean of 40 participants at T0 and a decrease in PPD to 3.03 mm was observed at T1, although there was not a significant difference (p > .05). Huang et al. 18 conducted a retrospective study of orthodontic treatment on anterior tooth displacement caused by periodontal disease and concluded that orthodontic treatment proved to be beneficial in reducing pocket depth. There is a fluctuance within the normal range of pocket depth in our study, hence future studies should be undertaken with PPD much more than the average PPD to observe significant changes.
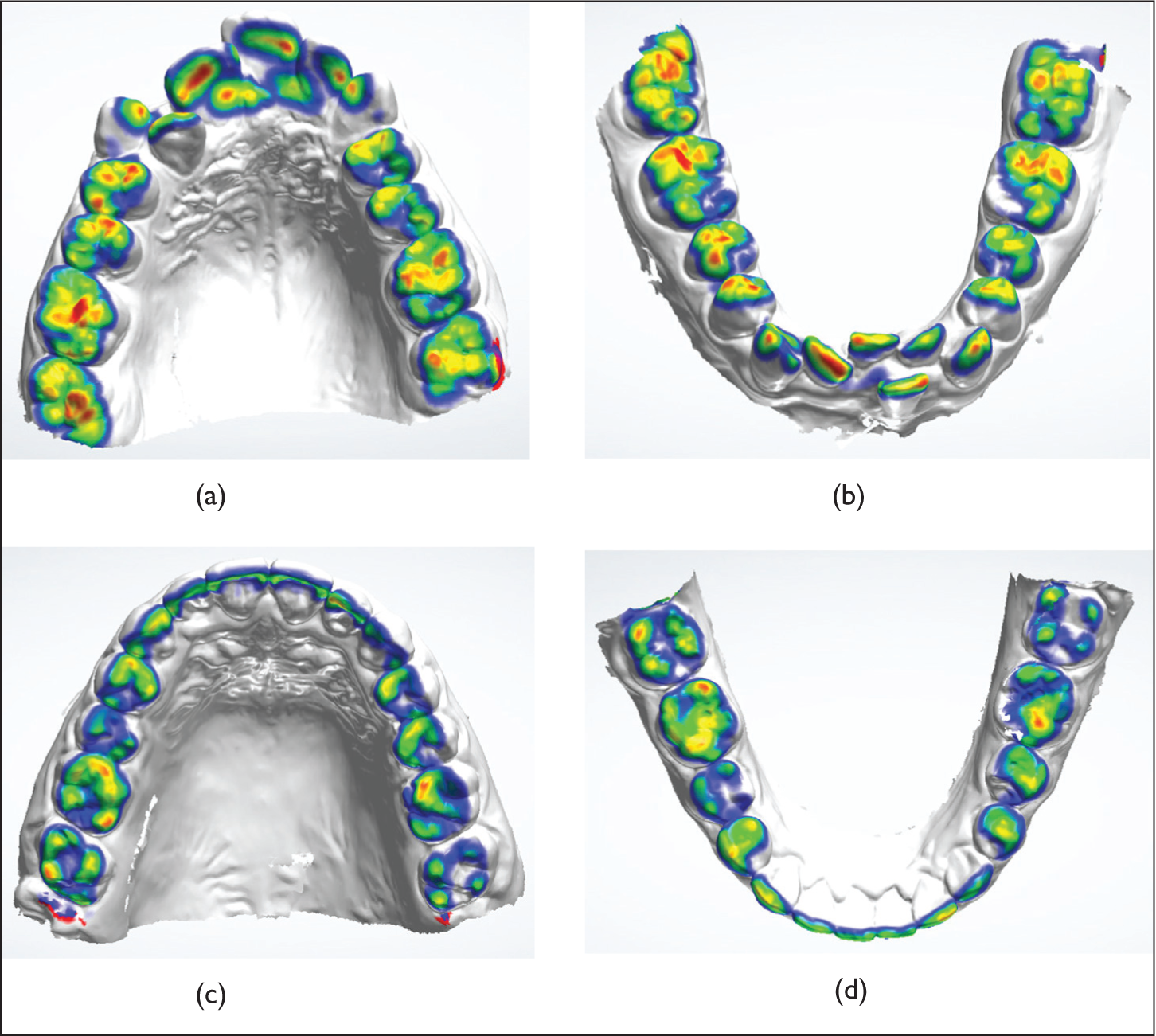
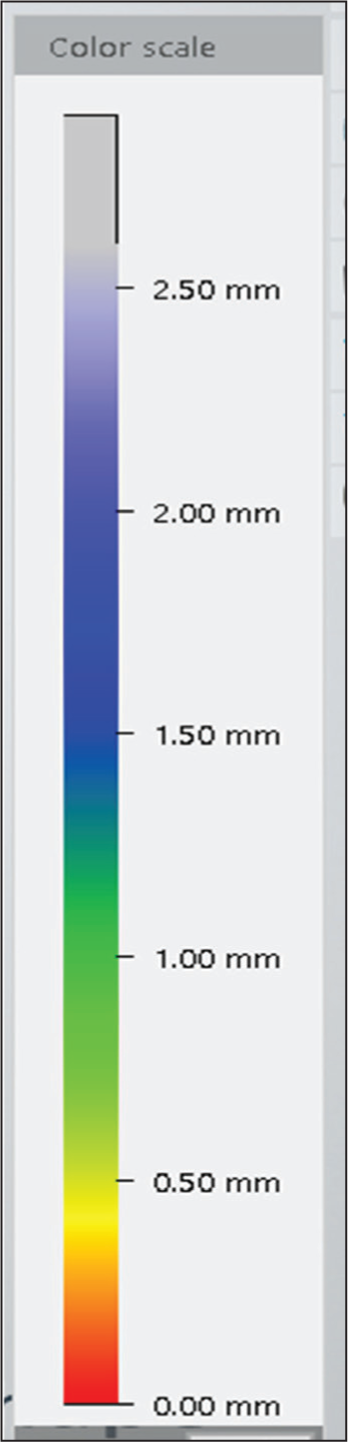
When coming to the number of occlusal contacts, a statistically significant difference was observed only for incisors and canines (p < .05). Color-coded Occlusal mapping of all the xmodels was obtained. The more the redder areas seen on the models, the greater the traumatic occlusal contact (Figure 4). The interocclusal distance between the maxillary and mandibular model corresponds to the color indicated in the scale (Figure 5). It can be calibrated to a distance of 0.5 mm or 1 mm or 2 mm according to the preference. Figure 4 shows that the red areas observed in pre-treatment models were reduced in the models obtained post-treatment (T1). This proved the improvement in the occlusal contacts obtained after completion of orthodontic treatment. Also, in the entire pretreatment model scans obtained almost all the participants were found to have the highest number of red areas in the incisor and canine region when compared to that of premolar and molar regions. This showed that traumatic occlusal contacts quantitatively reduced at T1, especially in incisors and canine regions. In a study by Deng et al., 19 there was improvement in occlusal contacts post-orthodontic treatment which showed a reduction in the mean number of occlusal contacts resulting in orthodontic treatment being effective quantitatively and quantitatively in TMD patients.
T-scan analysis helps in interpretation of relative occlusal loading of force at each contact. Each bar’s color and height quantify the amount of force applied during each contact. The occlusal load magnitude is color coded; the greatest force is shown in red, whereas the smallest force is blue. 20 From Figure 2 and Table 3, force distribution in the anteriors has reduced in T1 when compared to T0; however, the occlusal force distribution of posteriors has increased in T1 from T0. But when compared to anteriors, the posteriors have greater root surface to withstand oblique, transverse, and vertical forces if the supporting periodontium is in good condition to allow the forces to be dissipated over their occlusal table, taking into consideration the forces not exceeding the tolerance capacity of the periodontium. From the results of this study, there is only minimal change in force distribution of posteriors which may not be considered harmful to the periodontium. The concern for TFO is the anteriors which showed an improvement in T-scan values thus showing reduction in occlusal forces overcoming the traumatic occlusal contacts.
According to the combined results of our study, fremitus is eliminated once the traumatic occlusal contacts are relieved. Although a greater number of participants did show a negative fremitus at the end of orthodontic treatment it was not reflected in all the participants. This indicates that not all patients with TFO will have fremitus (as few participants did show negative fremitus at T0) and it is not definite for the patients with TFO to have negative fremitus after orthodontic treatment, although significant results were obtained in the study. Gingival biotype and PPD requires long-term follow-up of participants as reversal of original architecture might take a longer time than expected and the results might not have been favorable as our duration of study is shorter (2 years) to expect a normal periodontal attachment apparatus. The mean gingival recession in relation to lower anteriors showed a greater improvement at T1 except for right lateral incisors. TFO deterioration according to T-scan showed a good reduction in anterior traumatic contacts and increased in posteriors. In our study, most of the participants who underwent T-scan at T0 were found to have increased TFO in anteriors and very minimal TFO in posteriors. This was vice-versa at the end of T1. This could be attributable to variable mechanics used in orthodontic treatment arch alignment and corrections in three dimensions. Efficiency of the orthodontist, orthodontic biomechanics, and growth pattern of the individual participant does have an influence over the TFO in posteriors.
Thus, orthodontic treatment greatly improves the occlusion by eliminating or reducing harmful traumatic contacts, especially in the anteriors. Null hypothesis is accepted for only certain parameters assessed in the study (fremitus, TFO occlusal contact analysis, and gingival recession). Limitations of the study include a very small sample size to be generalized to a larger population. Future studies should focus on a larger population and longer follow-ups for more stable results.
Conclusion
Orthodontic treatment helps effectively in eliminating or reducing the fremitus, gingival recession, and traumatic occlusal contacts qualitatively and quantitatively in the anterior region. Long-term observation is necessary to observe changes in PPD and gingival biotype.
Footnotes
Acknowledgements
I would like to acknowledge the effort of my co-author to get involved in interdisciplinary research topics involving matters of concern for orthodontic purposes.
Authors’ Contribution
K.K.S.S. contributed to the study design, manuscript correction, and formatting of the paper. S.D. contributed to study execution, data collection, data analysis, and manuscript preparation. K.K.S.S. contributed to data analysis. All authors have made substantial contributions to this study, and all have reviewed the final paper before its submission. Finally, all authors have given approval for publication.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author (Sowmithradevi S, E-mail:
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Human Ethical Committee of Saveetha University with the approval number of IHEC/SDC/ORTHO-2001/20/575.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors had obtained all appropriate patient consent forms. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed. This study was held in Saveetha Dental College, Saveetha University, Chennai, India.