
Abstract
Background:
For its synergistic effects in producing skeletal changes as well as to lessen the proclination of the lower incisors, which is a common negative result of mandibular advancement, fixed functional appliances with skeletal anchorage have recently been used.
Aim:
Objective was to evaluate the skeletal and dentoalveolar effects with fixed functional appliances with and without skeletal anchorage.
Methods:
Electronic database search and manual search were performed up to 2021, April in four databases namely The Cochrane Library, PubMed, Lilac, and Google Scholar. RCTs that employed the use of fixed functional appliances in Class II malocclusion with and without skeletal anchoring were collected. Two co-authors independently extracted the data, and a pre-designed template was followed during the data extraction process. Data including inclusion and exclusion criteria; study design, the year of publication; age and gender of the patients; type of fixed functional device; stage of skeletal maturation; size and site of mini-implant or miniplate placement, amount of force applied in grams or Newtons; method of study outcome assessment (2D or 3D); and follow up were collected. The skeletal and dentoalveolar parameters were extracted.
Results:
The risk of bias was evaluated, and the SMD and 95% confidence intervals (CIs) were also calculated. Four RCTs were evaluated for qualitative and quantitative analysis. The review involved data of 179 Class II individuals. The results of a random-effects meta-analysis showed that the SNB differed significantly from the control group (SMD = 0.50 (95% CI –1.55 to –0.10)). No significant differences noted between the two groups in terms of lower incisor inclination and mandibular length changes [SMD = –0.04 (95% CI −2.06 to 1.98) and –1.33 (95% CI −3.28 to 0.62), respectively]. The studies under this were not able to provide enough data to draw any conclusions about the effects of using skeletal anchorage with FFA.
Conclusion:
According to the evidence that is currently available, using FFA coupled with skeletal anchorage does not appear to have any superior skeletal effects than those without skeletal anchorage.
Introduction
Class II malocclusion is one of the most prevalent problems in orthodontics, and it constitutes one-third of the orthodontic population.1–3 Class II skeletal deformity is characterized by sagittal discrepancy between the two jaws. This could be the result of maxillary prognathism, mandibular retrognathism, or both. 4 During the period of growth, skeletal dysplasia can be corrected with removable functional appliances. 4
By influencing the maxillomandibular skeletal base and the dentoalveolar structure, the removable functional appliance therapy primarily seeks to treat skeletal dysplasia and lessen overjet.5,6 However, fixed functional appliances offer a therapeutic option for correcting skeletal class II malocclusion once the growth has ceased. Fixed functional appliances cause skeletal changes through facilitating remodeling at the temporomandibular joint and by utilizing residual growth. Clinical trials 7 have shown that these also counter discrepancies in the sagittal relationship. Numerous clinical trials contrasting late vs. early therapies have analyzed the efficacy of fixed functional appliances.7–10 However, recent evidence concluded that the skeletal effects achieved by fixed functional appliances is negligible, which is mainly attributed to the loss of anchorage caused by these appliances that could compromise the treatment stability. Attempts were made to overcome these untoward dentoalveolar adverse effects, which also includes the use of skeletal anchorage. These include use of miniscrews6,11-14 and miniplates. 7
Temporary skeletal anchorage devices (TADs) have become a vital component of contemporary orthodontics. TAD is a device that is screwed temporarily to bone for the purpose of enhancing orthodontic anchorage. 15 These TADs can be transosteal, endosteal, or even subperiosteal and are cortically stabilized or osseointegrated to the bone.15,16 TADs provide absolute or infinite anchorage, showing nil anchorage loss, which is one of the potential adverse effect of orthodontic tooth movement. 16 Titanium miniplates were introduced into dentistry for use in 1999, which showed to be well accepted by the clinicians and well tolerated by the patients, and thus now are widely used in orthodontics for its ability to provide skeletal anchorage and its biocompatible nature.17,18
Previous SRs conducted on this topic had limitations like studies other than non-randomized studies, and retrospective studies and most of the studies included in the SR were of low evidence. 19 The SR concluded that there was a lesser lower incisor proclination and better skeletal effects in the skeletal anchored group, but they also mentioned that the results should be taken with caution due to the described limitations. 19 Also, those included studies analyzed the skeletal landmarks with 2D imaging, and thus, there is a need to conduct an SR with a higher number of randomized control trials with 3D imaging.
Thus, this SR was conducted in an attempt to include only RCTs that assessed the skeletal and dentoalveolar changes post-functional appliance therapy with or without skeletal anchorage.
Materials and Methods
Registration Protocol
This review was registered with PROSPERO database (CRD42021249009) and followed the (PRISMA) Preferred Reporting Items for Systematic review and Meta analysis checklist. 20 .
Search Strategy
Several databases and sources were used to identify all relevant studies in English. The Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Google Scholar, Lilac, and PubMed database were searched to April 2021. The studies included those that involved early Class II malocclusion, related to the intervention and the outcomes involved. Manual hand search was carried out for the journals. Unpublished studies were also searched on ClinicalTrials.gov. and duplicates were removed. Irrelevant studies were excluded after reading the abstracts. The full texts of the potentially relevant studies were obtained and thoroughly checked for compliance with the inclusion and exclusion criteria. Two investigators (S.S. and P.R.) independently performed the searches.
Eligibility Criteria
Inclusion Criteria
Class II correction using fixed functional device with skeletal anchorage (miniplates or miniscrews) or without skeletal anchorage (comparative studies).
Growing patients.
RCTs.
Primary outcome: mandibular growth.
Secondary outcome: Lower incisor proclination.
Exclusion Criteria
Animal studies.
Class II correction involving extractions, class II elastics, or orthognathic surgery.
Patients with syndromes of temporo-mandibular disorders or other systemic conditions.
Patients who underwent orthognathic surgeries.
Studies without a control group.
Abstracts, SRs and meta-analyses, case reports, retrospective studies, narrative reviews, comments, laboratory studies, and letters to the editor.
Data Collection and Analysis
Two co-authors independently extracted the data, and if there were any questions, a third co-author was consulted. A pre-designed template was followed during the data extraction process. The following quantitative and qualitative data were collected: inclusion and exclusion criteria; study design, the year of publication; age and gender of the patients; type of fixed functional device; stage of skeletal maturation; size and site of mini-implant or miniplate placement; amount of force applied in grams or Newtons; method of outcome assessment (2D or 3D); and follow up.
Results
Study Selection and Characteristics
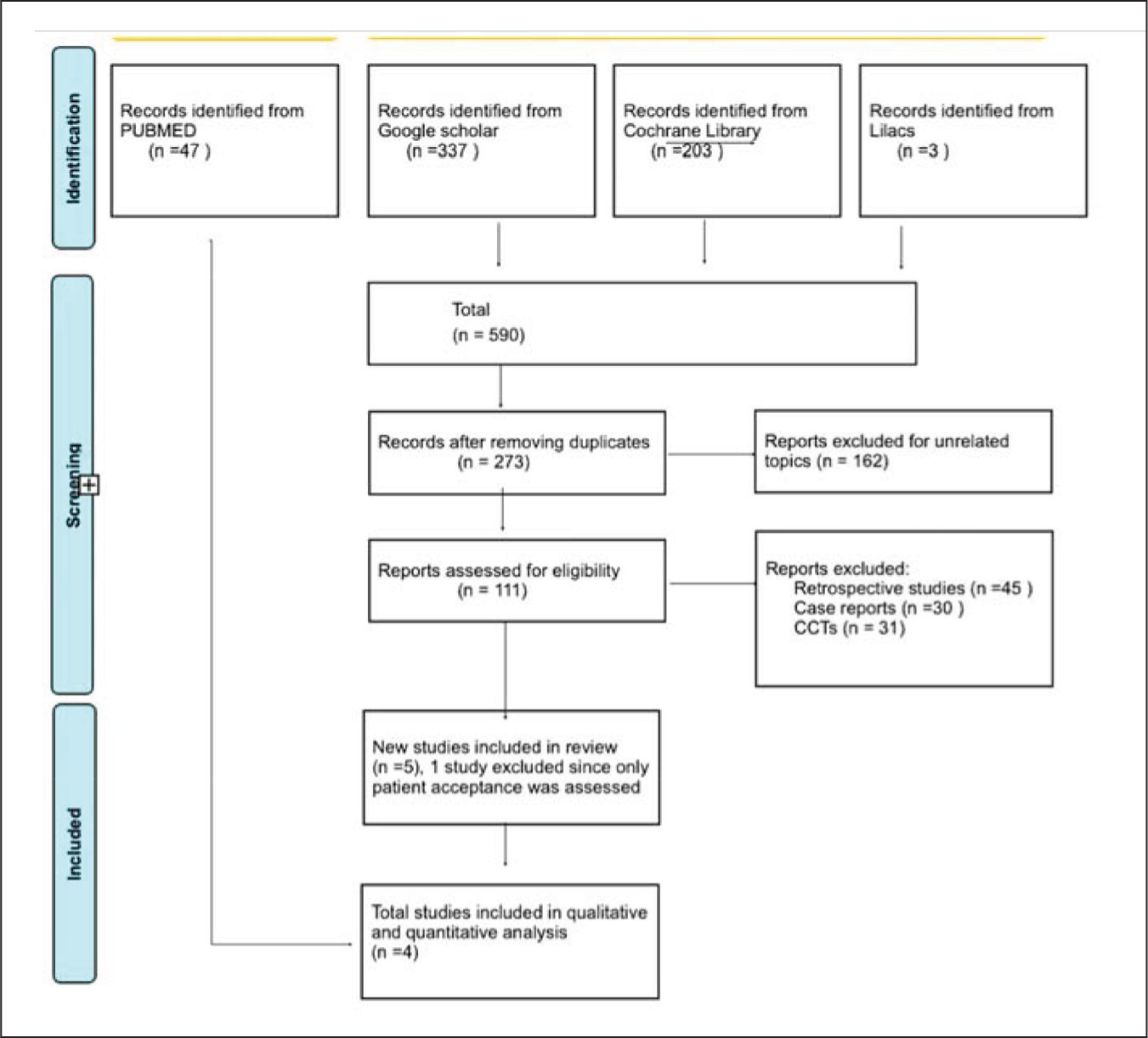
A total of 590 articles were identified from 2011 to 2021. A total of 273 articles were excluded for the reason they were duplicates and the other 162 studies were excluded as they were unrelated topics and from the extracted articles, 111 eligible full-text articles were included. Out of it, 106 studies were excluded as they were retrospective studies, case reports and CCTs. Then, one study out of the remaining five studies was excluded as the study assessed only the “patient acceptance.” Finally, four RCTs were included for qualitative and quantitative analysis. Due to heterogeneity in the measurements among the included studies, the parameters that assessed the mandibular base position, sagittal skeletal relation, and mandibular incisor inclination were evaluated (Figure 1). The study characteristics are shown in Table 1.
PRISMA Flowchart Showing the Study Selection Process.
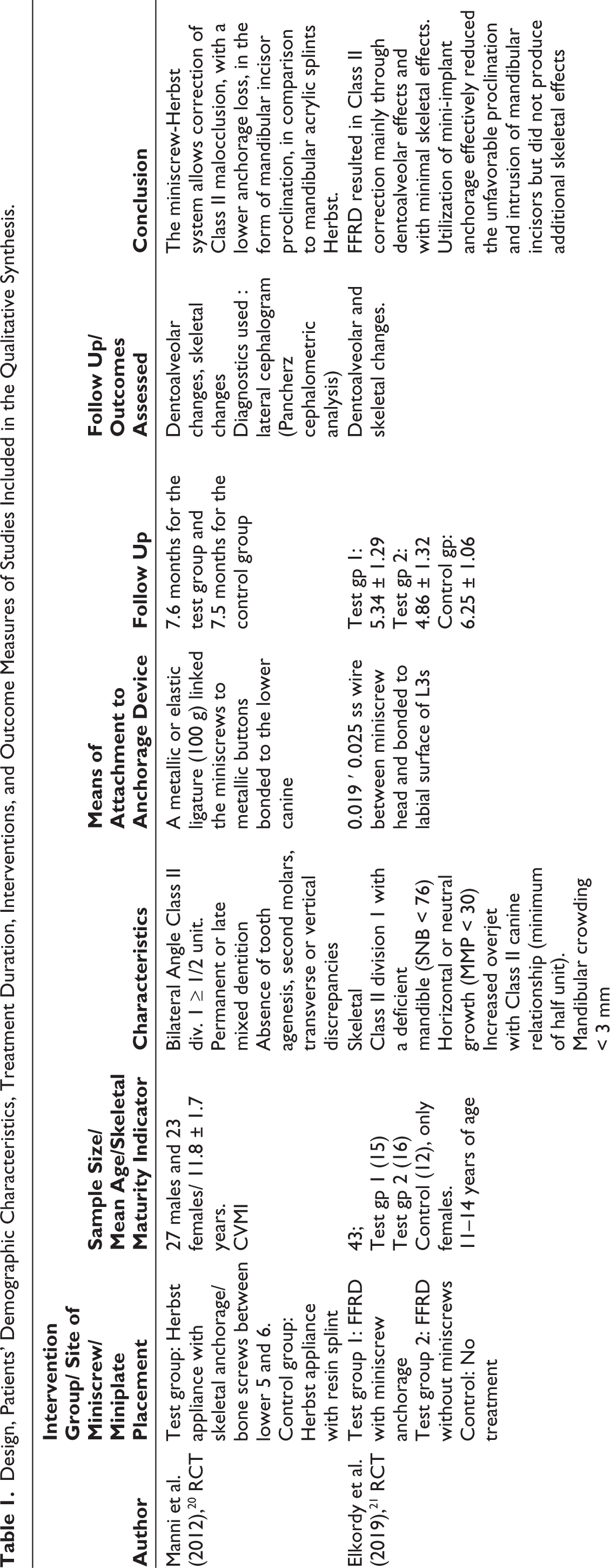
Design, Patients’ Demographic Characteristics, Treatment Duration, Interventions, and Outcome Measures of Studies Included in the Qualitative Synthesis.
Risk of Bias in Studies
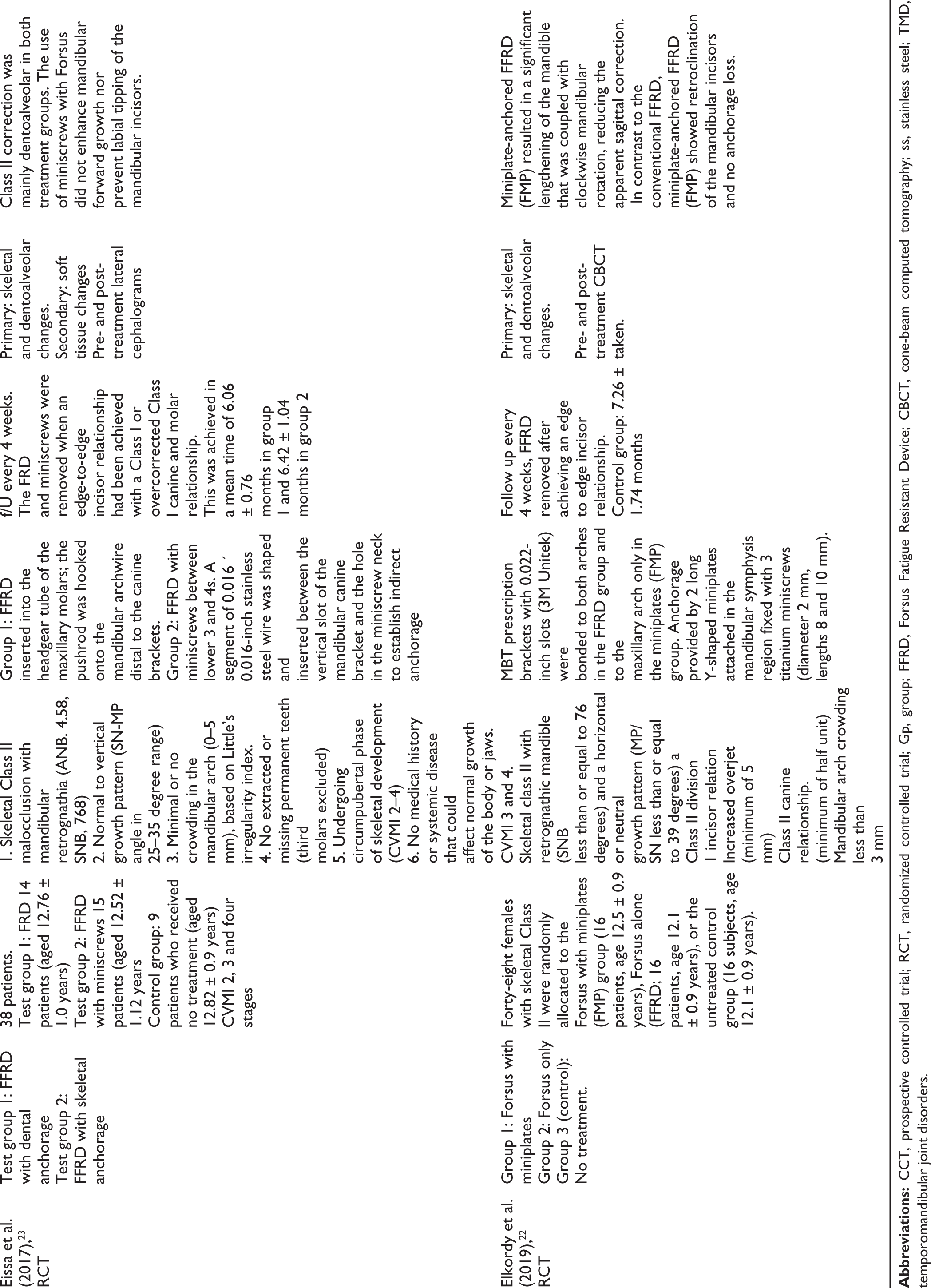
Risk of Bias Summary and Risk of Bias Graph Outlining Judgement of Risk-of-bias Items for the RCTs Included in the SR.
Characteristics of the Participants in the Studies and Interventions
A thorough summary of the characteristics, methods, and patient demographics is provided in Table 1. The design of all four studies was prospective.21–24 The inclusion and exclusion standards used in different studies were comparable. The patients with a deficient mandible with an average to horizontal growth pattern, a full cusp or a half-unit class II molar relationship, with an ANB angle greater than 4.
Three studies22-24 used the CVMI method and the other two studies21,22 did not specify the method of estimation of skeletal maturation.
Manni et al. compared the skeletal and dentoalveolar effects with and without miniscrew anchorage using a typical Herbst fixed functional appliance, while the other studies compared the effects of FFRD with and without skeletal anchorage. 20 Pre- and post-treatment changes were evaluated with CBCTs or lateral cephalograms.
Out of the total 79 patients, 71 patients were enrolled as members of the fixed functional appliance group with TADs and 71 patients were included in the conventional group (without skeletal anchorage) and the remaining 37 patients were enrolled as control as they were not treated with a functional appliance therapy. The individual’s mean ages ranged from 11 to 14 years. One of the four RCTs employed miniplates,21-23 while the other three RCTs used miniscrews for skeletal anchorage. None of the studies reported the amount of force employed for mandibular advancement. Changes in mandibular base position (SNB), lower incisor inclination, and length of the mandible (Co–Gn) were the primary parameters evaluated in this review.
Results
Individual Studies and Meta-analysis
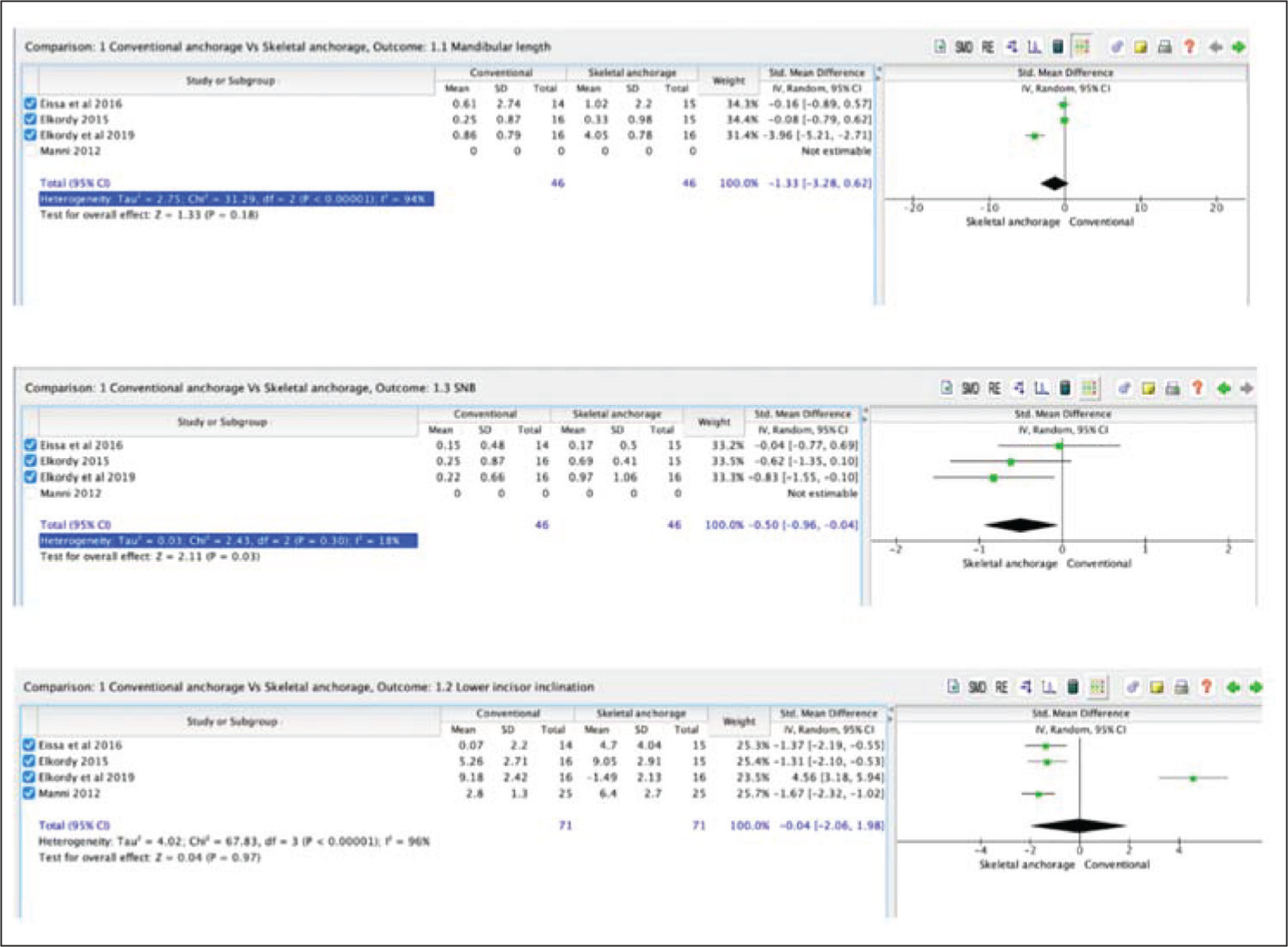
Meta-analyses were performed with all the included studies. Only three studies assessed the parameter SNB.21-23 On meta-analyses, between the skeletal and conventional anchoring groups, there was no statistically significant difference in mandibular length, with an overall effect P value of .18 and an SMD of (–1.33 (95% CI 3.28 to 0.62) as shown in the Table 1. For this metric, I2, heterogeneity was very high at 94%. Only the aforementioned three studies evaluated the SNB angle,21-23 which illustrates the relationship between the mandible and the cranial base. After pooling the data from the subgroups, the meta-analysis’s findings showed a significant difference in the changes in SNB angle between the analyzed groups, with a P value of .03 [SMD = 0.50 (95% CI –1.55 to –0.10)]. With an I2 value of 18%, this result has the benefit of acceptable heterogeneity (Figure 3).
Random-effects Meta-analysis of the Mandibular Length Changes Using Ar-Pog and Co–Gn in mm (A) and the SNB Angle Changes in Degrees (B) (SMDs) and Lower Incisor Inclination in Degrees.
Dentoalveolar Changes
Dentoalveolar change assessed was the lower incisor proclination. All the four RCTs assessed this parameter. A total of 179 subjects (71 for the skeletal anchoring, 71 for traditional FFA, and 37 in the no-treatment group) were assessed for the lower incisor inclination changes in terms of dentoalveolar modifications. Although skeletal anchors were introduced to FFA, the lower incisor proclination was not statistically different [SMD = –0.04 (95% CI 2.06 to 1.98)]. For this parameter, I2 = 94%, heterogeneity was extremely high. The included studies’ findings were quite diverse, and a number of factors had an impact on how well the treatments worked. The majority of the findings seemed to be inconsistent, and using miniplates, anchoring had greater skeletal mandibular consequences than using miniscrews with FFA. The only study by Elkordy et al. analyzed the treatment effects using CBCT. 21
Discussion
Of the enrolled 179 patients, 71 were enrolled in the study group, and 71 patients were enrolled in the comparator group (without skeletal anchorage), and the remaining 37 patients were enrolled as control as they were not treated with a functional appliance therapy. One of the four RCTs employed miniplates (Elkordy et al., 2018), while the other three RCTs used miniscrews for skeletal anchorage. None of the studies reported the amount of force employed for mandibular advancement. Changes in mandibular base position (SNB), lower incisor inclination, and length of the mandible (Co–Gn) were the skeletal and dentoalveolar evaluation parameters in this review. The experimental group consisted of patients treated with FFA with either a miniscrew or miniplate anchorage. The evaluated skeletal and dentoalveolar parameters included the changes in the mandibular length, lower incisor inclination and SNB.
Three studies measured mandibular length between the points pogonion to articulare (Ar), one study measured it between the points of the condylion (Co) and the gnathion (Gn). When skeletal anchorage was conjugated to FFA, it was discovered that the change in mandibular length was not significantly different. Lower incisor proclination is the most frequent adverse effect encountered with the use of removable or fixed functional appliance therapy, and hence, this parameter is important to consider and the skeletal anchorage did not prove to be advantageous in controlling it. The same results were found for the lower incisor angulation, whereas the SNB angle depicting the amount of advancement of the mandible in relation to the cranium showed significant difference in the skeletal anchorage group.
Previous studies claimed that no available functional appliance, whether fixed or removable, could fully address the issue of anchorage loss.19,25,26 Miniplates reduced lower incisor proclination more than miniscrews did when used with FFA, as was found in the previous SR. 19 However, our results did not support this. This could be attributed to the fact that all the studies included in this review are RCTs. But keeping in mind that the studies’ overall quality was moderate, interpreting the findings to be done with caution.
Strength and Limitations
The current review search strategy involved a thorough manual search process, multiple electronic database searches, and no language restrictions. However, since data were retrieved from only four RCTs, it is important to proceed with caution when considering the results of this systematic review. The random-effects model was utilized for data synthesis because the included studies were RCTs and the data were heterogenic. The random-effects model’s objective is to compute the average effect across all included research without allowing any one study to significantly influence the final estimate. Most of the results showed heterogeneity, which was generally supported by the carried out subgroup analyses. Due to the use of this type of anchorage in just one included study of fair quality, the majority of the results favored the miniplate subgroup; however, the superiority of the appliance design was not currently demonstrated.
This systematic review’s diligent search for unpublished studies that met the requirements was an advantage. To lessen the overestimation effect of publication bias, search for any additional pertinent unpublished trials was done. Another significant flaw in the included studies is that one of the studies failed to specify the subjects’ stage of skeletal maturation. The skeletal age should have been used instead of the chronological age because it has previously been shown to be unreliable.27-31 Since genders develop at different rates and at different times, the lack of gender differentiation in the included studies is another flaw.
Conclusion
The studies under this review do not offer enough data to draw any conclusions about the effects of using skeletal anchorage with fixed functional appliances. According to the evidence that is currently available, using temporary skeletal anchors with FFA do not appear to have any superior skeletal effects. However, new techniques, such as bimaxillary anchorage, have been shown to produce favorable skeletal effects, particularly in terms of maxillary and mandibular length and the ability to lessen proclination of the lower incisors. However, more high-quality studies and RCTs must be carried out before a proper conclusion can be made.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this systematic review was obtained from the Human Institution Ethical Committee, Saveetha University (IHEC/SDC/ORTHO-2003/21/018).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Patient consent was not obtained for the study as it was a systematic review conducted with a pool of RCTs performed previously by different authors. This review as such did not reveal any individual patient’s records.