
Abstract
Aim:
A space deficiency in the dental arch may result from the early loss of a second deciduous molar before the eruption of the first permanent molar. In this circumstance, the Distal Shoe Space Maintainer (DSSM) is recommended to prevent space loss. We aimed to evaluate the effectiveness and safety of this device.
Materials and Methods:
PUBMED, Cochrane libraries, Google scholar, Ebsco, and Science Gov. were all thoroughly searched. The effectiveness of DSSM as measured by patient tolerance and gingival response to DSSM was our main outcome goal. Also, we evaluated each study’s quality and design.
Results:
Eleven publications that fit the criteria for inclusion were examined after duplicates were removed. These papers were eventually chosen and thoroughly examined. The studies provided insufficient details regarding the efficacy of space maintenance or gingival response to the DSSM.
Conclusion:
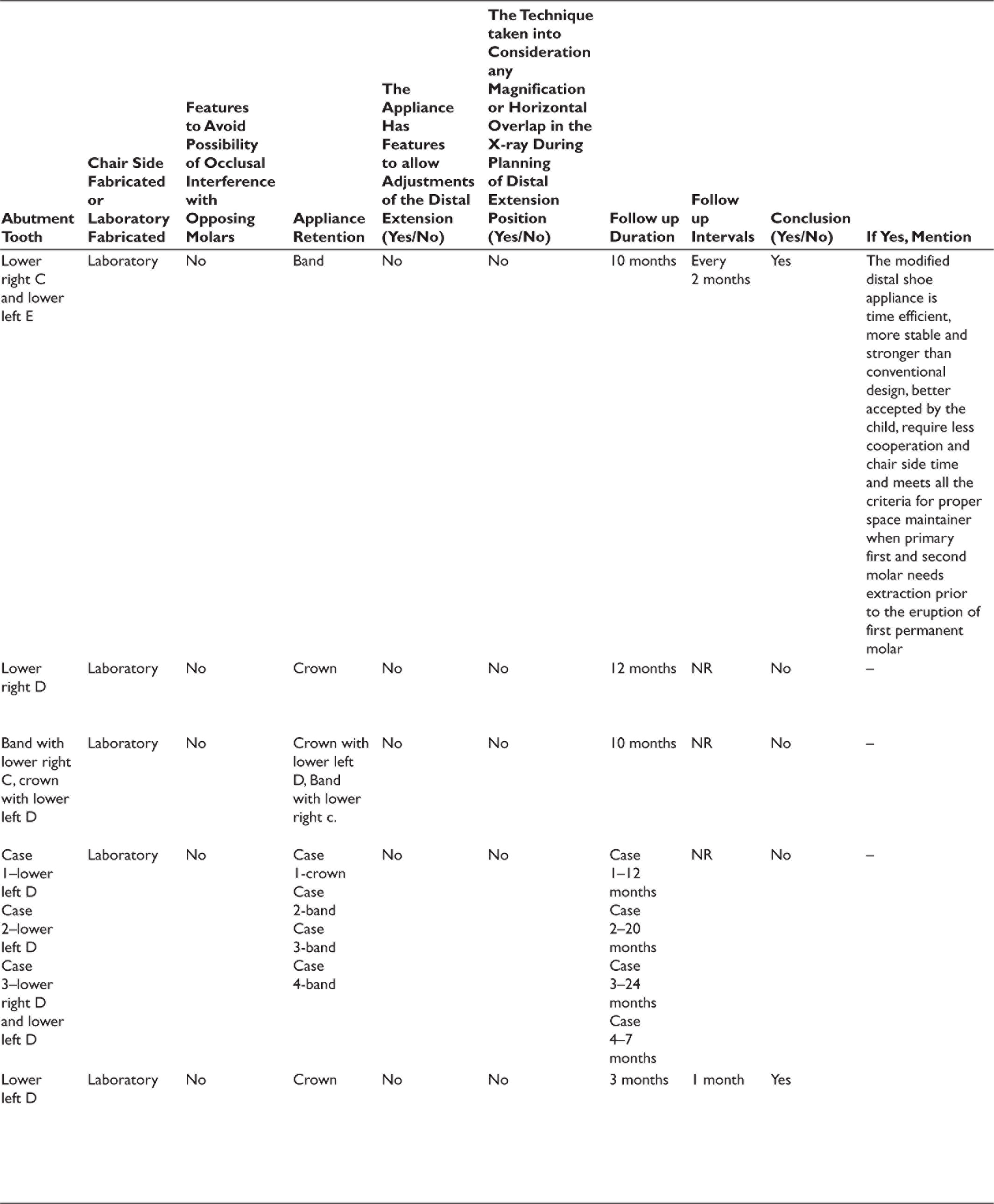
The main concern is to provide maximum benefit to the patient with minimum discomfort, maximum effectiveness, more cooperation and less chair-side time which can be achieved by the modified distal shoe appliance when compared with the conventional, as it was more stable and required less chair-side time. Though the appliances were designed keeping all the basic requirements in mind, it is firmly recommended to assess more patient-centered outcomes of DSSMs.
Keywords
Abbreviations
DSSM: Distal Shoe Space Maintainer
FPM: First Permanent Molar
PSM: Primary Second Molar
Introduction
Primary dentition plays a key role in guiding the eruption of permanent teeth and also in mastication, appearance, prevention of harmful habits, and speech. The maintenance of deciduous dentition has a significant role in preventive and interceptive dentistry, until its normal time of exfoliation. Several reasons for premature loss of teeth may be caries and trauma. The eruption of a permanent molar can potentiate a number of deleterious effects such as space loss drifting of the adjacent teeth into the space, the abnormal axial inclination of teeth, spacing between teeth, shift in the midline and significant arch space/ tooth size disparity.1–3 The deciduous second molar plays a prime role in the proper positioning and eruption of the permanent first molar. Early loss of the second primary molar is one of the chall--enging problems during the transition from primary to permanent dentition. The untimely loss of primary second molars and absence of eruption guidance for erupting permanent molars may result in the depletion of arch length. 4 Therefore, in such cases, the use of space maintainers must be preferred in order to avert space loss and malocclusion. 5 The idea of artificial space maintenance due to premature loss of primary teeth was originally by Angle, The Father of Modern Orthodontics, in the year 1907. 6
The first permanent molar can be guided using a wide range of devices. The “distal shoe,” the first space maintainer with a distal extension, was introduced by Willett in 1930. Since then, other modifications have been created. 7 The practitioner’s knowledge of one of two theories of the eruption will determine which space maintainer is most appropriate in these situations: (1) the distal surface of the second primary molar’s crown serves as a guide for the eruption of the permanent first molar, in which case a distal shoe appliance is recommended to provide the guidance for eruption of the first permanent molar. (2) A distal vertical blade in close contact with the tissue is required since the use of an appliance implanted in the tissue will not be sufficient. (3) Since the first permanent molar emerges in the correct position under the guidance of the second primary molar’s distal root, the use of an appliance inserted in the tissue will not be sufficient and a distal vertical blade in close contact with the mesial surface of the unerupted first permanent molar is required. 8
The specific design of an intra-alveolar space maintainer is needed due to the premature loss of the second primary molar prior to the eruption of the first permanent molar. Distal shoe appliance was first introduced by Gerber to guide the eruption of the first permanent molar to its appropriate position in the dental arch. 9
Various approaches have been recommended as a treatment modality for this early loss of the primary second molar including a removable partial denture or a reverse band and loop. However, it has been observed that the unerupted tooth may migrate far mesially and erupt beneath these appliances. Alternatively, the path of eruption and undesirable mesial migration of the unerupted tooth is controlled by the distal shoe appliance. Hence it has been an appliance of choice to be used to preserve the space and guide the erupting permanent molar in its place. 10
The aim of this systematic review was to evaluate the efficiency of the distal shoe space maintainer (DSSM) in children where lower second primary molars are lost prematurely before the eruption of lower first permanent molars.
Materials and Methods
Prospero Registration Number
This review was done in agreement with the established guidelines of Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and the eligibility criteria used were based on the PICOS (Participants, Intervention, Comparison, Outcomes, and Study design). The protocol used in this systematic review was published on PROSPERO (International Prospective Register for Systematic reviews) with publication ID-CRD42021235677
Review Question
Is the distal shoe appliance [Intervention] an effective and safe technique for space maintenance [Outcome], in children where lower second primary molars are lost prematurely before the eruption of lower first permanent molars [Patient]?
Search Strategy
We looked through four databases to find out if any articles on DSSMs already existed (Pubmed, Google Scholar, Ebsco & Science.Gov). The search included the following word combinations: “Intra-alveolar, “Roche,” “Willet,” “Deciduous molars,” “Primary molars,” “Premature or early,” “Loss or extraction or removal,” “Distal shoe,” “Distal extension,” and “Space maintainer.” The thorough search technique was conducted using the MeSH term “Space maintenance,” which was discovered in PUBMED. Searching for citations and screening the references lists of pertinent articles were also used.
Inclusion Criteria
[P]: Children between the ages of 4–6 years old whose lower second primary molar is suitable for the extraction or has already been extracted
[I]: The usage of a DSSM.
[O]: Outcomes: studies with measurable results
[S]: Clinical studies, case studies, or case reports from 1990 until 2021 studies.
Exclusion Criteria
They were studies examining the same issue with portable devices, observational research, animal research, and other language studies.
Data Collection
The full text of the relevant studies was analyzed in the second and final stage and relabeled once more according to the same criteria. The titles and abstracts of the articles retrieved during the database searches were analyzed. The discrepancies were recognized and resolved through discussion with the other author when necessary.
Data obtained includes four domains:
Identification of the study (article title; journal title; authors; country of the study; language; publication year; host institution of the study Methodological characteristics (Study objective or research question; sample characteristics, for example, sample size, sex; age, and preoperative diagnosis) Main findings like clinical and radiographic success rate on follow-up of 6 months and beyond, dropouts.
Quality Assessment
Evaluation of each study’s design and quality, including whether a specific research question was addressed, whether pertinent keywords were used, whether the studies’ objectives and purposes were clearly stated, 11 and whether the outcomes and findings of the studies listed in Table 2 were accurate.
Results
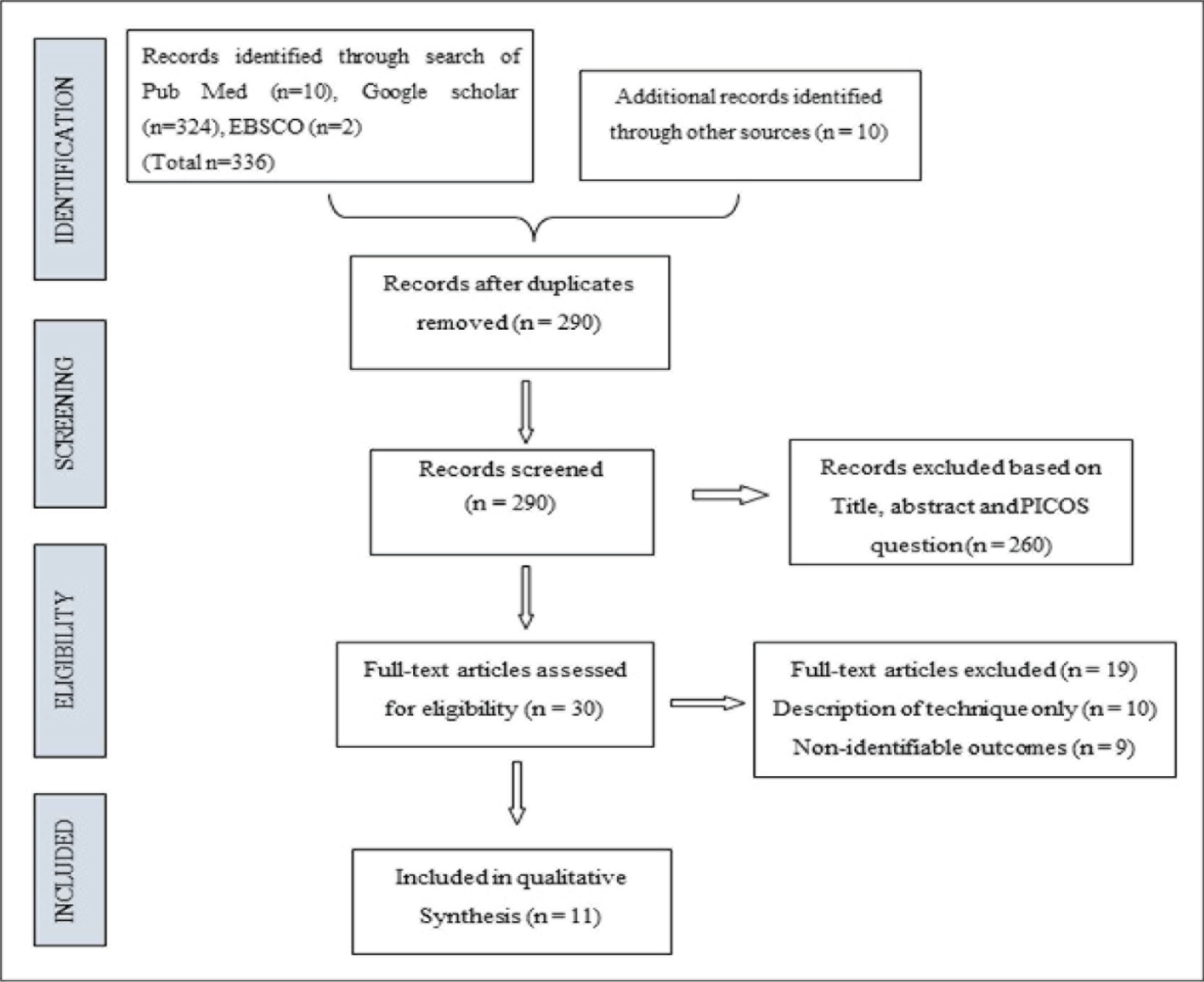
Details of the study selection process are outlined in Figure 1. From the database searches, we found 336 articles; after we removed the duplicate articles, 290 remained. The process of evaluating the eligibility of the studies comprised a screening phase from where the articles were distributed among the reviewers for the title and abstract independent reading. This showed 260 ineligible studies, therefore excluded, since they were not directly associated with the objectives and the purpose of the research. Two of us (MVD and NAC) then searched the case series and case reports and excluded 19 articles. Finally, 11 studies remained (Table 1) that met our inclusion criteria. The quality evaluation score for the studied studies, which are displayed in Table 2, varied from 2 to 3 out of 10, indicating that the investigations were of low quality.
PRISMA Chart Reporting the Article Selecting Process for Systematic Review.
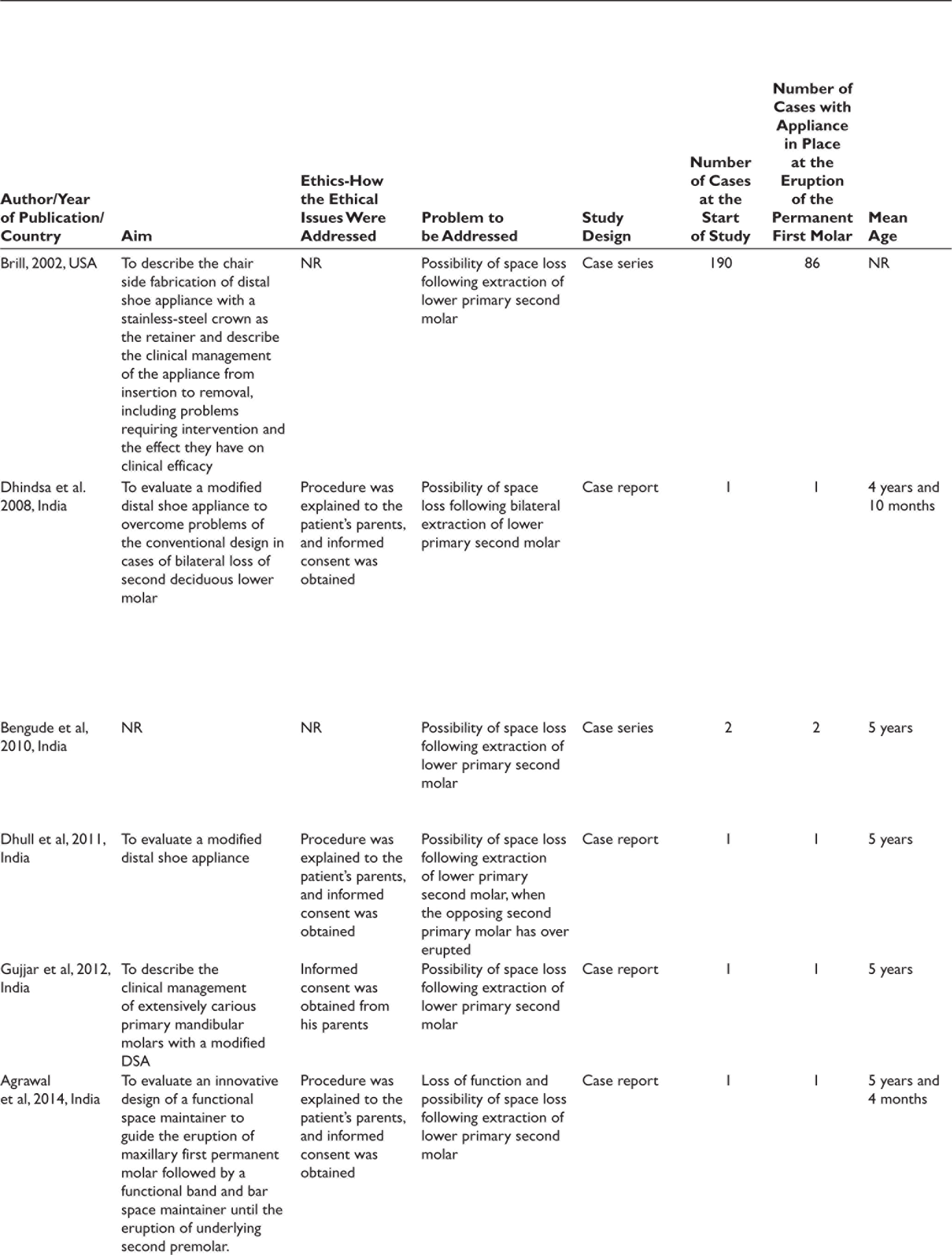
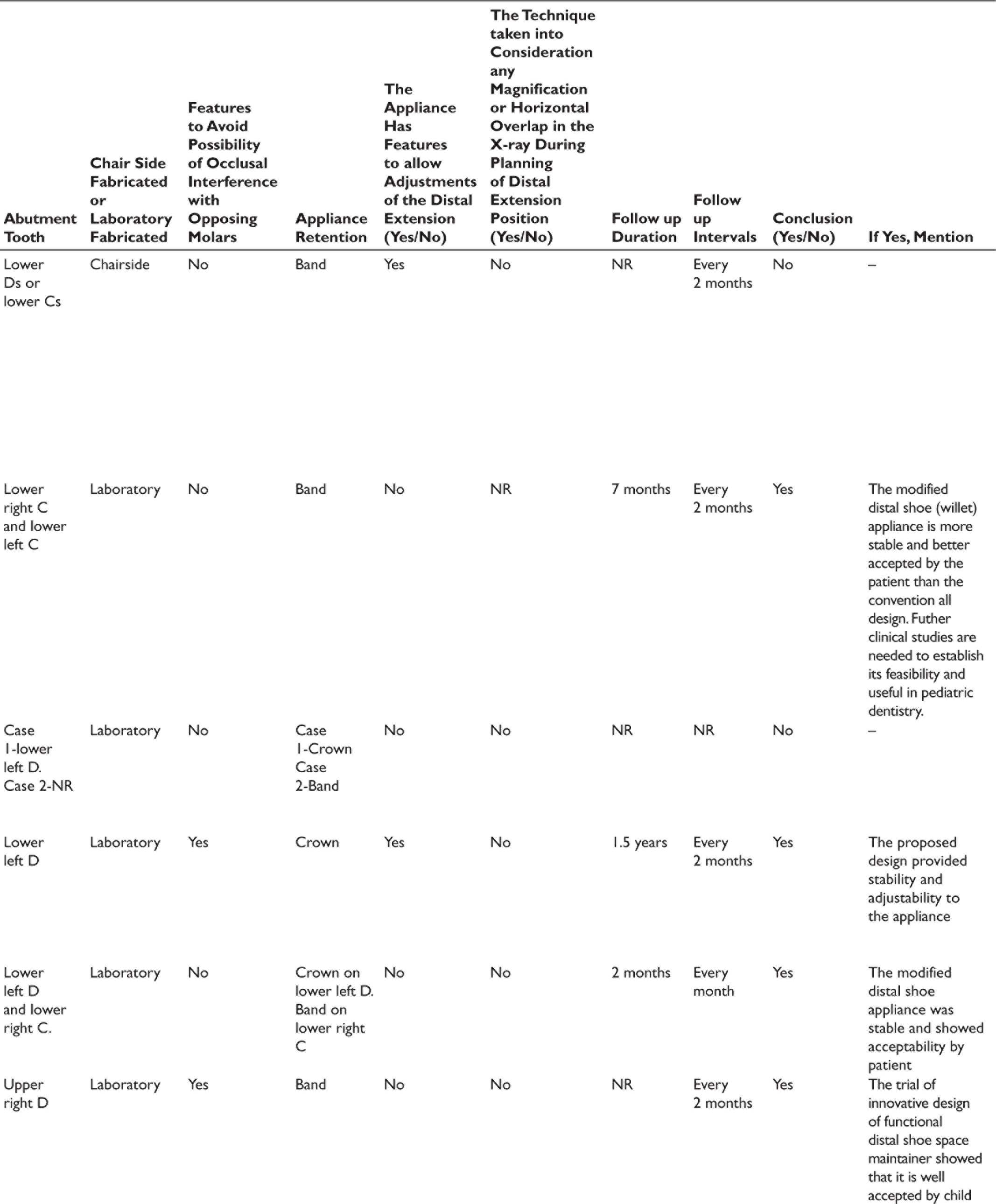
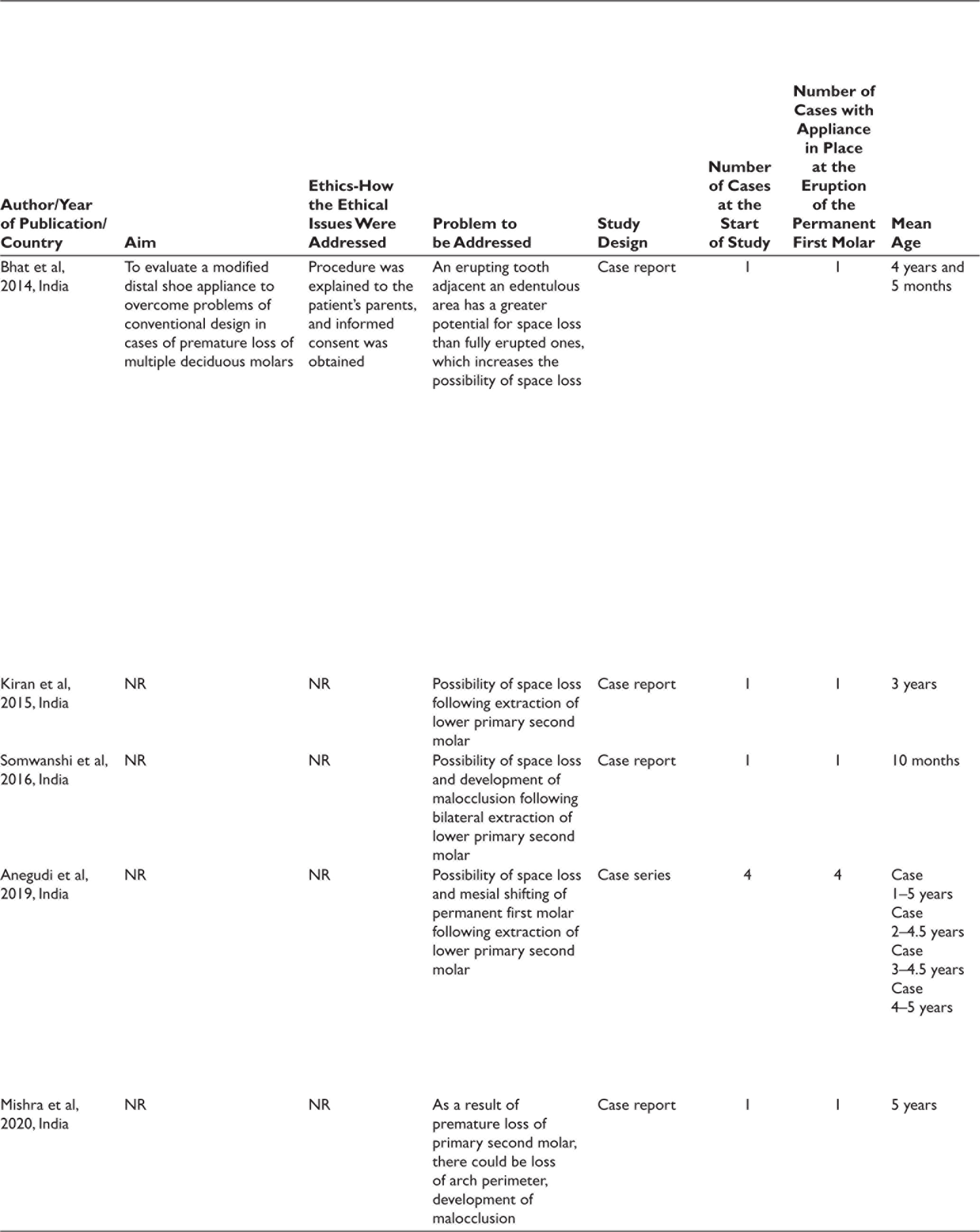
Characteristics of Studies Included.
Quality Assessment of Studies Included in Systematic Review.
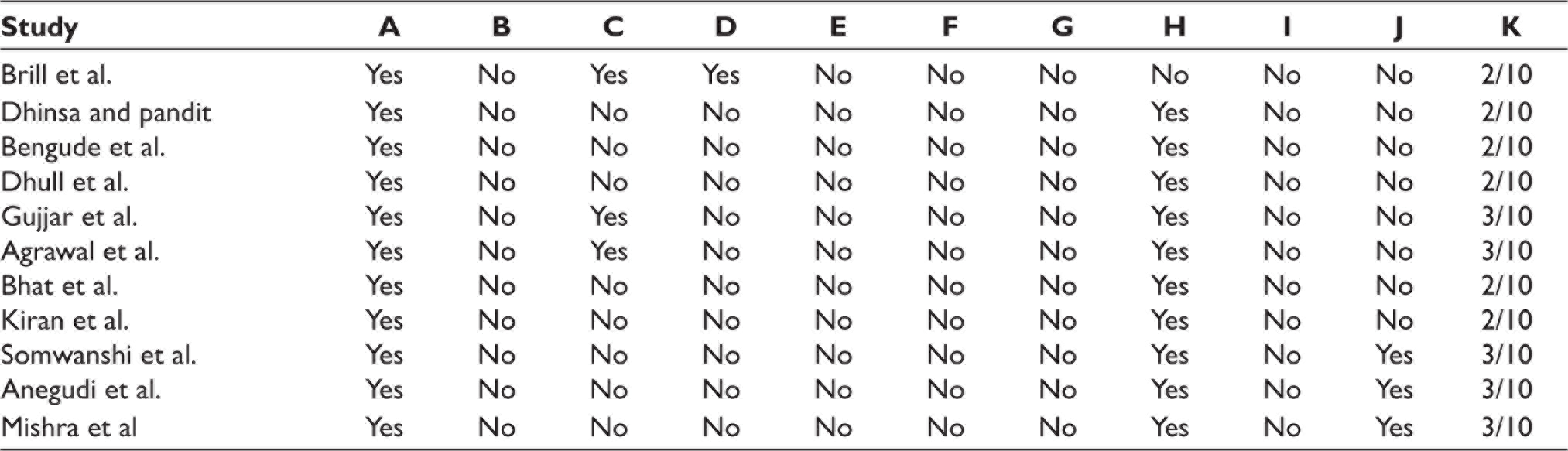
Did the study include keywords that identify areas covered in this case report? Did the study address a clearly focused question? Are the aims and purpose of the study clearly stated? Are the details of the technique sufficiently given to allow its transferability to other clinical settings? Are the outcomes of the study clearly stated? Are the outcomes measured using a defined method? Are the methods for collecting data clearly described? Is the case clearly described? Are the results credible and relevant for practice? Are the conclusions drawn justified by the results? Quality assessment score
Discussion
Deciduous or primary teeth act as an ideal space maintainer. So, always a decayed primary tooth should be restored if possible by conservative or endodontic treatment. 12 The only reason the primary second molar is an important tooth in the mixed dentition is because it directs the eruption of the permanent first molar. The permanent first molar’s mesio-occlusion pattern of eruption is assisted by the distal surface of the deciduous second molar. Thus, it is crucial to protect the deciduous second molar until the eruption of the permanent first molar. It is not recommended to extract the same thing unless it is indicated. 13 Pediatric dentists are once again faced with a dilemma when treating individuals who have lost multiple primary molars at an early age. 14 Thus, the case reports included are age-specific (4–6 years of age), irrespective of gender without any systemic involvement.
As defined by Baroni et al and Qudeimat et al., the success criterion of a DSSM is the successful guidance of the unerupted permanent tooth into the arch with no problems associated with the appliance. 9
The various other factors to be considered, include a long-range plan for space management in a growing child whose occlusion will need surveillance through three developmental stages: the primary, the mixed, and the permanent dentition. 15
Because of the cantilever design, the production of distal shoe SMs is technique-dependent, and its use is prohibited in a number of circumstances. According to histological investigations, the implantation of intra-gingival extensions does not result in complete epithelialization and is accompanied by a chronic inflammatory response. Thus, DSSMs should not be utilised in those who have a history of systemic diseases such as congenital heart disease, blood dyscrasias, immunosuppression, rheumatic fever, or juvenile diabetes and who require prophylactic antibiotic coverage. 16
According to Gujjar et al. 13 removable space maintainers can also be the appliance of choice but have certain disadvantages, such as requiring cooperation by the patient and the possibility of being lost or broken, hence fixed space maintainers can be preferred. Gujjar et al. 13 reported a case of 5 year old boy requiring bilateral DSSM and found out that solder joint failure is a typical reason for the failure of any fixed space maintainers. De-cementation, obstructions to the eruption of the permanent dentition, and pathological involvement of the abutment tooth are other causes. Nonetheless, fixed space maintainers outperform removable appliances, which were possibly more often used in the past and do not require exceptional patient participation. Frequent inspections are necessary to evaluate the appliance’s integrity, make sure it is maintaining the space as planned, and also for watchful surveillance and prevention because the appliance can put patients at risk for dental caries and gingivitis. 1
Among all of the choices for space maintenance, the distal shoe appliance has many contraindications for use, mainly due to the subgingival extension which involves continuous communication between the oral environment and the intra-alveolar space. Meticulous oral hygiene has to be maintained and its use is contraindicated for patients with systemic diseases that affect healing or cardiac anomalies requiring antibiotic prophylaxis. 17
As a result of premature loss of the primary second molar prior to the eruption first permanent molar, there could be a loss of arch perimeter, which would eventually need complicated orthodontic intervention. 18
A modified distal shoe appliance was recommended as part of the treatment strategy for a 4.5-year-old boy who had lost all of his primary molars, according to Bhat et al. 14 Bilateral fixed appliances with intra-alveolar extensions are capable of guiding the eruption of the first permanent molar tooth into its normal place and preventing space loss due to the mesial tooth drifting with the aid of an anchorage from the other teeth in the jaw. Furthermore, compared to removable appliances, this appliance is more kid-friendly due to its fixity, maximum stability, and straightforward design. However, there are significant drawbacks to this device, including its difficult construction, low cost, and lack of functionality. This device may be more suitable for youngsters who are uncooperative. Depending on the eruption pattern of the molars and incisors, a modified DSSM may be used in place of other appliances as a short-term appliance. In this situation, it will take several sittings for lingual arch appliances to see the eruption of permanent successors. Yet, research has revealed that when primary molars are lost too quickly, the first permanent molar emerges earlier than anticipated. So, it would be less alarming if mandibular incisor eruption occurred before the full eruption of permanent first molars. In order to provide simple chair-side adjustability, a modified appliance was made in the case series of Afshar et al. 8 by soldering a portion of the Gerber-type distal shoe. Depending on the patient’s clinical condition, the appliance must be replaced once the first permanent molar has fully erupted or if there is any interference with the eruption of permanent incisors. 8
Further adjustments in appliances are made in healthcare settings to satisfy the demands of the patients. The conventional design has a number of issues when several primary teeth are lost before the eruption of the first permanent molar. In order to provide comfort, cooperation, and success for various paediatric patients, the conventional designs were modified. If a DSSM was made by banding a canine, the stability of the device was a problem. Hence, in a different case by Bhat et al.,8 a modified distal shoe appliance design was employed, which preserved the space’s mesiodistal dimension without affecting the patient’s stability or cooperation. However, this style of design has some drawbacks, like being non-functional, difficult to fabricate and cannot be administered to unwilling individuals. Bilateral appliances have the potential to obstruct the emergence of permanent mandibular incisors. As a result, it is possible to develop a short-term modified bilateral distal shoe appliance whose duration can be subjected to the observed eruption of permanent mandibular incisors on both a radiographic and clinical level.
The bilateral acrylic “saddle” appliance is an alternative space maintainer with major drawbacks such as poor retention and patient compliance. 14 There are several advantages served by the modified distal shoe appliance over the conventional appliance such as less chairside time, and less cooperation of the patient, increased stability and strength, fixed appliance. Premature eruption of successors at a very early stage of root formation occurs when the overlying primary tooth has a periapical infection and significant bone destruction. The periapical lesions associated with deciduous dentition can reveal a number of anomalies, such as eruption problems, enamel hypoplasia (Turners Hypoplasia), tooth displacement and rotation, and partial or complete cessation of root formation of the next permanent tooth. Although it has been observed, failure of the tooth germ to grow as a result of periapical or inter-radicular infection of the primary tooth can result in hypoplastic crowns with significant pitting and abnormalities of the crown in respect to the right second premolar. 14
The fabrication of the Roche appliance was chosen in another case report by Mishra et al. 18 in which a 5-year-old boy was involved, whose left primary second molar was recommended for premature extraction. The Roche appliance consisted of a horizontal part of the wire spanning the space and a vertical sub-gingival extension that was seated roughly 1 mm below the medial most aspect of the first permanent molar. Using a radiograph, the length of the loop from the lower left primary molar’s distal-most aspect up to the unerupted permanent first molar’s mesial aspect was estimated. 18 According to Nayak et al., roughly 51% of prematurely lost first primary molars and 70% of prematurely lost second primary molars cause space loss and, as a result, malposition of a permanent tooth in that quadrant. Many orthodontic cases with crowding and lack of space in the permanent dentition may be avoided if the practitioner’s intervention could keep enough space in mixed dentition.
The effectiveness of DSSM and the gingival response to it have not been studied in the published research that is currently accessible. There is proof that DSSM is well-tolerated by patients. It was determined that the studies had inadequate design and quality. The drawback of this systematic review is that the effect of appliance design in each study can directly influence the survival rate of the appliance. There is no clinical trial with no longer follow-up to authenticate the results and survival rate of the appliance.
Conclusion
In the light of available evidences in our review, the following conclusions can be drawn:
The main concern of the operator is to provide maximum benefit to the patient with minimum discomfort, maximum effectiveness, more cooperation and less chair-side time which can be achieved by the modified distal shoe appliance when compared with conventional DSSM as it was more stable and required less chair side time. The modified semi-adjustable design can also withstand the force of eruption by providing broad contact, thus preventing lingual or buccal deflection of erupting first permanent molar. There is no measured evidence for effective space management and safety of DSSMs on gingival tissues, that could help clinicians to confirm or counter its use in children. Among the available studies, none of the studies has adequately covered all the technical aspects of fabrication. There are weak evidences to make any recommendation on which design is appropriate due to the lack of patient-centered studies. Though the appliance was designed keeping all the basic requirements in mind, it is further recommended to conduct high-quality studies to assess more patient-centered outcomes of DSSMs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.