
Abstract
Aim:
Basic guidance on nonpharmacological behavioral management techniques in dental practice is fundamental for the effective treatment of pediatric patients. The aim of this study was to compare the use of basic nonpharmacological behavior guidance in general and specialist pediatric dentists and to evaluate the perceived difference in their effectiveness across hospital clinics in Jeddah, Saudi Arabia.
Material and Methods:
A cross-sectional study with a nonpurposive sample of 179 registered general and pediatric dentists in the Saudi Dental Society based in Jeddah in 2019. Participants were contacted and asked to complete a validated questionnaire. The first section of the questionnaire comprised questions on demographic data and the second section investigated the frequency of the use of various behavioral management techniques. Descriptive statistics (frequency and percentages) and inferential statistics were used.
Results:
A total of 109 participants completed the survey; 52 were general dentists and 57 were pediatric dentists. The techniques tell–show–do (P = .018), positive reinforcement (P = .004), distraction (P = .001), and nonverbal communication (P = .001) were used more frequently by pediatric dentists than general dentists, and there were statistically significant differences. Also, pediatric dentists reported that the techniques tell–show–do (P = 0.035), positive reinforcement (P = .026), distraction (P = .011), and nonverbal communication (P = .007) were highly effective more often than general dentists did.
Conclusions:
Statistically significant differences were found between general and pediatric dentists in the use of basic behavioral management techniques. Broadly, general dentists used fewer behavior guidance techniques compared to pediatric dentists. More pediatric dentists reported that behavioral management techniques were effective in comparison to general dentists.
Introduction
One of the most prevalent chronic diseases in children throughout the world is dental caries (tooth decay), which is more common among children in developing countries than developed countries. 1 In Saudi Arabia, despite high rates of dental caries in children, 2 a relatively low number of specialist pediatric dentists are available to provide dental care. 3 Indeed, the prevalence of caries in children is high regardless of countrywide introduction of caries preventive modalities and water fluoridation. 2 Based on the findings of one systematic review, the approximate prevalence of dental caries and severity in Saudi children was estimated at 80% (mean decayed, missing, or filled teeth (DMFT) index = 5.0) in the primary dentition and 70% (mean DMFT index = 3.5) in the permanent dentition. 2 Census data taken in 2018 shows that there are more than 10 million <19 years old children living in Saudi Arabia. 4 It is difficult to effectively meet the high demands of care for such a large number of children since there are only 444 registered pediatric dentists in Saudi Arabia, 3 although there are 11,942 licensed general dentists providing dental care to the majority of pediatric patients. 3 Problematically, some previous studies have found that a number of general dentists choose not to treat children. 5
Several studies have shown that when providing dental care to children, behavioral management techniques, pain management, and treatment modalities used by general dentists differ from those used by pediatric dentists. 6 In the Netherlands, pediatric dentists were found to perform more preventive procedures, restorative treatments, and extractions compared to general dentists in the treatment of young children.7, 8 In Germany, pediatric dentists were shown to use a wider variety of behavior management techniques when treating anxious children compared to general dentists, and a greater number of general dentists than pediatric dentists reported that treating this group of children was a difficult task. 9 Also, pediatric dentists in general prefer to provide definitive treatment to preschool children while general dentists are inclined to use conservative and noninterventional techniques.10,11
Pediatric dentists receive in-depth theoretical and clinical training in behavior management techniques for children, enabling them to better communicate and guide the child patient through their dental experience. 12 Undergraduate dental programs in Saudi Arabia prepare graduates by teaching comprehensive courses on pediatric skills, with particular emphasis on basic behavior management techniques and hands-on experience in the comprehensive treatment of children. 13 A recent survey on acceptability of behavioral guidance was conducted on Malaysian dental students and it was found that most students cited acceptance of reinforcement and desensitization methods techniques such as a positive reinforcement and tell–show–do but not for aversive interventions such as hand over mouth. 14
There is a research gap on whether these undergraduate programs enable general dentists to use behavior management techniques effectively to provide children dental treatment of quality equivalent to that given by pediatric dentists or not. Therefore, there is a need to conduct such research comparing between the use of nonpharmacological behavior guidance among general dentists and pediatric dentists. Thus, the first aim of the study is to compare the use of basic nonpharmacological behavior guidance by general dentists and pediatric dentists in Jeddah, Saudi Arabia. The second aim is to assess the difference in perceived effectiveness of basic nonpharmacological behavior guidance through reports of general and pediatric dentists.
Materials and Methods
Study Design and Data Collection Procedure
This descriptive cross-sectional study was conducted in Jeddah between October 2019 and November 2019. It included general dentists and pediatric dentists registered with the Saudi Dental Society (SDS). Dentists and pediatric dentists were invited to participate from five pre-selected governmental and private dental clinic hospitals within Jeddah. Participants were also invited to participate during SDS meetings. Those who agreed and consented to participate were provided with a detailed explanation of the study aims and were informed that participation was voluntary and confidential. The questionnaire was given to the participants on a tablet to be completed independently in the hospital setting. The study incorporated a nonpurposive sample of 179 participants, comprising 122 general dentists, and 57 pediatric dentists.
Sample Size Calculation
The sample size was calculated based on the reported statistics by distributed dentists in different areas across Saudi Arabia in 2017. 3 Following the method of AlBaker et al. (2017), it was assumed that response rate is 70%, so, for example, if the number of SDS-registered pediatric dentists in Jeddah is 53, then the minimum sample size should be 37.
Ethical Approval
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study documents were approved by the Research Ethics Committee of King Abdulaziz University Faculty of Dentistry (Approval No. 099-10-18). A written informed consent was obtained from participants prior to the study.
Study Instrument
A web-based questionnaire was utilized to assess the use of basic nonpharmacological guidance among licensed general and pediatric dental practitioners. The online questionnaire was written in the English language. The survey was developed and reviewed by the authors.
A pilot study on a focus group was conducted to validate the content of the questionnaire, which involved four pediatric dentistry consultants, related to its clarity, simplicity, and ambiguity of questions and relevance to the study aim, using a four-point Likert scale with four options (1 = very important, 2 = important, 3 = moderately important, and 4 = not important). The validity of the questionnaire was ascertained by calculating the content validity index (CVI). The questionnaire was given on two occasions to four postgraduate students in pediatric dentistry with a two-week interval to evaluate its reliability.
The questionnaire comprised 15 questions varying between multiple choice, check boxes, and short answers, formulated on Google Forms (Google LLC). The first section of the questionnaire inquired about demographic data, such as dental education, experience, employment, occupation, age, and gender distribution of the patients seen by respondents. The second section of the questionnaire involved questions related to the frequency of use of behavioral management techniques, that is, tell–show–do, positive reinforcement, distraction, nonverbal communication, voice control, live modeling, and parental separation. The questionnaire also contained questions on the effectiveness of nonpharmacological guidance techniques for providing dental care to children. The estimated time taken to complete the survey was 10–15 min.
Statistical Analysis
Participants filled out the online questionnaire and the data were arranged on an Excel (Microsoft) sheet. All data were anonymized and saved securely by password on a desktop computer. The data were entered and analyzed using the Statistical Package for the Social Sciences (SPSS), version 22.0 (SPSS Inc., Chicago, II, USA). Descriptive statistics, frequency, and percentages were used to present the outcomes and independent variables. A comparison between dentists and pediatric dentists was made using chi-squared tests, Fisher’s exact tests, and independent samples t-tests. The P value of .05 was set as statistically significant.
Results
Four pediatric dentistry consultants rated the item content of the data collection tool. There was an agreement recorded at 89.5% for the questionnaire. However, the reliability recorded by the four postgraduate students was 83.0%. Table 1 shows the participants’ demographic characteristics and clinical experience with pediatric patients. A total of 109 participants out of 179 completed the survey, giving the response rate of 60%. Fifty-two participants (47.7%) were general dentists, and 57 participants (52.3%) were pediatric dentists. General dentists were predominantly aged <35 years (84.6%), whereas a lower proportion of pediatric dentists (59.6%) were in this age category. Females were just under two-thirds of the general dentist participants (61.5%) but approximately three-quarters of the pediatric dentist participants (75.4%).
Participant Demographic Data and Clinical Experience with Pediatric Patients
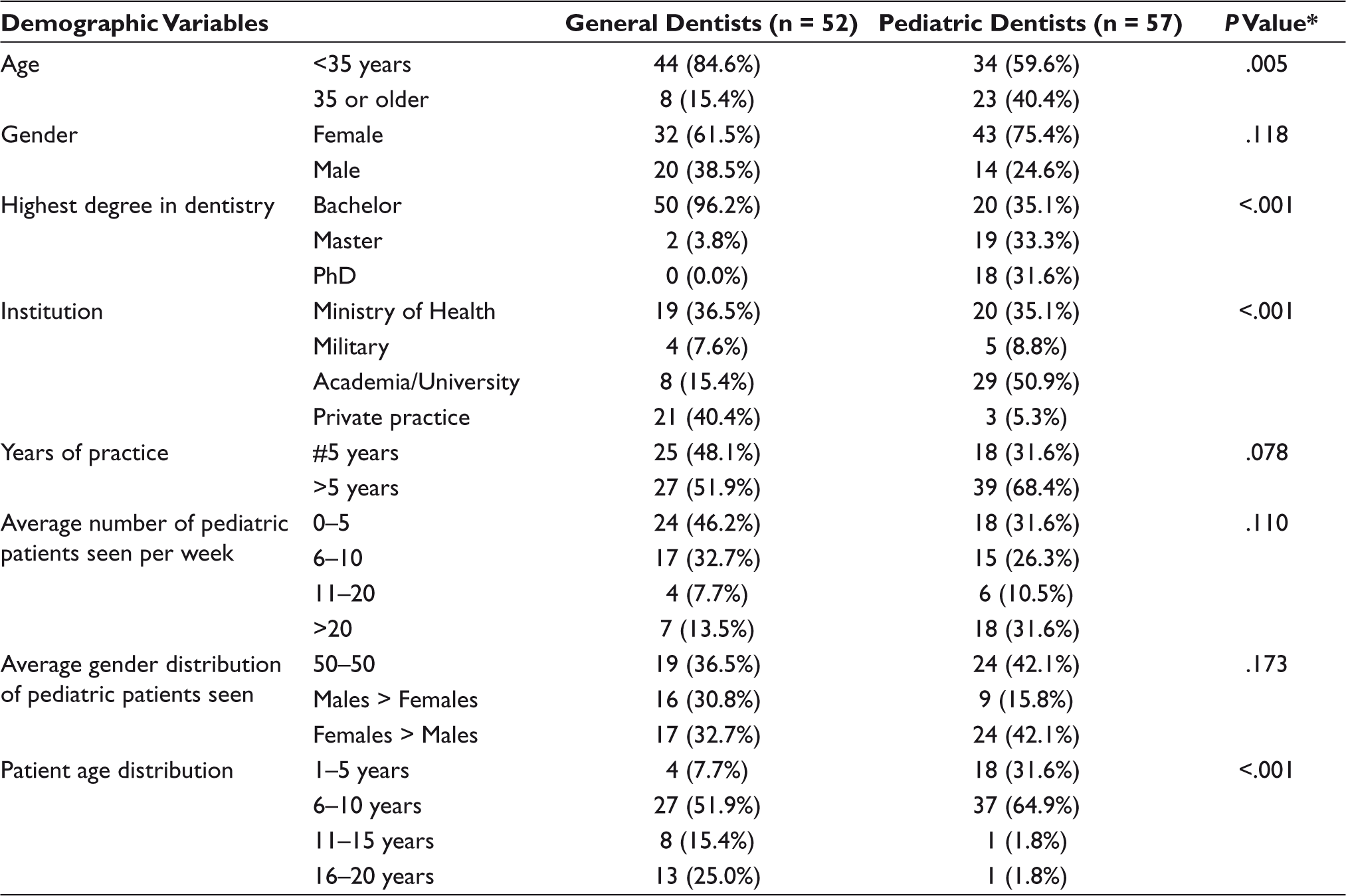
*Chi-squared test and Fisher’s exact test, P <.05.
There was no significant difference found between general dentists and pediatric dentists regarding the number of years of practice (P = .078), the average number of pediatric patients seen per week (P =.110), or the average gender distribution of pediatric patients (P = .173). General dentists reported treating a larger number of older pediatric patients while pediatric dentists reported treating a larger number of younger pediatric patients (P <.001). In particular, only four general dentists (7.7%) reported that the predominant age of patients seen was 1–5 years, compared to 18 pediatric dentists (31.6%). Pediatric patients aged 6–10 were the most commonly seen by 51.9% of general dentists compared to 64.9% of pediatric dentists; pediatric patients aged 11–20 were reported as the most common age group seen by 40.4% of general dentists, compared to 3.6% of pediatric dentists.
The Use of Basic Behavioral Guidance by General Dentists Compared to Pediatric Dentists
Table 2 shows a comparison between pediatric and general dentists regarding the use of behavioral management techniques. All pediatric dentists reported using tell–show–do, positive reinforcement, and distraction, while most general dentists reported using these techniques (92.3%, 86.5%, and 80.8%, respectively), and this difference was statistically significant (P <.05). Also, more pediatric dentists reported using nonverbal communication, live modeling, and parental separation than general dentists (P = .001, P = .003, and P = .019, respectively). No statistically significant difference was found between the number of pediatric dentists and general dentists who reported using voice control.
Use of Nonpharmacological Behavior Guidance Techniques in General and Pediatric Dentists
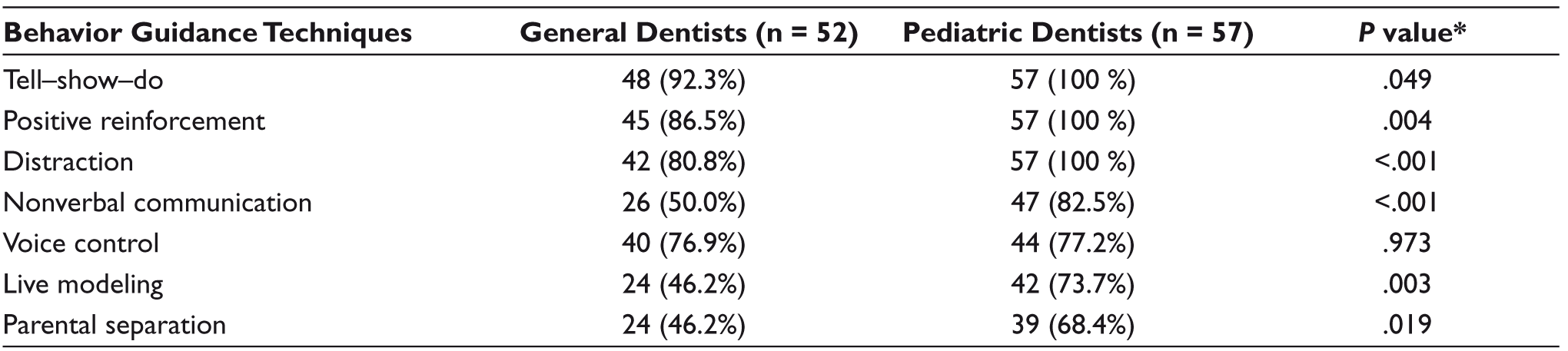
*Chi-squared test and Fisher’s exact test, P <.05.
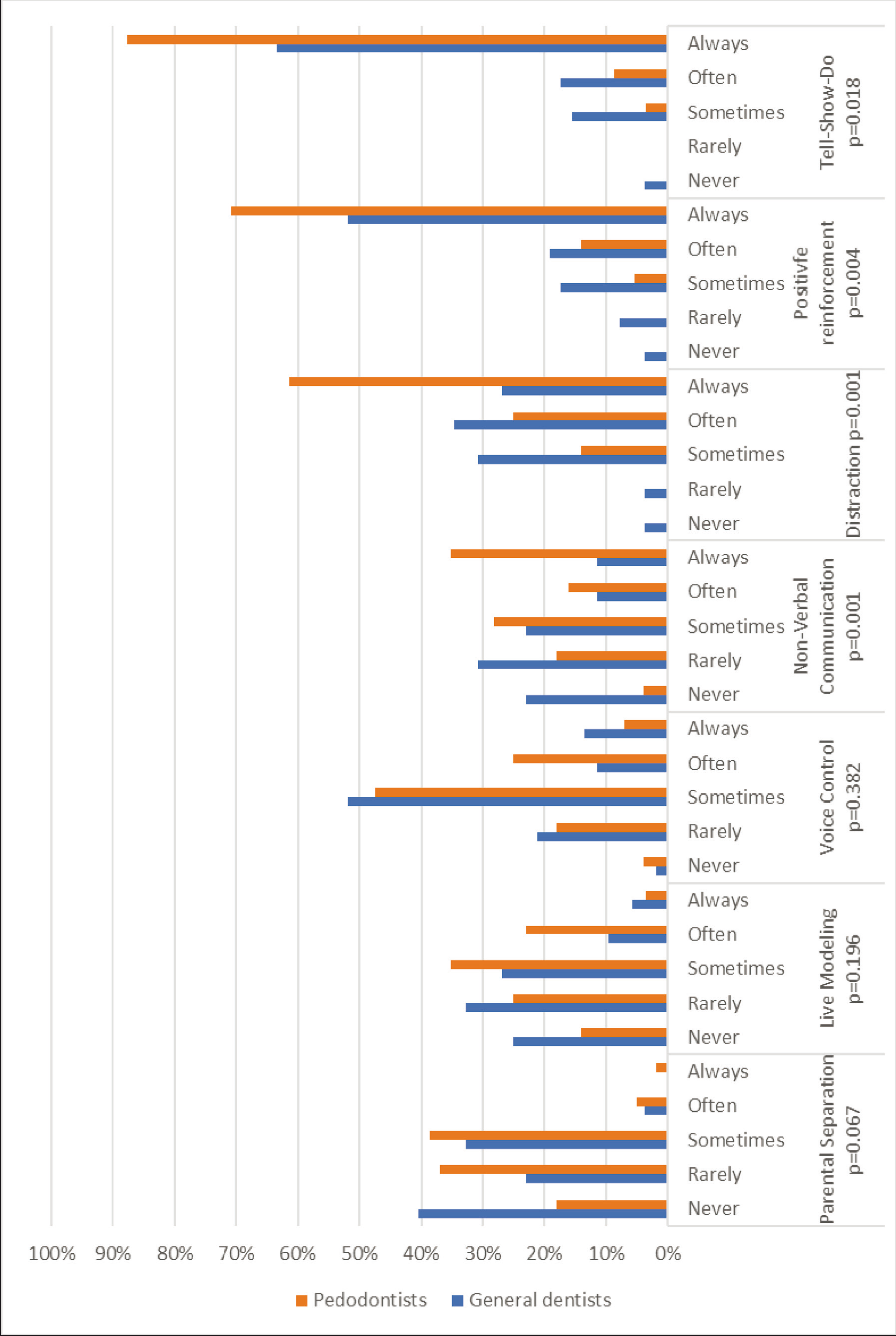
Figure 1 shows the difference in frequency between the use of basic behavioral management techniques by general and pediatric dentists. Pediatric dentists used the following techniques more frequently than general dentists: tell–show–do (P = .018), positive reinforcement (P = .004), distraction (P = .001), and nonverbal communication (P = .001). No significant difference in frequency was found between general and pediatric dentists in the use of voice control (P = .382) and live modeling (P = .196). Pediatric dentists reported using the parental separation technique more often than general dentists, although the difference was not statistically significant (P = .067).
Frequency of Behavioral Management Techniques Used by General and Pediatric Dentists
Difference between General and Pediatric Dentists in the Perceived Effectiveness of Basic Nonpharmacological Behavior Guidance
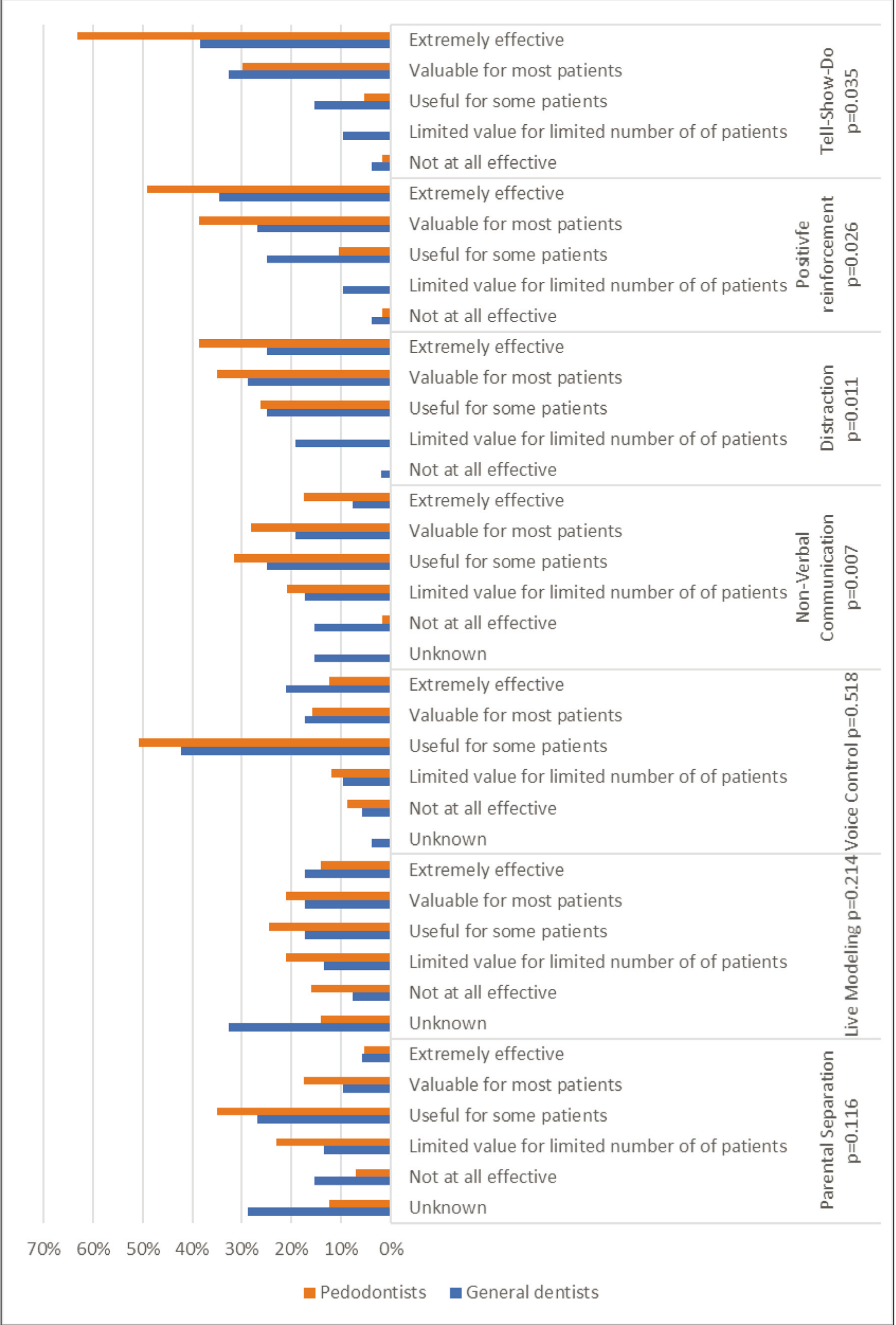
Figure 2 shows a comparison of the reported perceived effectiveness of various behavioral management techniques by general and pediatric dentists. Pediatric dentists reported the following techniques as highly effective more often than general dentists: tell–show–do (P = .035), positive reinforcement (P = .026), distraction (P = .011), and nonverbal communication (P = .007). No significant difference was found between general and pediatric dentists in terms of the perceived effectiveness of voice control (P = .518), live modeling (P = .214), and parental separation (P = .116).
Effectiveness of Various Behavioral Management Techniques Reported by General and Pediatric Dentists
Discussion
This descriptive cross-sectional study compares the different perceptions on the use of basic nonpharmacological behavior guidance techniques between general and pediatric dentists in Saudi Arabia. The findings show that pediatric dentists reported using tell–show–do, positive reinforcement, nonverbal communication, and distraction more frequently than general dentists. Additionally, pediatric dentists reported finding these techniques highly effective compared to general dentists. However, in the included group of participants, the frequency of use and reported effectiveness of voice control, parental separation, and live modeling did not differ significantly between pediatric and general dentists.
The choice of different styles of behavioral management techniques by pediatric dentists may be affected by education, training, comfort, personal preference, availability of devices, financial constraints, parental acceptance, patient acceptance, and legal concerns. 15 Previous studies conducted in various countries have found that tell–show–do is the most common technique used in behavioral pediatric dentistry while by comparison pharmacological techniques including nitrous oxide, sedation, and general anesthesia are used less frequently.15–17
As mentioned above, in Saudi Arabia, the prevalence of dental caries among children is relatively high, 2 whereas the number of licensed specialist pediatric dentists is relatively low. 3 A number of previous studies have found that general dentists can experience stress when performing restorative treatment for young children. 18 Therefore, it is important to promote education and up-to-date information among specialist pediatric dentists as well as general dentists regarding the various types of behavior guidance techniques available. Knowledge, training, and application of these techniques by a dental team as a whole can help treat children in line with the highest standards. 19 It has been found that continuing educational courses considerably improve the perception of behavior guidance techniques among general dentists. 20
The perception of dental students toward behavior management techniques may be influenced by various factors, such as culture, background, education, and training. 21 Dental students show higher levels of acceptance of these techniques after receiving didactic and clinical training courses during study programs. 13 In general, every dentist should have the ability to deal with various types of children visiting the dental clinic, because children can differ naturally in terms of their degree of cooperativeness, which is classified according to Wright into three groups: cooperative, lacking cooperative ability, or potentially cooperative. 17
Adequate assessment of child behavior assists dentists in planning appointments and delivering efficient dental treatment. One retrospective study which included 247 children living in Saudi Arabia found that assessment and evaluation helps dental professionals reinforce their belief in their used techniques. 17 Thus, using the appropriate management techniques can enhance a child’s behavior in dental visits; 17 however, the choice of technique is impacted by parental permission. With parents in Saudi Arabia, it was found that there was a general acceptance to most behavioral management techniques, but those presented with clarification about the possible behavior management techniques that can be used exhibited a higher acceptance level. Also, less educated and younger parents showed higher acceptance levels. 22
In agreement with previous studies, our study shows a difference in the behavior management choices of pediatric dentists and general dentists in treating children.5,7,8,10,11,23 Some studies show that when treating children, pediatric dentists use a wider range of behavior management techniques compared to general dentists. 9
In the present study, the techniques tell–show–do, positive reinforcement, and distraction were the most frequently used among pediatric dentists. In accordance with these findings, a recent cross-sectional study conducted on pediatric dentists across a broad selection of countries in the Middle East region showed that the most routinely used behavior management techniques were tell–show–do (95%, n = 107) and positive reinforcement (89%, n = 101). 24 These results are consistent with the results of Sharath et al. (2009), who found that tell–show–do was the most common technique practiced by postgraduate students in India. 17 Moreover, Bin Saeed et al. 25 found that tell–show–do, positive reinforcement, and distraction were the most commonly used behavior management techniques by dentists in the UK on adults with learning disabilities. This finding is in accordance with the current guidelines and recommendations by the American Academy of Pediatric Dentistry, which promotes the use of “ask–tell–ask,” which can be interpreted as the following: ask to assess patient’s emotional desires, tell a limited amount of information using simple language, and ask to assess patient’s needs, comprehension, and concerns. 26
In agreement with a study by Bin Saeed et al., 25 nonverbal communication, voice control, and live modeling were found used less frequently in comparison to tell–show–do, positive reinforcement, and distraction. However, parental separation appeared to be the least used technique, which is also comparable with the results of Peretz et al. 27 Recently, several modern techniques have been added to the British Society of Pediatric Dentistry (BSPD) nonpharmacological behavior management guidelines, which include child-centered care, magic tricks, hypnosis, memory restructuring strategies, and motivational interviewing. 28 Moreover, the development of additional behavior management technology has been suggested as a necessary strategy by the BSPD.
The present study has highlighted some important differences between pediatric dentists and general dentists in using behavior guidance techniques; however, this study may be limited by its cross-sectional design and it can only show associations and is more limited with respect to inferences of causality. 29 This study included a small sample, which may have led to some bias in analyzing the results as reaching out to each participant directly by both general dentists and pediatric dentists may arguably limit objectivity. The unequal number of respondents was a product of the environmental constraints: there is a lower number of pediatric dentists than general dentists working in Saudi Arabia. Furthermore, not every practitioner is willing to provide information for 10–15 min of their time, which may have been an obstacle in yielding a diverse profile of participants.
Conclusion and Implications
General dentists more commonly reported treating older pediatric patients, while pediatric dentists more commonly reported treating younger pediatric patients. Pediatric dentists reported using the techniques tell–show–do, positive reinforcement, nonverbal communication, and distraction more frequently than general dentists. Pediatric dentists also reported that they found these techniques more effective than general dentists.
Broadly, the information presented in this study may aid in getting a deeper understanding of the nonpharmacological management of pediatric dental patients and could be instrumental in developing ideas and strategies for training and continuing education in the future. This is necessary to promote continual education and updated information regarding the various types of nonpharmacological behavior guidance techniques for specialist pediatric dentists as well as for providing appropriate training to nonspecialist dental professionals.
Footnotes
Acknowledgements
The authors would like to thank the pediatric and general dentists that participated in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Institutional Statement
The study and questionnaire were approved by the Research Ethics Committee of King Abdulaziz University Faculty of Dentistry (Approval No. 099-10-18).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.