
Abstract
Aim:
The aim of this study is to assess the oral health conditions of 8- to 10-year-old students in the mixed dentition stage in Erzurum, Turkey, by determining their dental caries’ status and the soft tissue damages by untreated caries.
Materials and Methods:
The study was carried out in two randomly selected schools in the residential areas populated predominantly by families with mid-and-low socioeconomic levels. A total of 586 children, 275 girls, and 365 boys with a mean age of 8.95 ± 0.8 participated in the study. Number of decayed, missing due to caries, and filled teeth in the permanent dentition/number of decayed and filled teeth in the primary dentition (DMFT/dft) and visible pulpal involvement (P/p), ulceration caused by dislocated tooth fragments (U/u), fistula (F/f) and abscess (A/a) (PUFA)/pufa indices are included in the clinical examination section of the study. Obtained data were analyzed with SPSS (IBM Corp. 2013, IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY).
Results:
Our research revealed a DMFT score of 2.43 ± 1.7, dft 4.12 ± 2.7, pufa 0.75 ±1.2, PUFA 0.05± 0.24, a caries frequency of 96.1, PUFA/pufa frequency of 40.9, and untreated caries PUFA/pufa ratio was found as 13.3%. A significant difference with positive correlation was found between d and pufa scores (P < .01). Increasing DMFT, decayed, missing, and filled surfaces (DMFS) in the permanent dentition, and decreasing dft, decayed, and filled surfaces (dfs) in the primary dentition, and pufa scores with the age increment were found to be significant (P < .05).
Conclusion:
The frequency of soft tissue damage associated with untreated caries, caries index scores, and frequency of dental caries was found to be quite high in the study population consisting of children belonging to families with similar socioeconomic status.
Introduction
Field research studies are conducted globally for identifying the dental caries status of different communities. Prevalence, incidence rates, and some indices such as DMFT/dft are used in these researches.1,2 The DMFT/dft index, which is used for evaluating the oral health conditions, reflects the patients’ existing oral health status; however, they are deficient in revealing the untreated caries-associated pulpal involvement and the presence of the disorders, for example, dental abscess, fistulas, and ulcerations.
In addition to the traditional indices, which present the health condition of the tooth tissue, indices reflecting the soft tissue pathologies should also be used for obtaining more detailed information about the oral health condition. 3 A number of international indices with more sensitive criteria for the early diagnosis of tooth decays were constructed and used in the epidemiologic studies of dental caries, which had been performed in the last decade.
These indices are very advantageous for revealing the specific treatment needs for the different stages of caries formation especially in the populations with high-income levels.4,5 Nevertheless, they are insufficient for determining the pulpal involvements and periodontal tissue damages caused by untreated caries in the communities with mid-and-low income. DMF index, 6 in which missing, decayed, and filled teeth/surfaces have been recorded and has long been used in the epidemiologic studies cannot reflect the caries’ impacts on the tooth pulp, although they provide a crude quantification.
In 2010, PUFA/pufa index was developed by Monse et al. 3 for compensating the limitations of the existing indices. The PUFA index clinically evaluates the oral conditions resulting from the dental decays that remained untreated and records the consequences of pulpal involvements such as pulpal exposure, ulcerations, fistulas, and abscess. 3
This study aimed to measure the oral health conditions in a group of 8–10-year-old children with mid-and-low socioeconomic status and also to assess their untreated carious primary and permanent teeth with the PUFA/pufa index.
Materials and Methods
Setting and Design
This descriptive cross-sectional study had been performed in two state schools in Erzurum from April, 2018 to November 2019. To examine the caries status, soft tissue sequelae (pufa) of untreated dental caries, accumulation of dental plaques, and malocclusions in the children at the age of 8 to 10 years and to measure their oral health conditions. Based on the study data obtained, we plan to evaluate the oral health conditions in our area. Thus, we aim to obtain provincial data for further studies.
Ethics Committee Approval and Formal Consents
This study was approved by the ethics committee of Ataturk University, School of Medicine (no. 4. 10. 2018/B. 30. 2. ATA. 0.01. 00/271) and we obtained the consent of the provincial directorate for national education before starting school dental screening.
Sampling
There were approximately 9000 students at the age of 8 to 10 years in Yakutiye province, Erzurum, Turkey. The sampling size was calculated in Epi Info v7.2.2.6 as 635 at a 95% confidence interval and 3% level of precision and with a 20% estimated prevalence of PUFA/pufa. By adding 10% to the sample size for compensating the sampling errors and probable data losses, we aimed to access 699 students. There were a total of 90 elementary and middle schools in Yakutiye province. In this study, we planned to include eight third grade classes, nine fourth grade classes, and six fifth grade classes from the participant schools. Schools and classes were chosen randomly. Participating schools and classes were chosen with simple random sampling. Subject students from the classes were included with a stratified sampling method and with proportionate allocation.
Indices Used
In this study, DMFT, dft, and PUFA/pufa indices were used.
DMFT index: Number of decayed, missing because of caries, and filled teeth in the permanent dentition.
dft index: Number of decayed and filled teeth in the primary dentition.
PUFA/pufa index: The presence of severely decayed teeth with visible pulpal involvement (P/p), ulceration caused by dislocated tooth fragments (U/u), fistula (F/f), and abscess (A/a). Uppercase letters were used for the perma-nent dentition and lowercase letters were used for the primary dentition.
Respondent Recruitment
Parents were provided with the informed consent forms, which included a description of the procedures to be performed and a statement that they fully understood the medical examinations to be applied. Children with any systemic diseases, which will restrain them to maintain their oral hygiene or routinely receiving medications, children with special needs and with communication problems, and also children who would not like to participate were excluded from the study.
Research Variables
The independent variables: Social: Age, gender, number of siblings, residential area, and parents’ income levels. Medical: Height, weight. Dental: Whether the children have their own toothbrushes or not, do they visit the dentist’s office, and frequency of their dental visits, tooth-brushing frequencies.
The dependent variables: OHI-S, DMFT/dft, DMFS/dfs, and PUFA/pufa indices for assessing the clinical findings.
Data Collection Tool
Study data were obtained from the demographic survey questions and from the examination forms assessing the oral health conditions. We received help from senior grade dental school students to fill out the examination forms in order to avoid any probable data losses.
Workforce
In epidemiologic research studies, training and calibration of medical examiners are very important for a quality and reliable study and for consistent examination data. 7 All examinations were made by a single dentist (Berrin Deniz Gören), attending the pediatric dentistry residency program. Prior to the study, she was trained by another dental specialist (Sera Şimşek Derelioğlu; SD). Examiner calibration was done in 50 school children. Inter-examiner reliability yielded a Kappa value of 0.95 for the examiner. Intra-examination reliability of the examiner, which was evaluated in the same children with 10-day intervals was high and the Kappa statistic was 0.93.
Data Collection Method
Demographic characteristics and oral health findings of the children were recorded in the dental examination forms. Obtained data were analyzed with SPSS v22.0.
Clinical Examinations and Quantifications
The chapter “Clinical examinations” of the study consists of data about oral health conditions. DMFT/dft, DMFS/dfs, PUFA/pufa, OHI-S indices, are also included in this section. Dental examinations were performed in the classroom conditions by using a penlight, a mirror, and a periodontal probe recommended by WHO for use with Community Periodontal Index (CPI; WHO 973/80-Martin, Solingen, Germany). The dentists who conducted the examinations reported the carious teeth and surfaces to the senior grade dental school students to be recorded in the examination forms.
Statistical Analysis
SPSS v22.0 was used for assessing the study data. Qualitative variables were presented in numerical values and in percentages whereas quantitative variables were presented in mean absolutes and standard deviations. Kolmogorov–Smirnov test, calculated z-scores of skewness and kurtosis, and graphical methods were used for verifying whether quantitative values follow a normal deviation. Mann–Whitney U and Kruskal–Wallis tests were used for inter-group comparisons of discrete quantitative values. We used Spearman’s Rho test to measure the association between discrete quantitative and ordinal values. P < .05 was found to be statistically significant.
Results
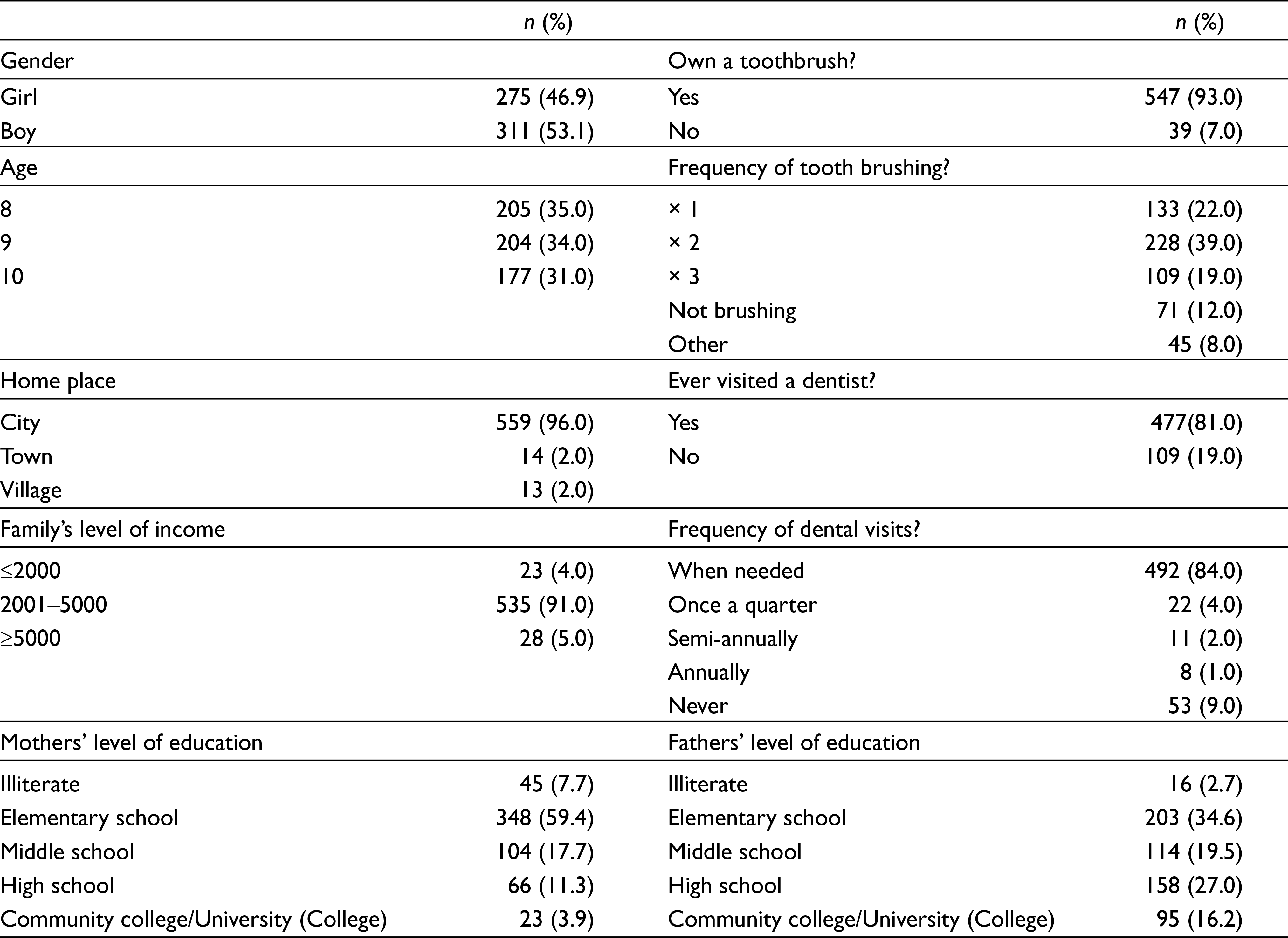
A total of 586 students were included in the study (participation rate: 84%). Their sociodemographic data are shown in Table 1. Students had an average of 2.69 ± 1.27 siblings in their families, they had an average height of 135.4 ± 6.6 cm (53 – 5⁄16 ± 2 – 39/64 in), and they weighed an average of 30.7 ± 5.9 kg (67 ± 13 lbs).
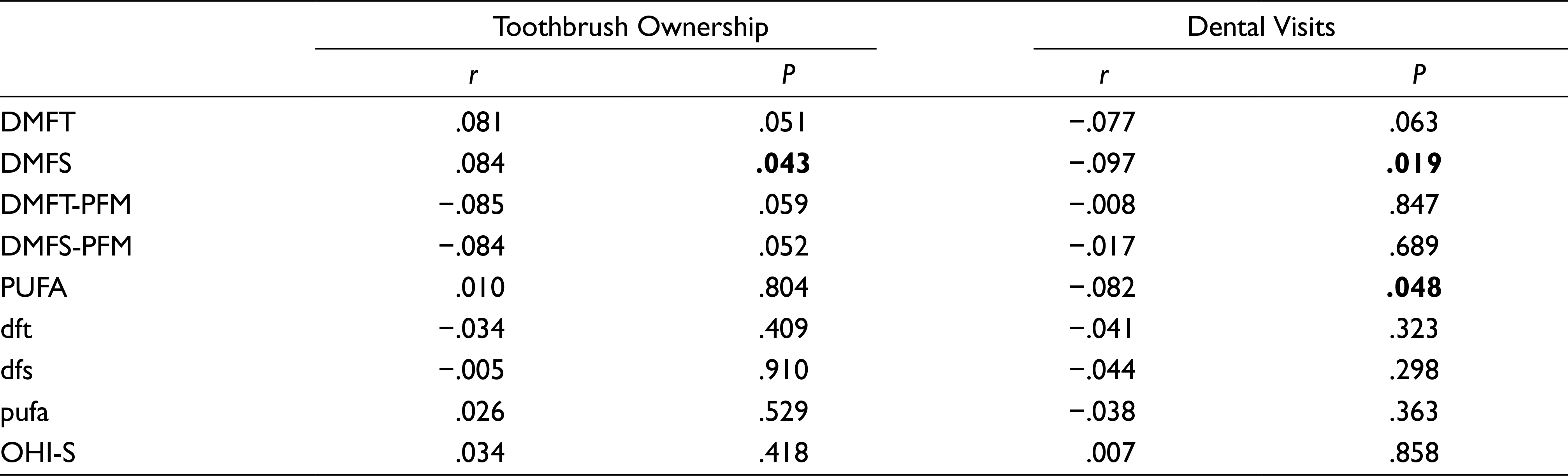
No statistically significant correlation was found between the parents’ levels of education and index data (DMFT, dft, DMFS, dfs, DMFT- Permanent First Molar (PFM), DMFS-PFM, PUFA, pufa) (P > .05). There was a statistically significant, weak positive correlation between DMFS indices and the ownership of a toothbrush among the students (r = 0.084, P = .043). Besides, we found a statistically significant, weak negative correlation between the students’ dental visits and DMFS (r = −0.097, P = .019) and PUFA (r = −0.082, P = .048) indices scores. Correlation between the index values and students’ toothbrush ownership, and their dental visit status are given in Table 2.
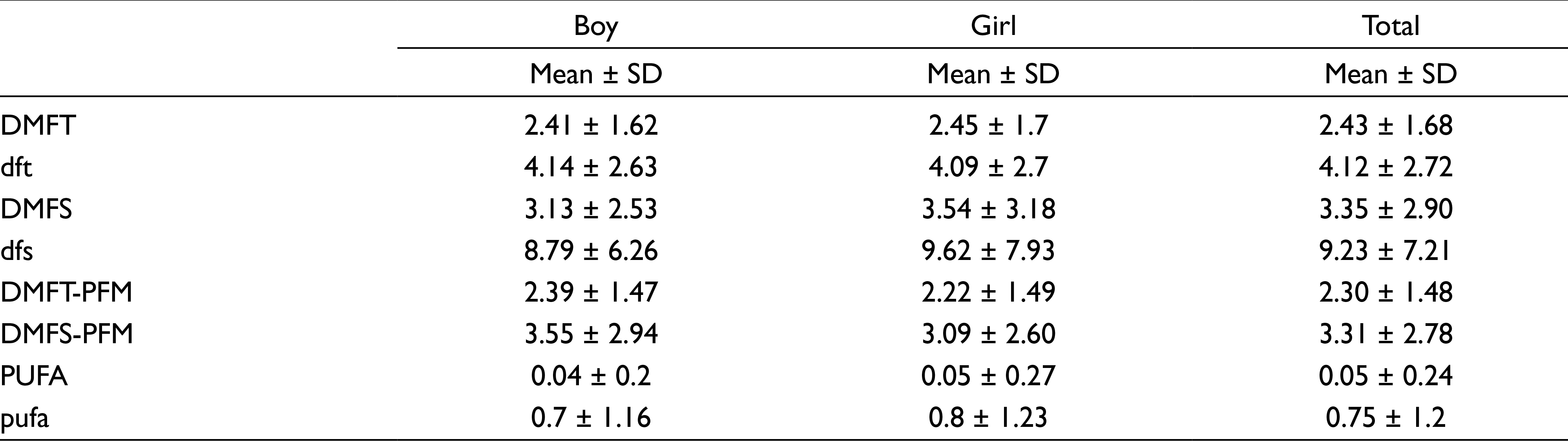
When indices data (DMFT, dft, DMFS, dfs, DMFT-PFM, DMFS-PFM, PUFA, pufa) were compared in regard to gender in the students, no statistically significant difference was found (P > .05; Table 3).
Frequency Distribution of the Children’s Sociodemographic Characteristics
Correlation Between the Index Values and Students’ Toothbrush Ownership, and Their Dental Visit Status
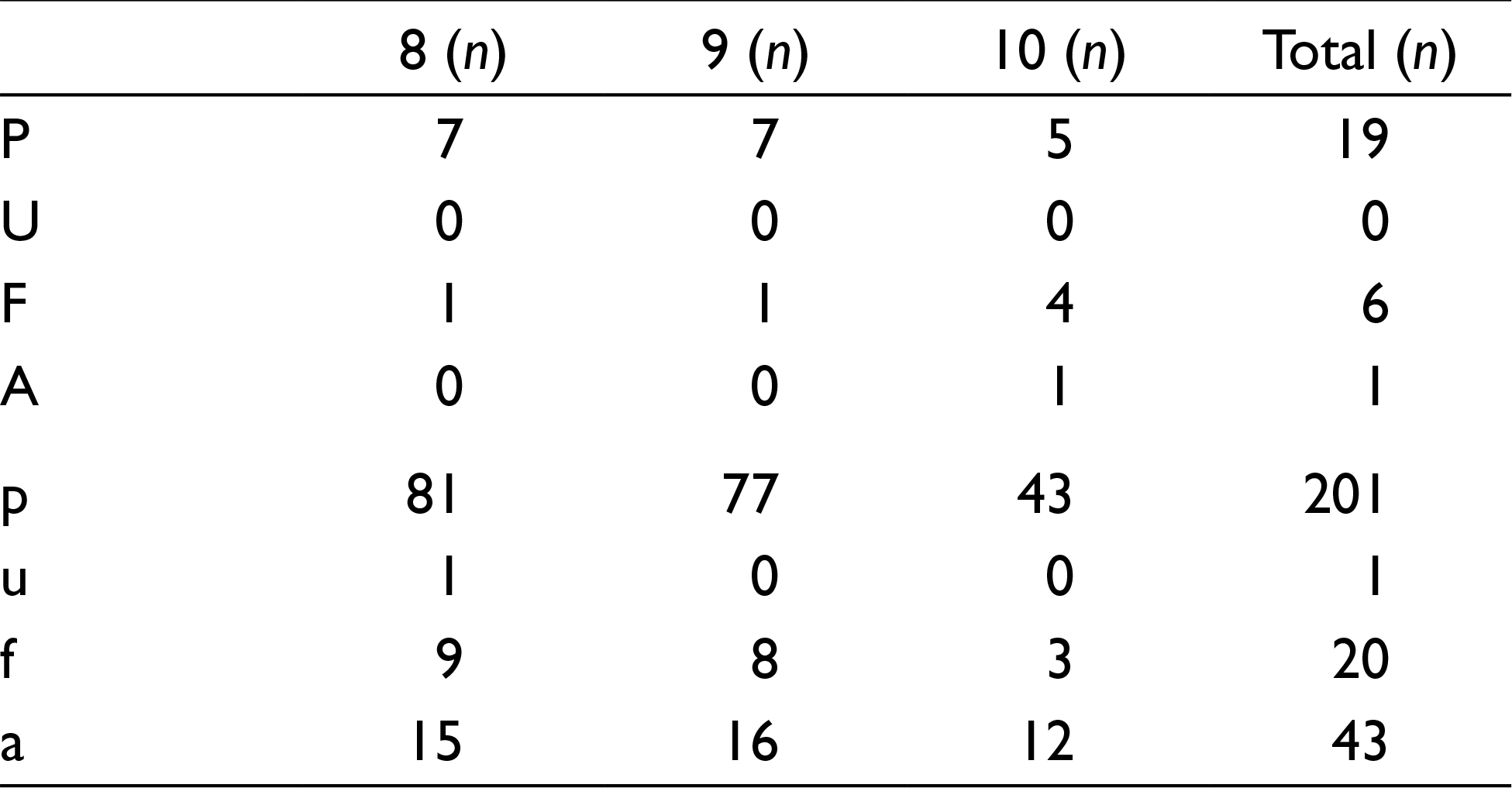
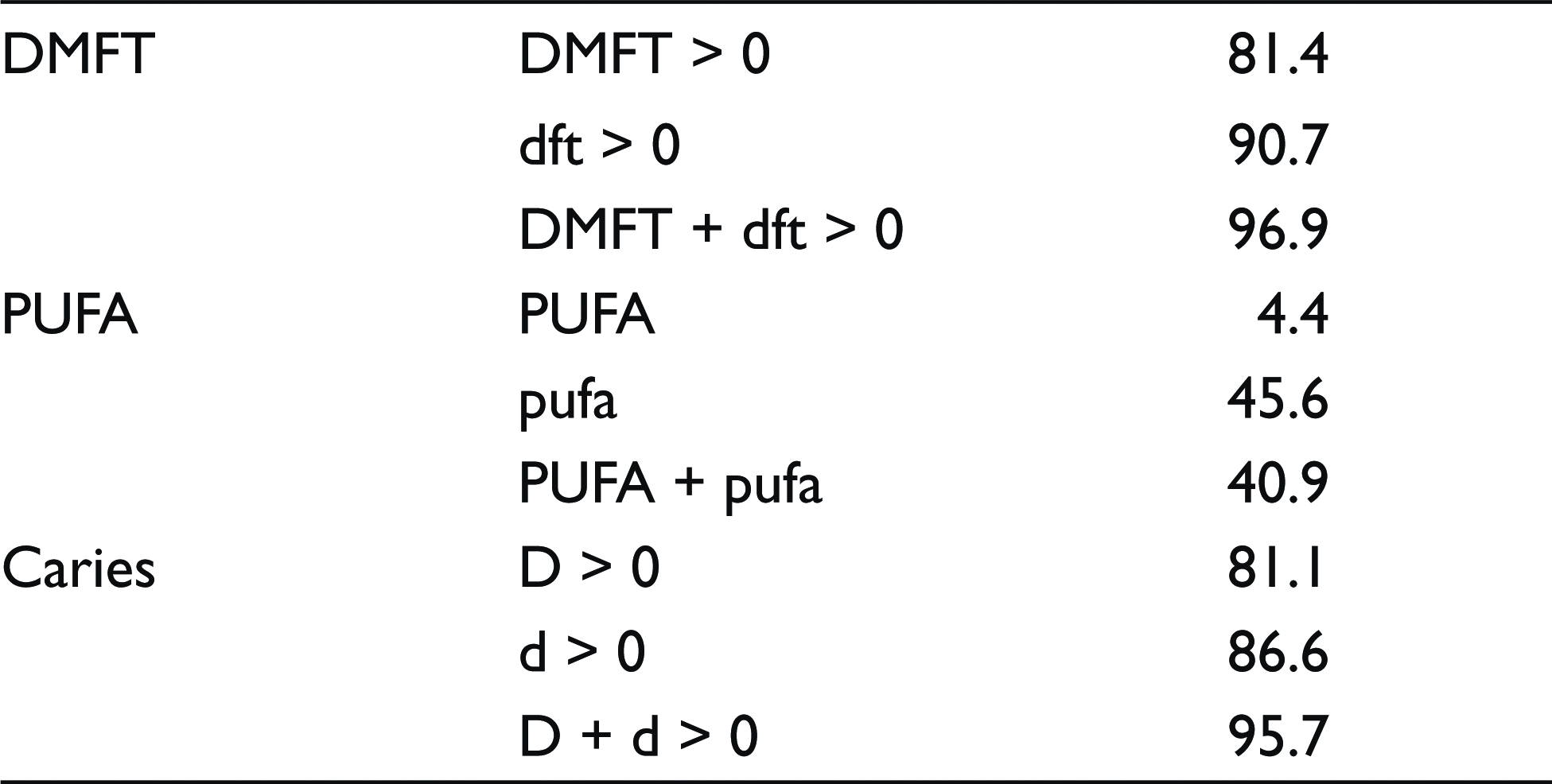
We evaluated PUFA/pufa index system codes with respect to the age groups (Table 4) and observed an increase in F code whereas there was a decrease in all pufa codes in the primary dentition. DMFT/dft and PUFA/pufa frequencies of the participating children are shown in Table 5.
Among the participating kids, the percentage of PUFA/pufa values = min 1 or > 1 was observed as 45.6% for the primary and 4.4% for the permanent dentitions. However, untreated caries PUFA/pufa ratio, which is significant in regard to disclosing what percentage of untreated dental caries results in pulpal involvement, was found as 13.3% for both primary and permanent dentition, which was 2.2% for permanent, and 20.2% for primary dentition.
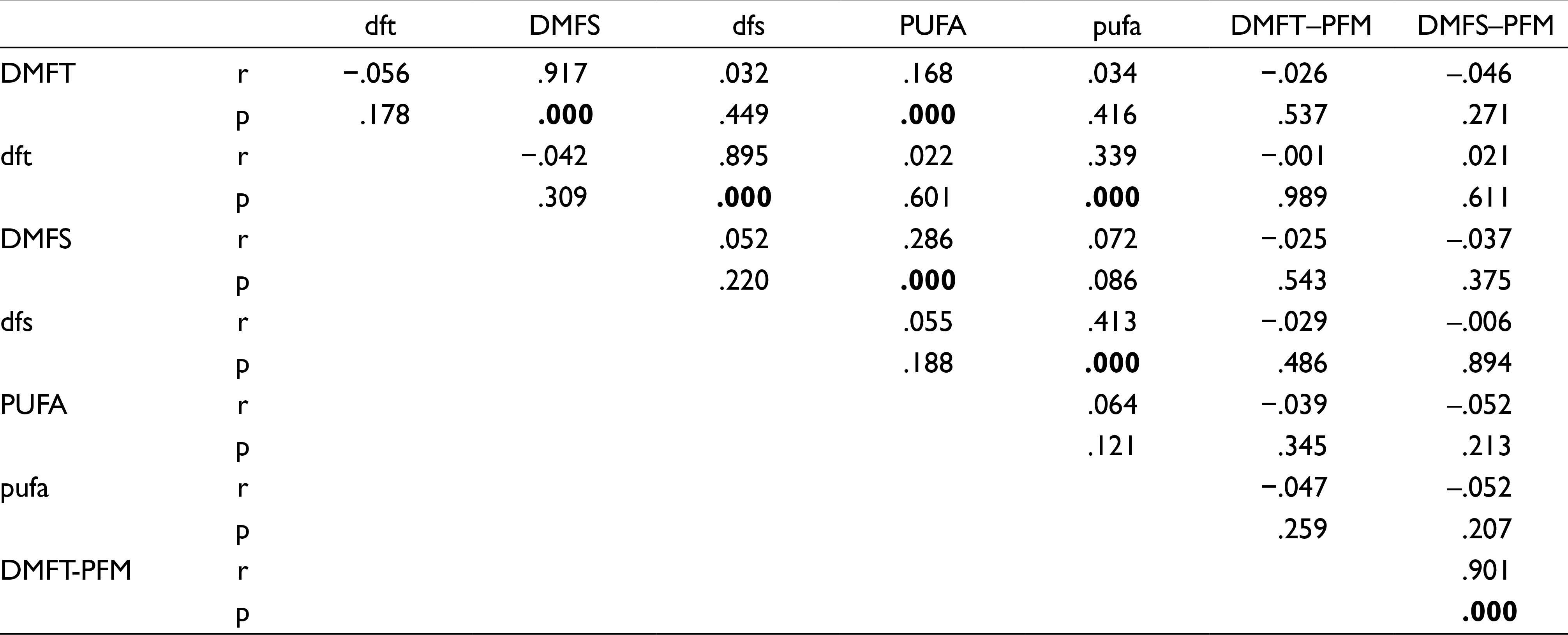
We observed a statistically significant moderate positive relationship between d score and pufa (r = 0.388, P < .001); pufa values increased with an elevation in d scores. On the other hand, we found that the age was positively associated with DMFT and DMFS indices (r = 0.214, P < .001 and r =0.219, P < .001 respectively) and yet, it was negatively associated with dft and dfs indices (r = −0.269, P < .001, r = −0.201, P < .001, respectively). Correlations between the indices used in this study were found to be statistically significant (Table 6).
Distribution of Indices Data Regarding Participants’ Genders
Distribution of PUFA/pufa Codes in the Permanent and Primary Dentition Regarding the Age Groups
DMFT/dft and PUFA/pufa Frequencies of 8–10-Year-Old Children (%)
Correlations Between the Indices
When we evaluated OHI-S of the participating students, 439 (74.9%) children showed regular, 93 (15.9%) showed bad, and 54 (9.2%) showed good results.
Discussion
In WHO oral health reports, dental caries affecting the children in early/late childhood, in adolescents, and adults was defined as a major public health issue. 8 Early childhood caries promotes caries activity in late childhood, adolescence, and adulthood. DMFT/dmft indices have long been used in dental epidemiological studies for assessing the impact of caries on public health.9–11 Nevertheless, these indices have some limitations in reflecting the negative impacts of dental caries on public health and its consequences because they do not express the caries severity. 12 PUFA/pufa index, introduced by Monse et al. in 2010 for eliminating those drawbacks, provides more accurate and elaborate information about the clinical consequences of untreated caries.3,13
PUFA/pufa index codes are: pulpal involvement, ulceration of soft tissue caused by root fragments, fistula, and abscess; thus PUFA index can score the effects of permanent damage caused by untreated caries unlike DMFT index which records the presence of the decayed permanent teeth with D. While PUFA index is needed in developing and under-developed countries for scoring the effects of untreated dental caries, DMFT indices may be sufficient in the developed countries where preventive noninvasive treatments have gained priority. PUFA index may also be considered as a supplementary tool for the DMFT index. 3
PUFA/pufa index is easy and reliable to use, it can be swiftly performed without any additional training and tools. 3 This index had been used in previous studies involving children with high caries prevalence, whose families lived in low-income areas.14,15 In this research, we considered that besides other indices, PUFA/pufa index should also be evaluated in the children with low–middle sociocultural level, who were recruited from the schools in Yakutiye, Erzurum.
High caries prevalence found in a previous study performed in Erzurum with 4–6-year- old children drove us to think about the oral health status of the children in early mixed dentition. 9 Children of 8 to 10 years of age constitute the first two stages of mixed dentition. As a result of our literature review, we did not find any study revealing the experience of dental caries or the consequences of untreated caries in the 8 to 10 years old children in our area. With our research, we aimed to evaluate caries and caries-associated clinical problems in 8- to 10-year-old children with no systemic disease. In addition to DMFT/DMFS, dft/dfs, DMFT-PFM/DMFS-PFM indices, PUFA/pufa index was also used for clinical assessment in this study.
Several situational analysis studies in oral and dental health have been conducted in the world and Turkey. In those researches, DMFT/dft and PUFA/pufa data were evaluated with mean scores.3,11,16 A study conducted in Poland, surveying the children in 5- and 7-years age groups, has reported that pufa scores also increase in parallel with higher dmft values in both ages. 14 Similarly, we also observed a significant increase in pufa/PUFA index along with an elevation in dft/dfs, DMFT/DMFS indices in this study. No statistically significant difference was found in the correlation analyses performed between DMFT and dft, dfs, pufa, and DMFT-PFM values; also between dft and DMFS, PUFA, and DMFT-PFM data. Additionally, no correlation was observed when a correlation analysis was used between PUFA and DMFT-PFM values. When we searched the impact of caries in the primary teeth of the participants (d) on PUFA/pufa indices, we found a significant correlation only between the pufa values. A positive correlation was observed between d scores and pufa values.
Another parameter evaluated in our study was the “untreated caries PUFA/pufa” ratio that was first indicated as 40% for 6-year-old children and 41% for 12-year-olds in a study by Monse et al. 3 in which 4052 Filipino children at the ages of 6 and 12 were included. As opposed to this study, untreated caries resulted in pulpal involvement with a ratio of 13.26% in our study: 2.2% for permanent dentition and 20.2% for primary dentition. We thought that the difference between the results of the two studies was related to the study populations in different age groups.
Since our research included children in mixed dentition, we observed a lower dft score due to the early loss of primary teeth, and thus, we found a lower pufa ratio than the former study. Yet, because of our study’s age group, we observed a lower PUFA score than the ratio, which Monse et al. reported for the permanent dentition.
Many research studies conducted around the globe and across Turkey have so far presented the prevalence of dental caries in the populations. In a 2019 study, consisting of 6- to 16 years old South African children in Tshwane, Molete et al. 16 expressed a caries prevalence of 25.9% for 8- to 10-year-olds in permanent dentition and 30.2% in the primary dentition. They also reported a PUFA prevalence of 2.2% for permanent dentition and 5.5% for primary dentition. We believed that the difference between the two studies was because the former research studies included only 35 children in the age group of 8 to 10.
The dmft/ DMFT and pufa/PUFA scores were reported as 82.7%, 42.7%, 25.9%, and 3.8%, respectively, in a research performed with the children at 6- to 16 years age group in Iran in 2017. 17 In a 2013 study conducted in Nigeria, Oziebge et al. 13 reported prevalence values for the 7- to 12-year-old children as; prevalence DMFT > 0 = 3.6%, prevalence dmft > 0 = 6.5%, prevalence pufa > 0 = 2.6, prevalence PUFA > 0 = 1.4, overall caries prevalence = 10.1%, and overall prevalence of PUFA/ pufa = 4.0. We found higher scores than Oziebge et al., 13 because our study consisted of data from the children with mid-and-low socioeconomic status. Jarzawi 18 presented an overall PUFA/pufa prevalence of 37.8% for 7- to 8-year-old children in 2014. We presume that their higher prevalence ratio might be associated with the different age categories of the study populations.
When we reviewed the relevant literature published in Turkey, we noticed that in a study carried out in Ankara in 2018, Aktas et al. 19 reported a PUFA prevalence of 0.7%, pufa prevalence 4.08%, and an overall PUFA/pufa prevalence of 4.78% for an age group: 8– to 10-year-olds. We also identified that in another research 20 conducted in Adana evaluating the oral health conditions of school kids at the age group 6 to 11 years, caries prevalence was reported as 69.2% whereas Altun et al. 10 presented a DMFT and dmft caries prevalence of 71.2% for again 6- to 11-year old children in a study performed in Ankara. Guler et al. 11 announced a caries prevalence of 82.6% in a study for 7- to 14-year-olds in Malatya. Because our study included only a group of children with low socioeconomic status, caries prevalence was not determined; however, caries prevalence was calculated as 95.7%. The main factors for observing different results in those researches might have been the study populations consisting of children from different cities and from different socioeconomic levels. Nevertheless, different age groups might also have affected the results.
In a 2018 study conducted in Ankara, Aktaş et al. 19 , reported for 8- to 10-year-olds that dental caries with pulpal involvement (p) was found to be the highest pufa score in the primary teeth (11.24%) whereas ulceration (u) and abscess (a) were observed as the lowest.
Similar to our findings, in a study performed in 2017, assessing the relationship between verbal bullying and untreated dental caries in 8- to 10-year-old Brazilian children, Barasual et al. 21 stated that the presence of “P” code had the highest score of 13.3% whereas the presence of “U” code had the lowest score of 0.4%. Considering that PUFA/pufa index was a very suitable tool for assessing the neglected oral health status in that study, we also used PUFA/pufa index in research for evaluating the dental neglect in children from mid-and-low socioeconomic status families. Although we did not search in this study, it is important for the dentists to evaluate the pieces of evidence of child abuse and neglect in children with high pufa/PUFA scores. PUFA index should also be included as a supplementary tool for the DMFT index in the field studies conducted in developing and under-developing countries.
Limitations
However, the research is based on a representative sampling size, it consists of the school children in only Yakutiye province of Erzurum.
Conclusion
The results of our small sample research revealed the importance of oral hygiene awareness training for parents and kids in order to improve oral hygiene in children with high PUFA/pufa scores from the schools in low socioeconomic areas. Thus, oral health training and dental screenings should be frequently performed in schools located in low socioeconomic areas. For more sensitive assessments, along with the DMFT/dmft scoring system, PUFA/pufa index should also be used in these dental screenings. The effectiveness of the protective approaches promoted with oral hygiene training should be enhanced in order to decrease dental caries and to stop their progress, and thus to achieve the regional WHO goals.
Footnotes
Author Contributions
Berrin Deniz Goren: Scanning archive data, examination of patients, and manuscript preparation. Sera Şimşek Derelioğlu: Study design, scanning archive data, and manuscript preparation. Sinan Yilmaz: Statistical analyses and manuscript preparation. All authors contributed to the article and approved the submitted version.
Ethical Policy and Institutional Review Board Statement
This study was approved by the ethics committee of Ataturk University, School of Medicine, (No. 4. 10. 2018/B. 30. 2. ATA. 0.01. 00/271) and we obtain the consent of the provincial directorate for national education before starting school dental screening.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.