
Abstract
Aim:
To compare the perspective of orthodontists and laypersons on the effects of orthodontic treatment on facial aesthetics in young Classes I, II, and III Turkish patients.
Materials and Methods:
In this cross-sectional study, a total of 60 patients (30 males and 30 females, 9 to 17 years of age) was included using randomization in strata and then divided equally (n = 15) into four groups according to the Angle classification. Photographs during frontal and lateral resting and also smiling were obtained from each patient before and after orthodontic treatment. A panel consisting 50 laypersons and 50 orthodontists was invited for the evaluation of the initial and final photos by using the visual analogue scale and a five-point scale to determine similarities and differences of their perspectives in the effects of orthodontic treatment on facial aesthetics. The data were analyzed by independent t-test, one-way analysis of variance, and Pearson’s correlation test.
Results:
The evaluation of facial aesthetics and treatment changes were not affected by the age and gender of the panel members (P <.05). Angle Class III patients were given lower scores by both orthodontists (P < .001) and laypersons (P < .05), but no significant differences were found between any of other classes (P >.05). Orthodontists reported greater improvement for Class III than in Class II Division 1 (P < .05) however laypersons did not notice the changes after orthodontic treatment for any of Angle classes (P >.05).
Conclusion:
Class III patients received lower scores for aesthetics from both panels. Laypersons may not be concerned about the effects of orthodontic treatment on facial aesthetics in patients with any Angle class. Orthodontists have seen more facial aesthetic changes after orthodontic treatment in Class III patients.
Introduction
Facial beauty has gained significance in daily social life recently. It has been reported to have positive effects on mental health and social behavior, and also provides advantages during education, job prospects, and interpersonal relations. 1 The mouth and teeth are the significant determinants of facial esthetics. 2 During communication, attention has been reported to be focused on the mouth of a person during talking. 3 Therefore, orthodontic treatment may gain significance in terms of esthetic improvement. 1 Patients and their families have been reported to expect to become more attractive by having straight teeth and a nice smile with orthodontic treatment. 4 Similarly, orthodontists have been also found to have similar anticipations from orthodontic treatment in terms of aesthetic improvement of the patient’s face which may affect the treatment plans. 5
Controversial results between orthodontists and laypersons have been reported in terms of their perspective to facial esthetics in the literature.6–9 Some studies have suggested that orthodontists are more critical,10,11 but others12,13 have reported the superiority of laypersons. In addition, studies without differences between orthodontists and laypersons were also presented in the literature.14,15 These differences in perception may diminish the satisfaction of patients and their families. Therefore, the determination of perceptions of orthodontists and laypersons may be a significant factor which may affect the outcome of orthodontic treatment. However, studies which compare the perspectives of laypersons and orthodontists on the effect of orthodontic treatment on facial esthetics are limited in the literature. Therefore, the purpose of this study was to evaluate the perceptions of orthodontists and laypersons on the effects of orthodontic treatment on facial esthetics by using visual analogue scale (VAS) and a five-point scale in Turkish adolescents with different Angle classes.
Materials and Methods
This cross-sectional study used the scanned records of Turkish adolescents from the same region, aged from 9 to 17, who applied to the Department of Orthodontics, Faculty of Dentistry at Selçuk University between 2000 and March 2008. A written informed consent form was obtained from the parents or guardians of all the participants. Patients were included if they had no severe malocclusion; no dental or facial trauma; no missing, extra, or malformed teeth; no surgical treatment need; no dental malformation or deficiency in anterior dentition; or any previous history of fixed orthodontic treatment. Orthodontic treatment results were evaluated with the peer assessment rating index, and individuals who were treated very well according to this index were included in the study. To determine the sample size for each group, a power analysis was carried out based on an alpha significance level of 0.05 and a beta value of 0.1 to achieve 90% power (version 3.0.10, G*Power; Franz Faul Universidad, Kiel, Germany) and it was calculated that minimum 20 patients for each group would be necessary.
More than 2,000 patients were screened, and 60 patients (30 girls and 30 boys; mean ages: 12.96 ± 1.70) according to Angle classification and gender were included in the study using randomization in strata (Table 1). The patients were divided into four equal groups using the Angle classification 10 : Class I, Class II Division 1 (Class II/1), Class II Division 2 (Class II/2), and Class III. The types of treatments and the severity of the malocclusions in the patients were not considered as in a previous study, 16 because the aim was to examine only the changes in facial esthetics after orthodontic treatment.
Age Distribution of the Patients With Postadded Two Patients, According to Angle Classification and Gender

Reference Photo Selection
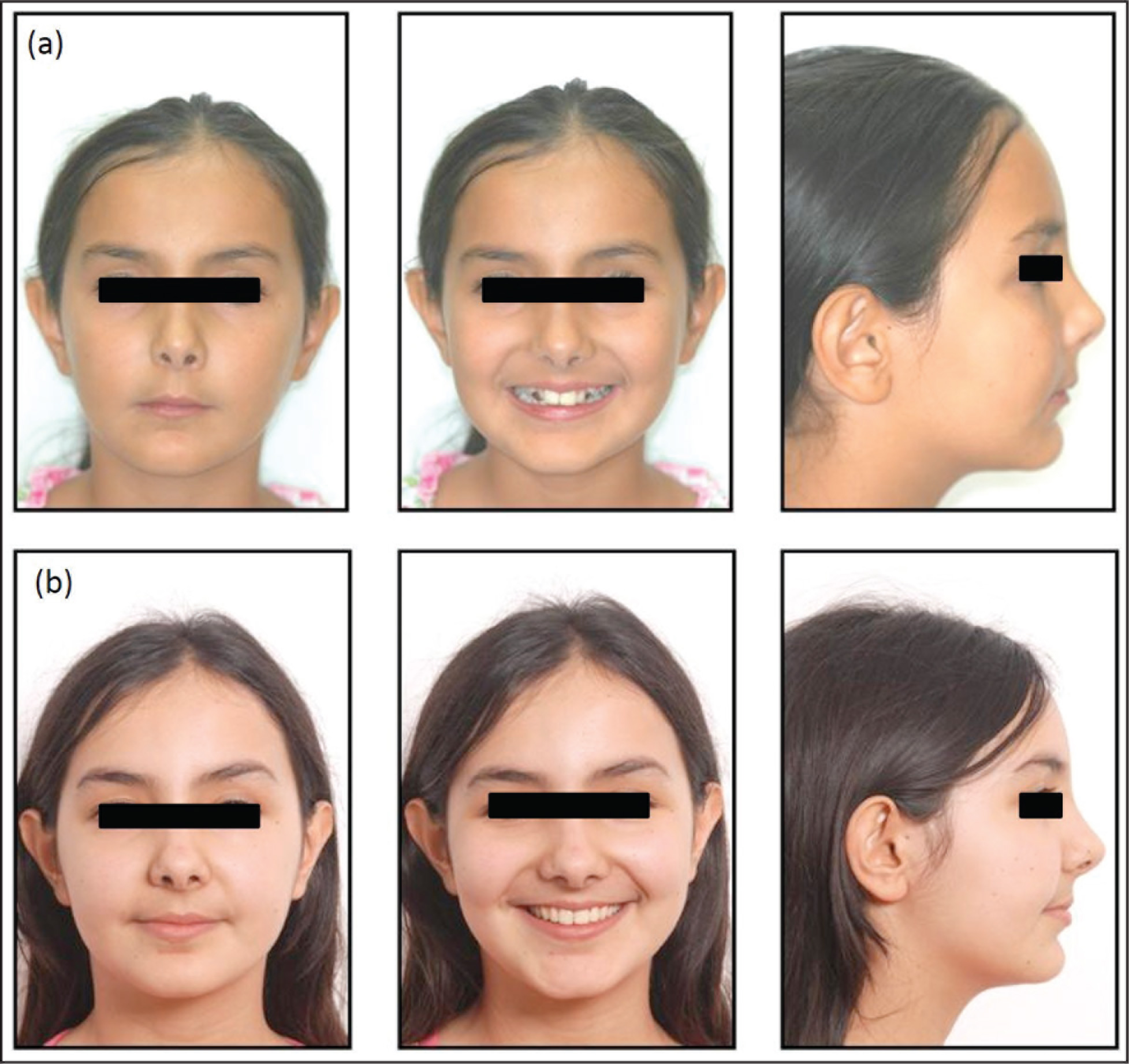
For the VAS measurements, separate reference photographs were first selected for the girls and boys and then all photographs were scored using the reference photographs. A slide showing a combination of photos of pretreatment frontal resting, frontal smiling, and lateral resting was prepared for each patient, and 60 slides were projected onto a curtain screen in random order. A total of 50 dental students [25 females and 25 males, aged from 19 to 26 years (mean: 21.46 ± 1.28 years)] voted on the photos of the slides, according to their perceptions of facial esthetics, using VAS from 0 to 100. Each slide was projected for 10 s, and no additional information was given about the patients before or during the presentation. Photograph series with mean scores that were close to the general mean of 3,000 (50 students × 60 patients) were preferred as the reference photos (one photograph series for males and another for females) for 60 sets of photographs (Figure 1A, B). After the slides had been shown, the reference photos were added to each photograph series, according to gender, to make the real measurement system (Figure 2A, B).
Reference Photographs for Girls (A) and Boys (B)
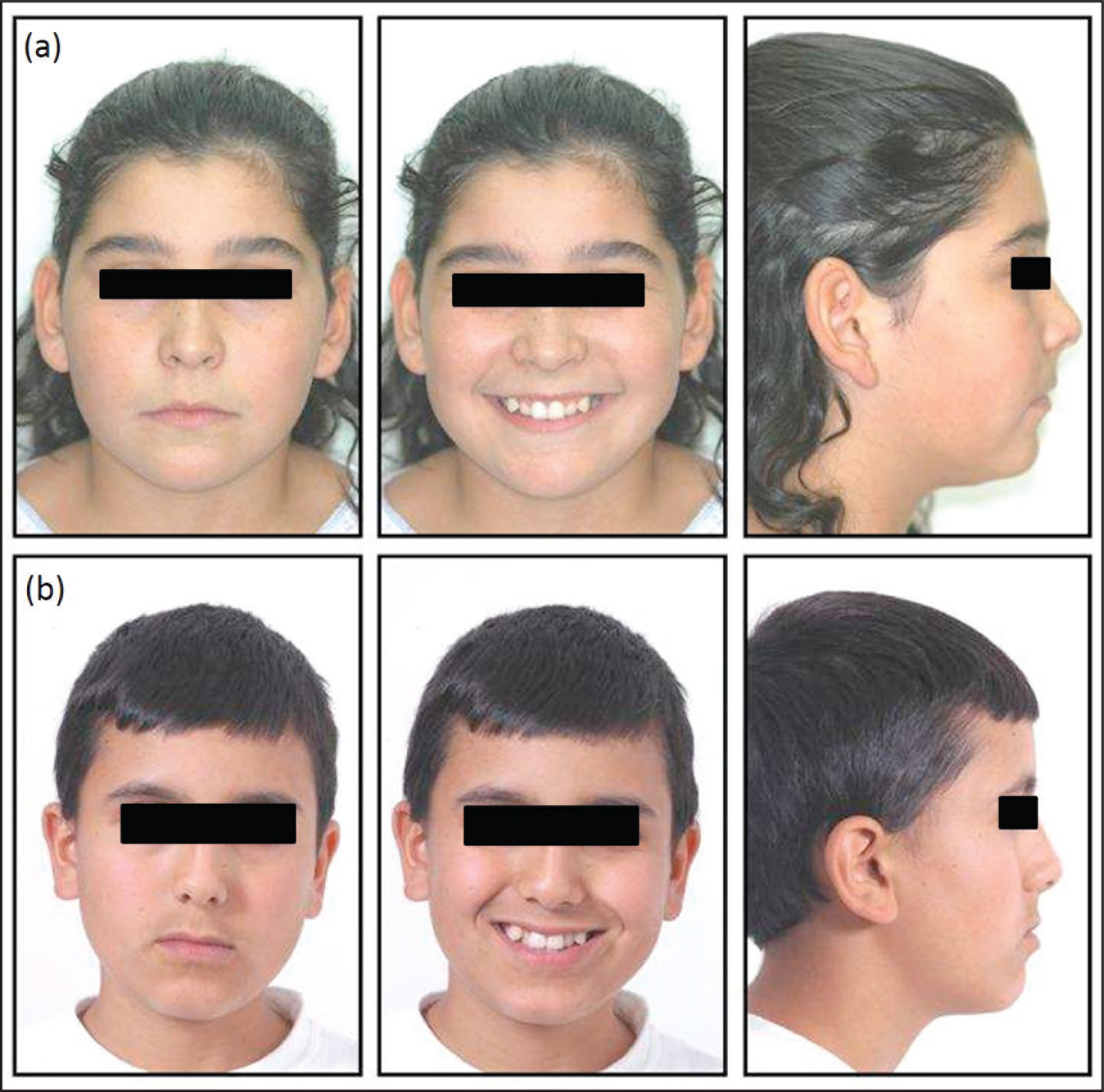
Scored Patient Photographs (A) and Reference Photographs (B)

Selection of Participants
To rate patient photographs, two separate panels were formed consisting of 50 orthodontists [29 females and 21 males, aged from 30 to 64 years (mean: 42.39 ± 4.48 years)], who had graduated from orthodontic training, and 50 laypersons [25 females and 25 males, aged from 30 to 51 years (mean: 42.33 ± 8.88 years)], who were university-educated but had not studied dentistry (Table 2).
Age Distribution of the Panel Members, According to the Panel Group and Gender

Determination of VAS Score
The slides of all patients were randomly arranged on a wall in the form of a slide show, with the help of the Microsoft Office PowerPoint (Seattle, Washington, USA) program. Three photographs of each patient, with three reference photographs of the same slides, were shown to panel members for 10 s. Members were requested to vote on the pretreatment photo series using the VAS score in a range of 0 to 100 (from very unattractive to very attractive), according to their esthetic perceptions. A vertical line showing 50 points was used as a guide at the center of the scale to help the panel members.
Determination of Five-Point Scale
Pre- and posttreatment triple photographs were then shown immediately for evaluation of the treatment changes, and each slide was shown for 10 s (Figure 3A, B). Evaluations were made using the five-point scale described by Kiekens et al. 16 : (a) Much worse (–2), (b) Worse (–1), (c) No change (0), (d) Improved (1), and (e) Much improved (2). Test scores were assigned using the selections made by each panel member for each patient. Photographs of six patients (numbers 15, 23, 27, 31, 36, and 37) were shown twice to the panel members to measure intraindividual repeatability of the measurement system. Panel members received no extra information about the patients during the screenings. The duration of the study was three months.
Pretreatment (A) and Posttreatment (B) Photo Sets
Statistical Analysis
The Cronbach’s α coefficient was calculated to measure the internal consistency of the VAS scores and test measures. Pearson’s correlation test was used to measure intraindividual repeatability of the VAS scores and test measurements between the first and second scores. An independent t-test determined the differences in the VAS scores and test measures between boys and girls, one-way analysis of variance determined the differences between the Angle classes, and Tukey’s Honestly Significant Difference (HSD) test was chosen for finding the sources of these differences. Analysis of variance was also used to determine a comparison between the VAS and test scores and the ages, genders, and professions of the panel members. Spearman’s correlation test was used to measure the interpanel repeatability of the VAS and test scores. In addition, Pearson’s correlation test was conducted to examine the intragroup effect of the panel members’ ages. The data were analyzed using the SPSS software (version 17.0; IBM, Chicago, IL). A P value less than 0.05 was accepted as the significant level in all evaluations.
Results
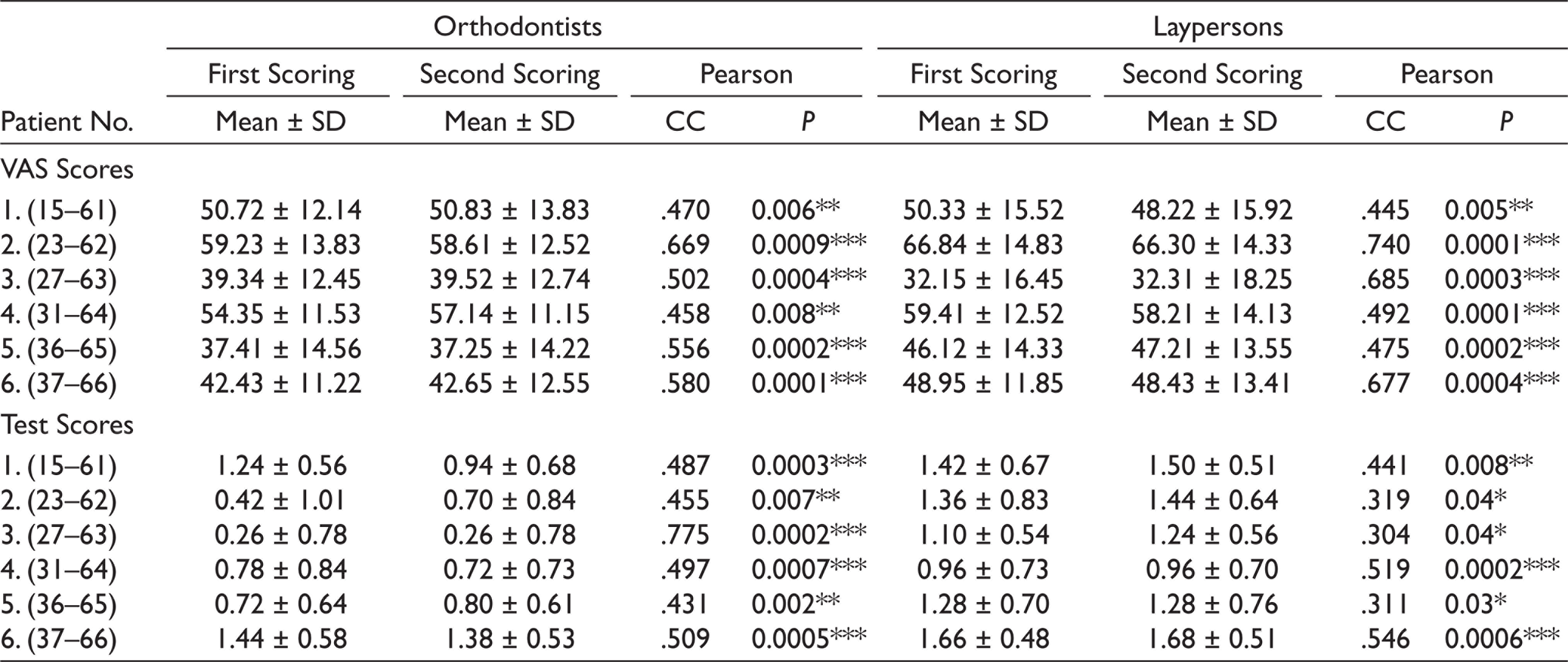
When the internal consistency of the VAS and test scores was calculated, Cronbach’s α was 0.916 and 0.880 for the orthodontists and 0.957 and 0.950 for the laypersons, respectively. Pearson’s correlation coefficient was calculated, and repeatability was found to be statistically significant for both panels (Table 3). No significant differences were found (P >.05) between the genders of the patients, according to both panels (Table 4).
The Repeatability of Intraindividual VAS and Test Scores Between First and Second Scoring
The Comparison Between the Patients’ Gender to the VAS and Test Scores of Panel Members
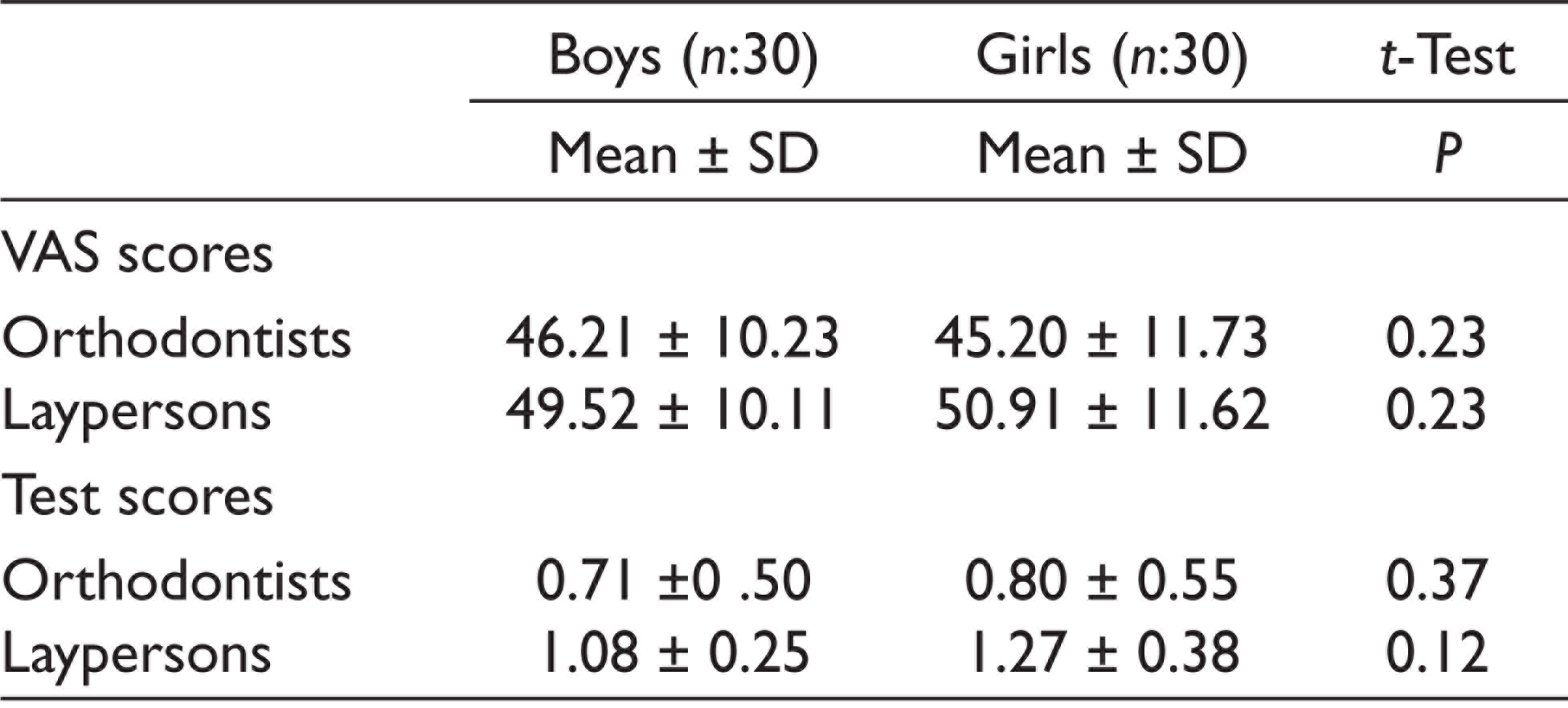
P, significance; t-test, independent t-test.
Results of VAS Score
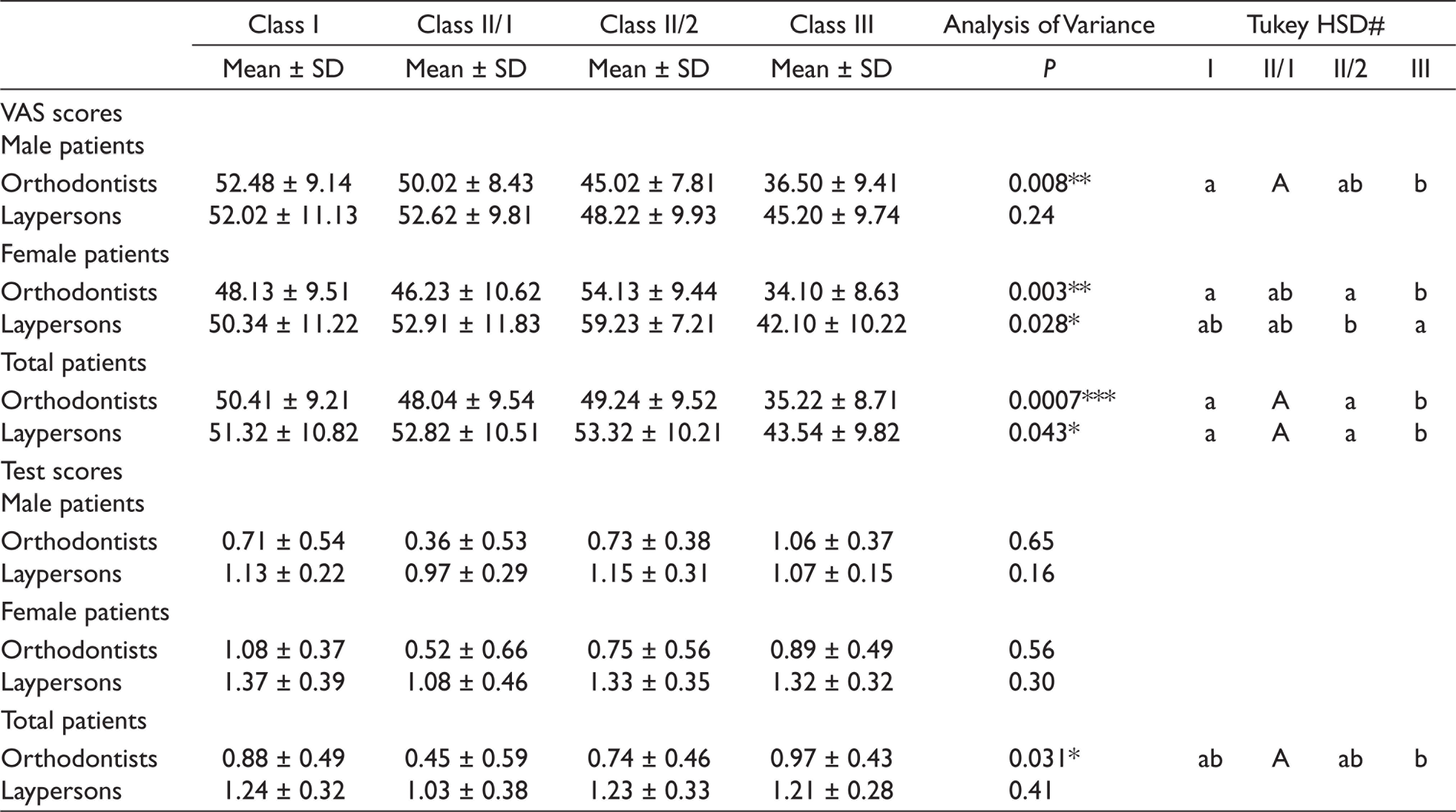
When the boys (n = 30) were evaluated with respect to the Angle classification, no significant differences were found between this classification for laypersons (P >.05). Orthodontists gave lower scores to Class III male patients than to Class I and Class II/1 male patients (P = .008), and there were no significant differences between Class II/2 and the others (P >.05; Table 5). Orthodontists also gave lower scores to Class III female patients than to Class I and Class II/2 female patients (P = .003), and there were no significant differences between Class II/1 female patients and the others (P >.05; Table 5). However, the laypersons gave lower scores to Class III female patients than to Class II/2 female patients (P = .028), and there were no significant differences between Class I and Class II/1 female patients and the others (P >.05). In addition, when considering the overall patients (n = 60), significant differences were found between four Angle classes for both orthodontists (P < .001) and laypersons (P = .043). According to both panels, Class III patients had lower scores than the others, but no significant differences were detected between the other groups (Table 5).
Results of Five-Point Scale
Considering the Angle classification, according to orthodontists, there were no significant differences in the changes after treatment in the male and female patients (P >.05), but there were significant differences between Class III and Class II/1 patients (P = .031; Table 5). Orthodontists rated the improvement among Class III patients higher than the improvement among Class II/1 patients. According to the laypersons, there were no differences in the treatment changes in boys (P >.05), girls (P >.05), or overall patients (P >.05; Table 5).
The Comparison Between Angle Classification and VAS and Test Scores of Both Panels
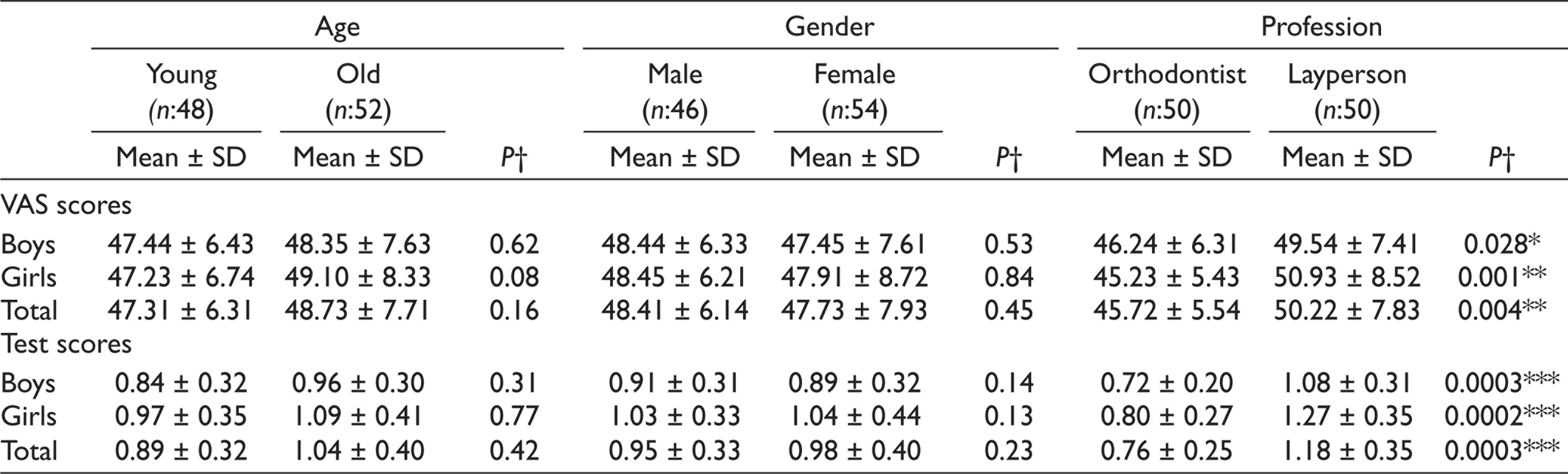
The average scores of the panel members were calculated by taking the average scores of 60 patients and dividing all the members into two groups according to age, gender, and profession. The members whose ages were lower than the median value (42) of all panel members were accepted as being young. When equal and older members were divided into a second group, as elderly, there were no significant differences between the VAS and test scores in terms of patients’ genders and age groups (P >.05; Table 6). However, according to the professions of members, significant differences were observed in the VAS scores of orthodontists and laypersons for girls (P = .001), boys (P = .028), and all patients (P = .004). The laypersons rated the patients as being more attractive than the orthodontists did (Table 6). In terms of the relationship between the members’ professions and the test scores, statistically significant differences were found between the orthodontists and laypersons for girls (P < .001), boys (P < .001), and all patients (P < .001). Also, laypersons assigned higher test scores than orthodontists (Table 6).
The Comparison Between the Age, Gender, Profession of the Panel Members and the VAS and Test Scores of Them
Discussion
Esthetic evaluation of pre and posttreatment has been gaining the attention of patients and their parents. Most patients in orthodontic clinics are adolescents. Therefore, it may be significant to know the esthetic perception of parents in terms of the treatment plan in this age group. However, studies which investigate the effect of orthodontic treatment on facial esthetics in adolescents are limited. Thus, this study aimed to evaluate the perceptions of orthodontists and laypersons about the effects of orthodontic treatment on facial esthetics in Turkish adolescents. The current results showed that orthodontists were more critical than laypersons, who did not notice the treatment changes later for any Angle class. Angle Class III patients also received lower scores from orthodontists and laypersons. In addition, the age and gender of panel members did not affect the perception of facial esthetics.
Previously, the perspectives of laypersons and orthodontists on esthetics have been evaluated by using different scales, including VAS and five-point scale in the literature. Kiekens et al. 16 found that orthodontists were more inclined to assign lower scores compared to laypersons in terms of facial improvement. de Paulo et al. 17 evaluated the esthetic perceptions of facial silhouettes produced by a mandibular protraction appliance in laypersons and orthodontists with VAS. They showed that laypersons identified greater changes between the pre- and posttreatment silhouettes than did the orthodontists. Falkensammer et al. 18 evaluated the perception of facial profile esthetics with a 10-point numerical scale and detected that laypersons gave higher scores than orthodontists. Spyropoulos and Halazonetis 13 also showed that orthodontists scored higher compared to laypersons using a 10-point numerical scale. Tedesco et al. 12 developed a valid and reliable index that provides relatively objective judgments of dental-facial attractiveness and resulted that nonorthodontists were more critical. However, Shelly et al. 14 and Vargo et al. 15 maintained that there was no difference between orthodontists and laypersons in the evaluation of facial esthetics. Similarly, Ackerman et al. 19 did not find any differences between orthodontists and patients’ families in terms of the perspectives of esthetics. In the current study, orthodontists were found more critical than laypersons, because their scores of facial esthetics and treatment changes were lower compared to laypersons.
The VAS which was used in this study has many advantages in esthetic studies. Gould et al. 20 found that VAS is more meaningful because it allows the assessor to assign a point in a continuous interval rather than selecting one of a limited number of categories. Kiekens et al. 10 also found VAS to be a useful method for evaluating facial esthetics, so it was used in this study. In addition, some studies6,13,17 used the VAS for pre- and postoperative photos in the evaluation of treatment changes. According to Kiekens et al., 16 evaluating the effects of treatment using a five-point scale as was chosen in the current study is both easier and more practical. Howells and Shaw 7 argued that although a panel of two persons is acceptable, it would be better to work with larger panel sizes. Kiekens et al. 8 argued that panels consisting of seven laypersons and/or orthodontists would be enough to make reliable measures in clinical and epidemiological studies on adolescent facial esthetics, using the VAS. However, the researchers found that decreasing the panel size makes the results less reliable, while increasing the size increases the costs, in terms of both effort and time. In this study, two separate panels consisting of 50 laypersons and 50 orthodontists were found to be enough for achieving reliable results and saving time, energy, and materials.
Gender7–9,21,22 has been reported to be a factor which may affect the evaluation of perspectives of laypersons and orthodontists. Kiekens et al., 8 evaluated the influence of professional background, age, gender, and geographical region of panel members on their evaluation of the facial esthetics of adolescents and found that males assigned higher esthetic scores to patients than females did. Tole et al. 23 also evaluated the effects of gender, age, and psychosocial context on the perceptions of facial esthetics and determined that women gave lower grades than men. Cochrane et al., 21 O’Neil et al., 22 and Falkensammer et al. 18 examined the effects of gender on esthetic perceptions, and resulted that the genders of the panel members did not affect their perceptions. Maurya et al. 24 evaluated the influence of panel composition on the facial attractiveness of adolescents and there was no significant difference between the ratings of males and females. In this study, it was concluded that gender may not be a factor which influences the perspective of the scorers.
Age6–9 has been also suggested to affect the evaluation of laypersons and orthodontists. Kiekens et al. 8 found that older panel members had more positive evaluations of the boys than younger panel members did, and explained this in terms of the “age factor,” which posits that as people get older they become more accepting regarding facial esthetics. Maurya et al. 24 founded that young laymen rated girls significantly more attractive than old laymen. Tole et al. 23 concluded that the older assessors gave higher grades. This study detected no differences among the orthodontists or laypersons in terms of the effects of the panel members’ ages on esthetic perception and treatment changes. Young age group was chosen for the effects of orthodontic treatment on facial esthetics because the demand for treatment of this age group is higher in our country.
To determine facial esthetics, the position of the sagittal jaw has been analyzed frequently during the determination of facial esthetics. Class I patients have been reported to have the most attractive features;25,26 however, some of the literature has reported the superiority of Class II and Class III patients. Naini et al. 27 evaluated how mandibular prominence influences perceived attractiveness with a seven-point Likert scale by pretreatment orthognathic patients, clinicians, and laypeople. They concluded that Class I profile was more attractive than Class II or Class III profiles and that there were no differences between Class II and Class III profiles. Falkensammer et al. 18 evaluated the influence of education on the perception of patient profiles with a ten-point numerical scale and found that Class I profiles were the most attractive facial profiles according to all groups. They indicated that the Class II profile was more attractive than the Class III profile. In the present study, Class III patients received lower esthetics scores from both laypersons and orthodontists, but there were no differences between the other three groups. In addition, Class I patients were not considered to be the most esthetic group. Mantzikos et al. 28 evaluated esthetic soft tissue profile preferences in the Japanese population and determined that the most preferred profile was the orthognathic profile and the least preferred profile was the mandibular protrusion. Mandibular retrusion was generally preferred over mandibular protrusion. In addition, Suphatheerawatr and Chamnannidiadha 29 modified the facial contour angles and evaluated the influence of the facial profile on perceptions of attractiveness. They found that a normal or slightly convex profile was the most attractive among Asian individuals and the concave profile the least attractive. However, Johnston et al. 9 manipulated silhouette images and found that Class III patients were considered more attractive than Class II patients with the same degrees of malocclusion. In this study, mandibular protrusion was the least attractive one. Thus, it may be concluded that different cultures have different esthetic perception.
This study has some limitations. First, the classification of patients was only in sagittal dimension. Further studies are needed to investigate the perception of orthodontists and laymen in vertical classification of patients. In addition, future studies should investigate the perspective of orthodontists and laypersons on the effects of orthognathic surgery on facial esthetic in patients.
Conclusion
Class III patients received lower scores for esthetics from both panels, but there were no other differences between the other three groups. The changes in facial esthetics after orthodontic treatment was seen more by orthodontists in Class III patients than in Class II/1 patients but was viewed as similar by laypersons.
The ages and genders of the panel members had no influence on the evaluations of facial esthetics and the effects of treatment on facial esthetics. However, the professional background influences evaluation, because orthodontists were found to be more critical than laypersons.
Footnotes
Acknowledgements
The authors would like to thank the patients, laypersons, and orthodontists for their contribution and patience.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This study was conducted by the Declaration of Helsinki and confirmed by the Local Ethics Committee of Selçuk University (#09202005).
Funding
This work was supported by a research grant from Selçuk University, Scientific Research Committee (09202005).
Patient Declaration of Consent
Patients accepted and permitted that their records can be used for any scientific meeting or publication.