
Abstract
Bruxism is a parafunctional teeth grinding activity that is attributed to be of multifactorial origin. The aim of this article is to provide a brief overview on drug-induced bruxism, commonly associated drugs, and its possible pathogenic mechanisms. Around 43 relevant publications were selected after a comprehensive search in PubMed, Cochrane library, Science Direct, and Google Scholar with appropriate keywords to collect data and compile this review. Disturbances in the neurotransmitters and their receptors in the central nervous system may play a significant role, particularly in sleep bruxism. Drugs that interfere normal secretion and function of neurotransmitters are documented to be capable of inducing bruxism. Such psychotropic drugs are being used in clinical practice chiefly for the management of mood disorders, anxiety, and depression. Although bruxism is a well-recognized side effect of certain medications, the extent of awareness about the same is still inadequate among dental professionals.
Introduction
The glossary of prosthodontic terms defines bruxism as “the parafunctional grinding of teeth or an oral habit consisting of involuntary rhythmic or spasmodic nonfunctional gnashing, grinding, or clenching of teeth, in other than chewing movements of the mandible, which may lead to occlusal trauma.” 1 Bruxism is of particular interest to dentists because of its adverse impact on dental hard tissue, restorations, prosthesis, and musculoskeletal structures associated with mastication and speech. The parafunctional teeth-grinding activity that occurs while the person is awake is called “awake bruxism,” and that which happens while the person is asleep is called “sleep bruxism.” Awake bruxism is a semi-voluntary activity that is attributed to life stress. However, sleep bruxism is considered as a sleep-related movement disorder. 2 Systematic reviews performed on the epidemiology of bruxism have shown that bruxism is prevalent among 8% to 31.4% of adults and about 3.5% to 40.6% of children.3,4
Bruxism is believed to be of multifactorial etiology. However, there is a lack of clarity regarding the exact etiology and pathogenesis of this parafunctional habit. Some of the factors which are associated with bruxism include tooth interference, psychological, social and environmental factors, and the functions of basal ganglia and neurotransmitters in the brain. 5 It is proposed that bruxism is mediated through centrally acting mechanisms modulated by the neurotransmitters in the central nervous system. Medications that can interfere with the functioning of these neurotransmitters can induce or suppress bruxism. 6 Literature survey reveals reports of many cases of bruxism occurring as an adverse effect to certain psychotropic drugs. Although drug-induced bruxism is a well-accepted entity in the field of psychiatry, the extent of awareness among dental professionals regarding bruxism as an adverse effect of medications is still under-recognized. Hence, this article aims to provide a brief overview of drug-induced bruxism, the medications reported to be associated with it, and its management. Search strategies used were the electronic databases PubMed [Mesh], Cochrane library, Science Direct, and Google Scholar. The keywords used were “drug induced” and “bruxism.” The article search was done to find all literature until March 2020. Relevant case reports, systematic reviews, and other literature reviews where bruxism was discussed as a consequence of medications were included in the review.
Pathogenesis of Drug-Induced Bruxism
Lifestyle changes including elevated stress levels, lack of proper sleep, and nourishment have increased the prevalence of mood disorders and mental health diseases globally.7–9 Because of the increasing awareness about mental health, the number of people who seek treatment for various mental health issues has also increased. A significant number of such patients are prescribed with drugs for the management of their mental health conditions. There is also an increase in the number of patients seeking treatment for various neurological diseases over the past decades.10,11 Antipsychotics, antidepressants, and many other classes of drugs which act directly or indirectly on the central nervous system are being prescribed to such patients as single agents or in combination.
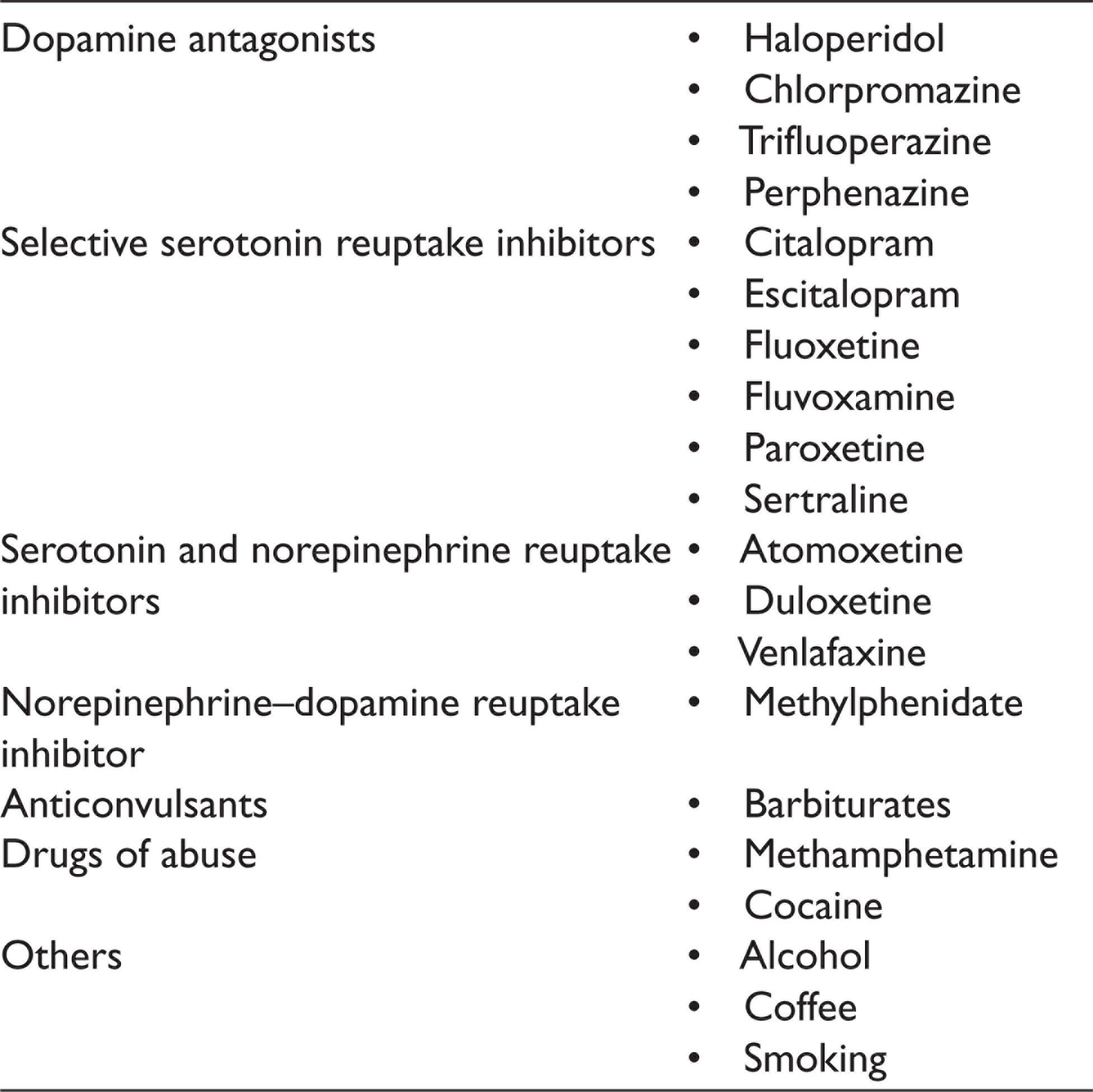
Psychotropic drugs are chemical substances that can cross the blood–brain barrier and primarily act on the central nervous system. This category includes all the drugs that act on various receptors in the central nervous system causing either stimulation or suppression. Thus, they result in alterations in perception, mood, cognition, behaviour, and consciousness. Some of these drugs are known to induce bruxism in patients. The drugs that cause bruxism act mainly through dopamine, serotonin, norepinephrine, and histamine. These medications alter the receptors of various neurotransmitters and modulate their responses. 6 Bruxism is an under-recognized adverse drug reaction associated with some psychotropic medications. 12 The drugs chiefly associated with bruxism are enlisted in Table 1. Although the exact mechanism involved in the development of the condition is poorly understood, several neurotransmitters such as serotonin, norepinephrine, and histamine could modulate the suppression of dopamine activity. This could be the potential cause of sleep bruxism among patients under drugs belonging to these respective groups. 13 Bruxism induced by antidepressants can occur in patients regardless of their age. The symptoms usually begin to manifest within 3 to 4 weeks since the commencement of the medication. 14 However, even a few doses of the offending drug may trigger the development of bruxism. The frequency of symptoms is dose-dependent and it usually resolves within 3 to 4 weeks after the cessation of the drug. 12 The specific pathogenic mechanism specific to each drug group is explained further under their respective headings.
List of Drugs Associated With Bruxism
Dopamine Antagonists and Bruxism
Dopamine antagonists are a group of antipsychotics which are used for the management of schizophrenia, bipolar disorder, and stimulant psychosis. Dopamine antagonists are of two types: typical antipsychotics that act solely on D2 dopaminergic receptors and atypical antipsychotics that act on D2 as well as on serotonin receptors. Bruxism is manifested in some patients under dopamine antagonists, as an extra-pyramidal side effect of the inhibitory action on dopamine. Dopaminergic neurons of the mesocortical tract control masticatory motor activity. Dopamine inhibits spontaneous movement, and it plays a significant role in motor control. Serotonin inhibits dopaminergic transmission in this tract. Thus, the administration of dopamine antagonists and serotonin inhibitors causes bruxism. 6 However, some of the atypical newer generation antipsychotics have weak extra-pyramidal effect. Hence, these drugs are often used as substitutes when extra-pyramidal side effects of typical antipsychotics limit its usage. 15
Haloperidol is a typical dopamine antagonist that causes nocturnal bruxism. 16 In a case report by Amir et al., bruxism induced by haloperidol was relieved by adding propranolol to the regiment. This is suggestive that in addition to dopamine, other additional neurotransmitters may also be involved in the causation of bruxism. The currently available evidence points that interference of striatal dopaminergic balance contributes to bruxism.17,18 Other dopamine antagonists of the category phenothiazines such as chlorpromazine, trifluoperazine, and perphenazine are documented to be involved in inducing bruxism.19,20 Ziprasidone, an atypical antipsychotic, was reported to have caused dystonia, bruxism, and trismus in a patient, which were relieved on reducing the dosage of the drug. 21
Studies have revealed that short-term usage of dopamine precursors has depressive effect on bruxism.1,22 Dopamine precursors are capable of managing the abnormal side imbalance in the receptor expression of striatal D2 and depletion of dopamine in the basal ganglia. Hence, drugs that can enhance the dopamine transmission such as levodopa and bromcriptine have suppressive effect on bruxism. 6
Selective Serotonin Reuptake Inhibitors
Selective serotonin reuptake inhibitors (SSRIs) are yet another group of drugs used for the management of various psychiatric conditions such as depression, anxiety disorders, and obsessive-compulsive disorders. They act by inhibiting the reuptake of serotonin at a presynaptic neuron. SSRIs induce serotonergic effect on mesocortical neurons at the ventral tegumental area. This in turn inhibits dopaminergic action in the tract indirectly. Bruxism is an extra-pyramidal side effect seen among some patients under chronic treatment with SSRIs. 6
In the systematic review by Garret et al., six SSRIs such as citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline were identified as offending agents for bruxism. It was also added that among SSRIs, fluoxetine is the most reported SSRI associated with bruxism, followed by sertraline. The resolution of symptoms was made possible either by adding serotonin 1A partial agonists such as buspirone and tandospirone, by reducing the dosage of the drug, by the cessation of the medicine, or by adding other pharmacological agents. Tricyclic antidepressants such as amitriptyline; other antipsychotics with weak extra-pyramidal side effects such as aripiprazole; chlorpromazine, norepinephrine–dopamine reuptake inhibitors such as bupropion; or serotonin 2A/2C antagonist and reuptake inhibitors such as trazodone could be used as substitutes for drugs that cause bruxism. These symptoms may also resolve over time without any particular intervention.14,23–26
Other Reasons for Bruxism
Serotonin and norepinephrine reuptake inhibitors (SNRIs) are a class of antidepressants that have action on both serotonin and norepinephrine. SNRIs such as atomoxetine, duloxetine, and venlafaxine are also reported to be capable of causing bruxism. Venlafaxine accounts for the most number of SNRI-related bruxism cases reported in the literature till date. Bruxism occurs as an extra-pyramidal side effect of serotonergic action. Buspirone, a partial agonist of serotonin 1A receptors, is found to be effective in treating venlafaxine-induced bruxism. Aripiprazole also functions in the same way to alleviate bruxism.27,28
Methylphenidate is a norepinephrine–dopamine reuptake inhibitor used in the treatment of attention deficit/hyperactivity disorder. A 9-year-old patient developed sleep bruxism five days after she was started on 18 mg/day oral methylphenidate, which completely dissipated during the drug holidays on weekends and reappeared on resuming the medication on weekdays. Clonezepam and buspirone did not resolve the condition. Bruxism completely resolved two days after patient was started on 75 µg clonidine at bedtime. 29
Dopamine is responsible for reward motivated behavior. 6 Addiction-producing pharmacological agents such as nicotine, opioids, alcohol, amphetamine, and cocaine increase dopamine release in accumbens nucleus in the basal ganglia. Other mediators such as glutamate, GABA, and serotonin also influence mesolimbic dopaminergic pathways and may be other reward pathways. 16 A nationwide cohort study done in Finland by Rintakoski et al. concluded that there is increased risk for sleep bruxism with increasing alcohol intake. The same study also concluded that the risk for sleep bruxism is high among those who consume more than eight cups of coffee per day. Smoking was considered as an independent risk factor. 30 A systematic review evaluating the association between sleep bruxism and alcohol, caffeine, tobacco, and drug abuse concluded that the odds for sleep bruxism increased almost two times for those who drink alcohol, almost 1.5 times for those who consumed more than eight cups of coffee per day and more than two times for smokers. 31 Cross-sectional studies conducted among methamphetamine users had identified that bruxism is a frequently prevalent event among them.32–35 Cocaine addicts with frequent intoxication tend to have severe bruxism leading to flat cuspal inclinations in posterior teeth. Chronic addicts tend to also develop temporomandibular joint disorders as a deleterious consequence secondary to long-standing bruxism. 36 Cessation of the habit and rehabilitation of the patient would be the first step toward addressing bruxism and related problems in drug addicts. See et al. have reported a successful management of medically intractable bruxism that developed in an amphetamine abuser one month after the withdrawal of the drug with botulinum toxin. 37
Anticonvulsant medications such as barbiturates were found to be associated with bruxism in patients with cerebral palsy in one study. The authors suggest that increased frequency of sleep bruxism among those administered with barbiturates should be considered as a consequence of dyskinesia induced by these medications. Neurological problems that already exist in children with cerebral palsy make them more prone to extra-pyramidal side effects of the medication. There is not enough evidence however to substantiate this claim. Other group of drugs such as benzodiazepines and valproates are associated with much lower incidence of sleep bruxism in children with cerebral palsy and should be preferred in such cases.13,38
A study among HIV positive patients under antiretroviral therapy suggested that the incidence of tooth wear increases with the increase in the duration of antiretroviral medication. The authors noted that there was increased prevalence of psychiatric disorders among HIV-positive patients included in the study with many subjects reportedly taking psychotropic medications. Hence, the study could not conclusively suggest that there is a direct association between antiretroviral therapy and tooth wear. 39 Future well-controlled studies may shed light on the association between antiretroviral therapy and bruxism.
Assessment of Bruxism
It is necessary to evaluate bruxism clinically as it causes damage to the teeth and perioral structures. The assessment may vary with the etiology of bruxism and the various complications faced by the patient due to bruxism. Various methods are employed for the assessment of bruxism. 40 Noninstrumental approaches include self-report and clinical inspection. Self-report can be prepared through questionnaires and case history. Clinical inspection is useful for evaluating both sleep bruxism and awake bruxism. Instrumental approach for bruxism assessment includes application of electromyography to record the teeth grinding activity during sleep or while the patient is awake. The number of grinding activities per hour of sleep is calculated and recorded. In addition, a few grading systems had also been proposed by different authors for the assessment and follow-up of the condition. 41 There are no standardized guidelines for the evaluation of bruxism. However, recently two closed meetings were conducted with selected invited members by International Association for Dental Research (IADR) with the aim of proposing a multidimensional system termed as “Standardised Tool for the Assessment of Bruxism.” The general structure of the multimodular system comprises of two axes. Axis A deals with the assessment of bruxism/masticatory muscle activity through self-reports, clinical evaluation, and instrumental assessment. On the other hand, axis B deals with the etiology, risk factors, and concurrent conditions associated with bruxism. However, this new diagnostic and decision-making algorithm, which is aimed at facilitating a comprehensive approach to the clinical impact of bruxism, is still under the process of revision and refinement by an expert panel under IADR. 42
Management of Drug-Induced Bruxism
The currently available literature does not suggest any standard protocol for managing drug-induced bruxism, and it is difficult to provide one due to the marked variability in the literature. 43 Based on the current understanding, the authors suggest that once the offending drug is identified, it has to be either stopped, administrated at a lower dose, or replaced with an appropriate substitute. Rajan et al. suggested that while replacing the offending drug with a substitute, an antidepressant belonging to the same class as the offending drug should be prescribed before prescribing a drug from an entirely different class. In case the symptoms are not subsiding, antidotes could be considered including dopamine agonists such as buspirone. 43 We further suggest that the patients under drugs of abuse should be rehabilitated and any damage to the oromuscular structures due to bruxism should be handled accordingly. Further the patients should be followed up regularly to ensure best results.
Conclusion
Over the past few decades, there is progressive increase in the awareness about mental health. Consequently, there is a rise in the number of patients taking medications for various psychiatric conditions. A detailed medical history of the patient helps the dentists to accurately identify and address various oral health problems which also include adverse drug reactions such as bruxism. Although there is literature on drug-induced bruxism, it is still an under-recognized problem in dentistry. The current availability of literature is limited only to a certain group of drugs. It is important that the dentists update themselves on this condition, identify it accurately, alert the specialists, and report it so that in the future such adverse reactions could be minimized or avoided and all patients experience a more comfortable recovery.
Footnotes
Acknowledgements
The authors would like to thank the editors and authors of various journals and articles which was a source for compiling this review article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Declaration of Consent (If In-vivo Study/Case reports)
Consent of patients was taken before commencement of study.