
Abstract
Aim:
The aim of this study was to compare the effectiveness of different filling materials and obturation techniques for root canal obturation in primary teeth.
Materials and Methods:
Eighty maxillary primary incisors were included in this in vitro study. After biomechanical preparation, all samples were scanned using microcomputed tomography (micro-CT) and root canal volumes were calculated. Samples were grouped according to filling materials and obturation techniques, with ten samples in each group. The samples were filled with zinc oxide eugenol (ZOE) and Vitapex using four different obturation techniques (local anesthesia syringe, lentulo spiral, pastinject, and lentulo spiral–ultrasonic activation). After filling, samples were scanned a second time using micro-CT and root canal volumes were calculated. The statistical analysis was performed using SPSS version 24.0. Data were analyzed by Kruskal–Wallis and Mann–Whitney U tests.
Results:
When the ZOE and Vitapex were compared, it was observed that there were no significant differences between their postobturated volumes, percentage obturated volume (POV), internal void (IV), and percentage of internal void volume (PIV) (P > .05). The local anesthesia syringe group had a significantly lower postobturated volume and POV, and a significantly higher IV and PIV for both filling materials than that by the other groups (P < .05). There was no significant difference between the other obturation techniques (P > .05). For the local anesthesia syringe group, postobturated volume and POV were significantly higher and IV and PIV were significantly lower with Vitapex than with ZOE (P < .05). There was no significant difference between the other obturation techniques filled either with ZOE or Vitapex (P > .05).
Conclusion:
Except for the syringe technique, no difference was observed between the ZOE and Vitapex materials. The syringe technique used in the primary root canal filling was less effective than the other techniques, which had similar efficacy, and in this technique, more effective canal filling was achieved with Vitapex.
Introduction
Root canal treatment is one of the preferred treatments for primary teeth that have irreversibly damaged pulps. 1 The purpose of endodontic treatment in primary teeth is to maintain healthy periodontal and periapical tissues until permanent teeth eruption. 2 For successful endodontic treatment, vital tissues, necrotic residues, and microorganisms should be eliminated from the root canal system. The root canals should also be shaped with respect to their original form and should be disinfected and hermetically filled with an appropriate filling material. 3 Several filling materials and obturation techniques have been proposed to increase the clinical success of pulpectomies in primary teeth. Generally, canal filling pastes containing zinc oxide eugenol (ZOE), calcium hydroxide, and iodoform have been recommended, although there is no consensus on an ideal material. 4 Endodontic pressure syringe, lentulo spiral, endodontic plugger, jiffy tube, tuberculin syringe, reamer, insulin syringe, disposable syringe, NaviTip, bidirectional spiral, and pastinject methods are used for obturation in primary teeth. 5 However, it is difficult to provide a hermetic root canal obturation using these methods because of the characteristics of the root canal system of primary teeth. Ultrasonic devices are widely used in various endodontic procedures, ranging from therapeutic and diagnostic applications to endodontic surgery.6,7 Ultrasonic activation of the filling pastes facilitates their deeper penetration into the lateral and accessory canals while enhancing impermeability and antimicrobial activity. 8 However, only a few studies have evaluated the effect of ultrasonic activation on the quality of primary teeth root canal obturation.
Several studies have evaluated the effectiveness of canal filling materials and obturation techniques in primary teeth, but they have predominantly used digital radiography or conventional tomography.9–12 Both these imaging modalities have low spatial resolutions (100–1000 μm). Additionally, digital radiographs permit only two-dimensional (2-D) evaluations. 13 Microcomputed tomography (micro-CT) has high-resolution and enables quantitative evaluation of internal anatomical changes in the root canal. 14 Several studies have evaluated the root canal obturation quality of permanent teeth using micro-CT15,16; however, only one study has evaluated the quality of primary teeth obturation using micro-CT. 13
The aim of this study was to compare the effectiveness of different filling materials and obturation techniques for root canal obturation in primary teeth using micro-CT. The null hypothesis is that there is no difference between the four obturation techniques and two filling materials in the root canal filling quality of primary teeth.
Materials and Methods
Setting and Design
This in vitro study was conducted in the Department of Pediatric Dentistry of Faculty of Dentistry at Erciyes University, Kayseri, Turkey. This study was conducted between April 2018 and January 2019. Eighty maxillary primary incisors were selected with the following inclusion criteria: (a) absence of root anomalies, (b) root resorption level not exceeding one-third of the root length, (c) radiographically confirmed absence of calcification, (d) absence of fracture or crack in the root canals, (e) absence of internal or external root resorption, and (f) root length of at least 10 mm. In the study, teeth with severely crown damage due to trauma and/or caries, with lesion at the root apex and with extraction indication, were used. With 1.5 effect value, alpha = 0.05 error, and power 95%, it was determined that there should be ten samples in each group.
17
The distribution of samples to groups was made by the simple random sampling method using a free internet-based randomization software (
Study Methods
The crown of the teeth was split from enamel–cement junction by a water-cooled diamond separe (Meisinger USA, Centennial, CO, USA), and access cavities were prepared using a diamond round bur (Mani, Utsunomiya, Japan). Using a 10# K-type file (Dentsply®, Maillefer, Ballaigues, Switzerland), the working length of each sample was determined to be 1 mm shorter than the anatomical apex. Canal preparations were completed using a WaveOne Gold (green, size 35-taper 0.06, Dentsply®, Maillefer) file. Root canals were irrigated with 1% sodium hypochlorite (2 mL) and sterile saline solution (2 mL) during the biomechanical preparation. Finally, all canals were dried with paper points (size 35) (DentPlus, DiaDent, Cheongju-si, South Korea).
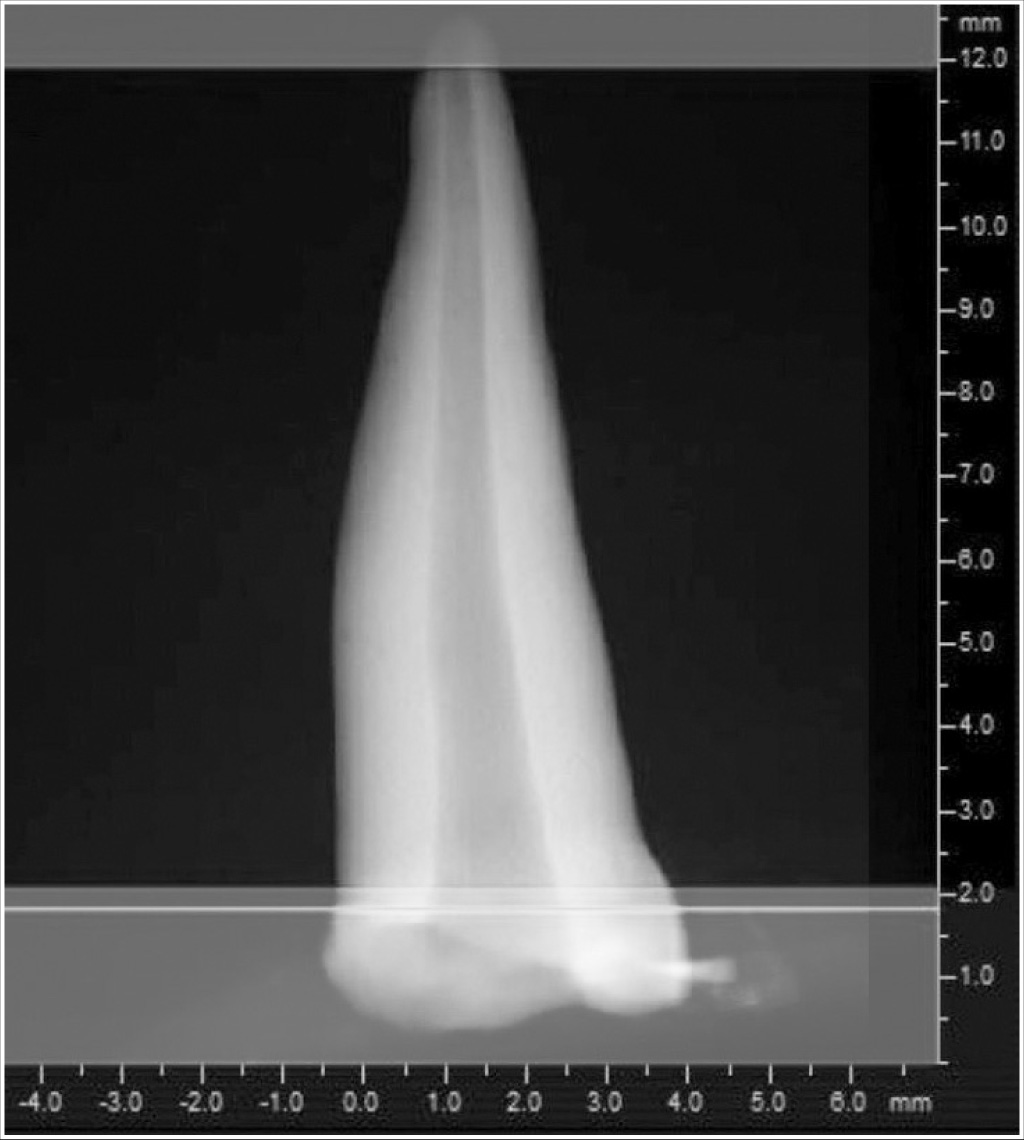
After the biomechanical preparation, all prepared samples were scanned with a micro-CT (SkyScan 1272; Bruker MicroCT, Kontich, Belgium) in the Scientific Research Laboratory of the Faculty of Dentistry in Erciyes University for 20 min using the following scan settings: section thickness 14.0 μm, reconstructor turning angle 180°, turning angle 0.5°, isotropic resolution setting 14.0 μm, frame mean on (2), and random motion off. The radiograph tube was operated at 80 kV and 125 μA using a 0.5 mm aluminum filter. From each sample, 1023 cross-sectional images with axial section thicknesses of 14.0 μm were obtained. Contrast and sharpness adjustments were made on the obtained section images. Data (sectional images) were reconstructed using CTAn software (version 1.6.6, Bruker Skyscan, Kontich, Belgium) and transformed into three-dimensional (3D) images. The preobturated canal volume (X) was calculated and recorded for each sample using the data obtained (Figure 1).
Micro-CT scan view of the primary tooth after root canal preparation and before root canal obturation
After the first micro-CT scan, the 80 samples were randomly divided into the following two groups based on the canal filling material, with 40 samples in each group: ZOE (Cavex, Haarlem, Netherlands) and Vitapex (Neo Dental, Cumnock, UK). Each filling material group was randomly divided into four subgroups based on the obturation techniques: local anesthetic syringe (n = 10), lentulo spiral (n = 10), pastinject (n = 10), and lentulo spiral–ultrasonic activation (n = 10). ZOE was prepared in line with the manufacturer’s recommendations. Vitapex was transferred from its own syringe to a sterile glass before use.
Local Anesthetic Syringe
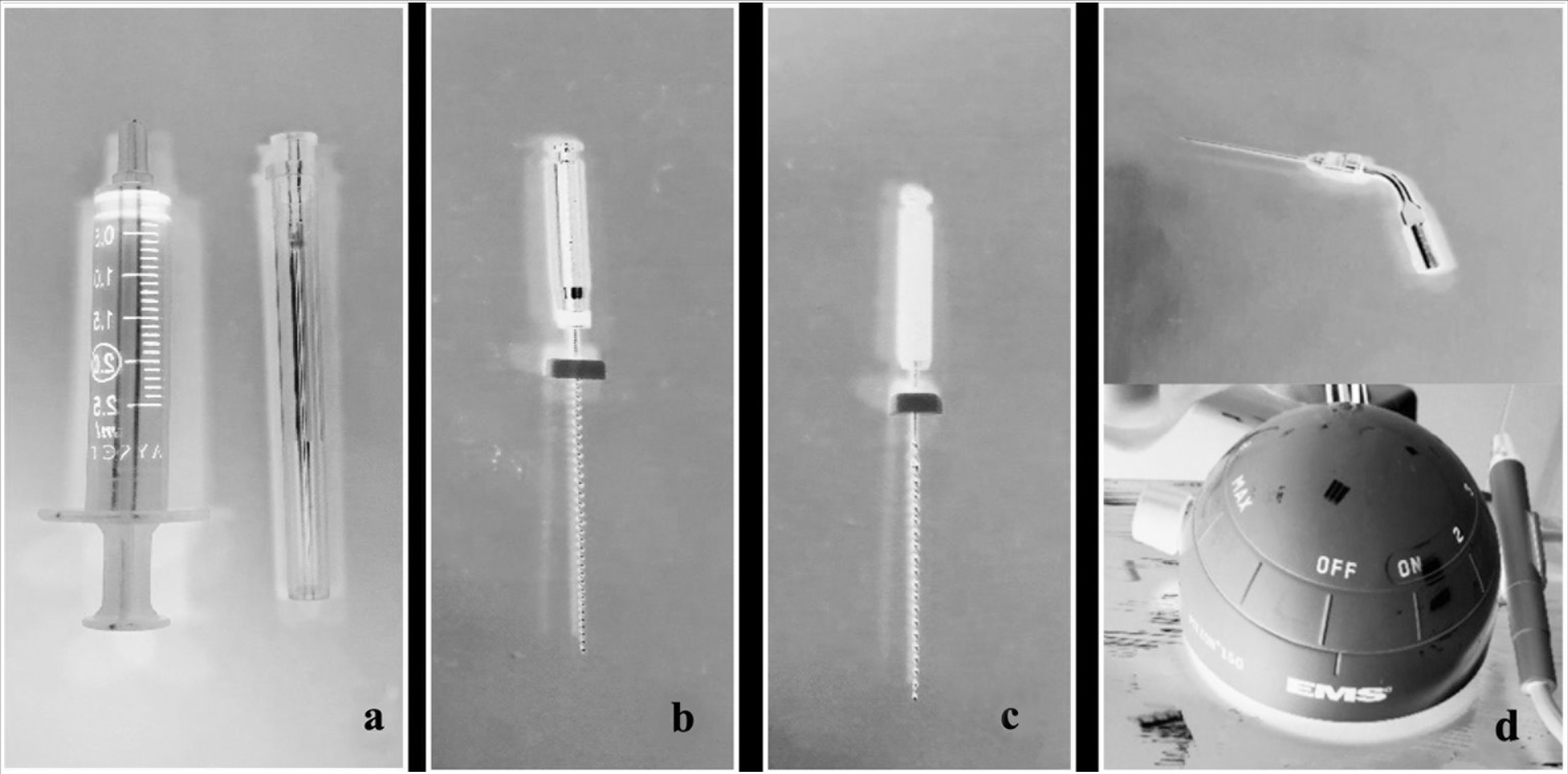
In this group, a 2 mL 27-gauge disposable local anesthetic syringe (Ayset, Adana, Turkey) was used to fill the canals (Figure 2A). A rubber stopper, adjusted to 2 mm shorter than the biomechanical preparation length, was placed on the needle to determine the working length. The syringe was filled with filling materials, and the needle was advanced into the canal to the length marked by the rubber stopper. The paste was injected by finger pressure until it was seen at the opening of the canal. The needle was slowly withdrawn while the paste filled the canal.
Lentulo Spiral
In this group, a green band lentulo spiral (length: 25 mm, Dentsply, Maillefer) was used to fill the canals (Figure 2B). A rubber stopper, adjusted to 1 mm shorter than the biomechanical preparation length, was placed on the lentulo spiral to determine the working length. The lentulo spiral was dipped in ZOE or Vitapex, advanced into the canal, turned clockwise, and withdrawn from the canal while turning. The lentulo spiral was changed after being used twice.
Pastinject
In this group, pastinject (length: 21 mm, Micro-Mega, France) was used to fill the canals (Figure 2C). A rubber stopper, adjusted to be 1 mm shorter than the biomechanical preparation length, was placed on the pastinject to mark the working length. The pastinject was dipped in ZOE or Vitapex, advanced into the canal, turned clockwise, and withdrawn from the canal while turning. Pastinject was changed after being used twice.
Lentulo Spiral With Ultrasonic Activation
In this group, the canals were initially filled using the lentulo spiral technique. Subsequently, ultrasonic activation was applied for 2 s at the fourth power level without touching the root canal walls, using an ultrasonic file (size 15, taper 0.02; ESI Instrument, EMS, Nyon, Switzerland; Figure 2D), which was positioned 1 mm shorter than the biomechanical preparation length.
Instruments used in root canal filling procedure. (a) Local anesthetic syringe. (b) Lentulo. (c) Pastinject. (d) Ultrasonic activation device and tip
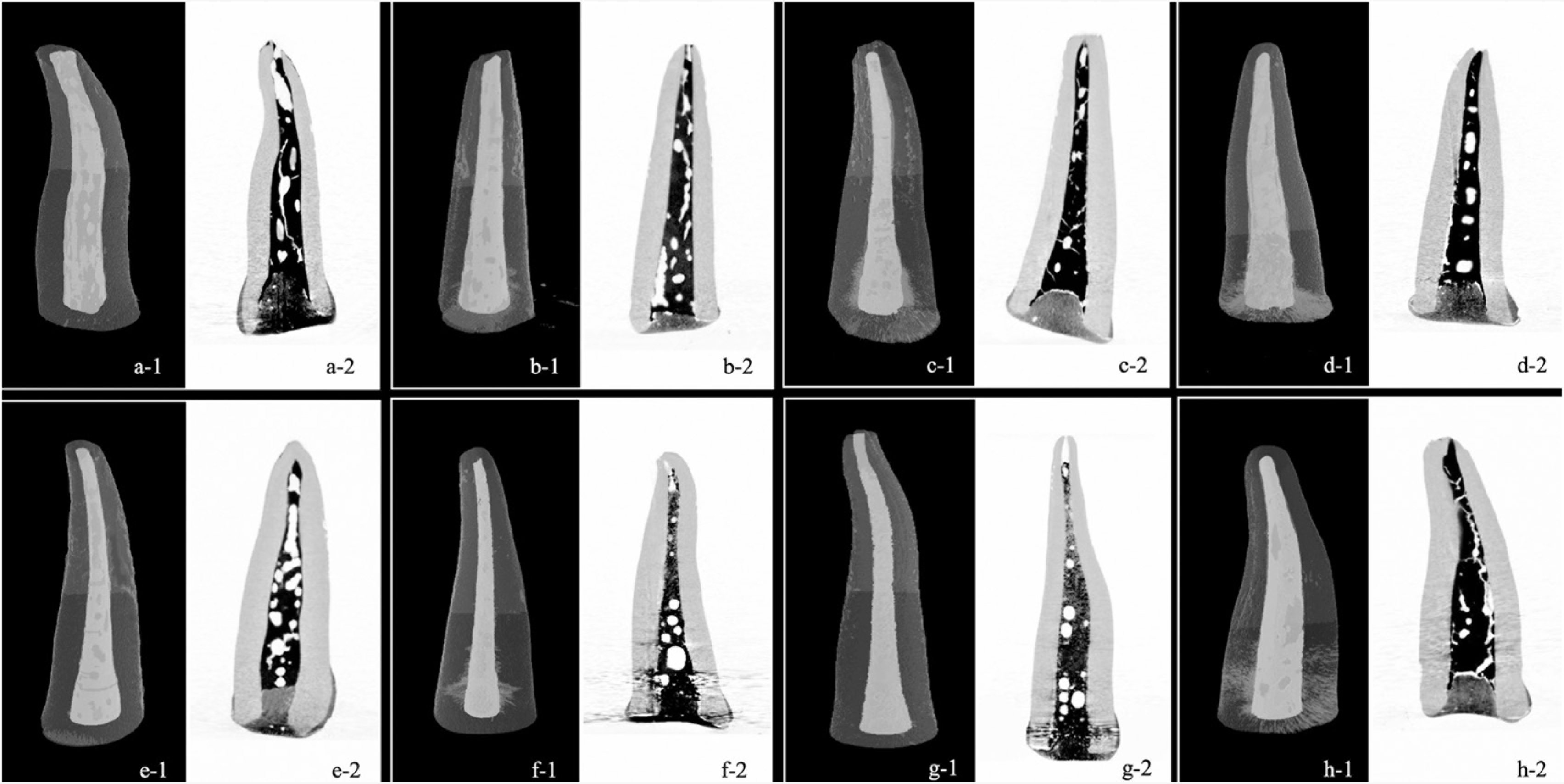
All obturation procedures were carried out by only one operator. After obturation, each sample was sealed with glass ionomer cement and its root surface was covered with nail polish. To complete the hardening of the filling materials, samples were placed in a sterile saline solution and kept in an incubator (NUVE Incubators, Ankara, Turkey) at 37°C for 48 h. Then, a second micro-CT scan was performed to determine the volume of the filling paste inside the canal (Y). The parameter settings for the second micro-CT scan were the same as that for the first. Images obtained for each sample from the second micro-CT scan were reconstructed with CTAn software and transformed into 3D images. Using data from these scans, the postobturated root canal volume for each filling material in each sample (Y) was calculated (Figure 3). For each canal, the percentage obturated volume (POV) was calculated using the following formula:
Micro-CT scan view and 3D views for each group. (a) 1,2: Eugenol and syringe group. (b) 1,2: Eugenol and lentulo group. (c) 1,2: Eugenol and pastinject group. (d) 1,2: Eugenol and lentulo + ultrasonic activation group. (e) 1,2: Vitapex and syringe group. (f) 1,2: Vitapex and lentulo group. (g) 1,2: Vitapex and pastinject group. (h) 1,2: Vitapex and lentulo + ultrasonic activation group. 1: 3D view of root canal filling; 2: Cross-sectional view of root canal in vertical plane
POV = Postobturated root canal volume (Y)/Preobturated root canal volume (X) × 100 = (Y/X) × 100.
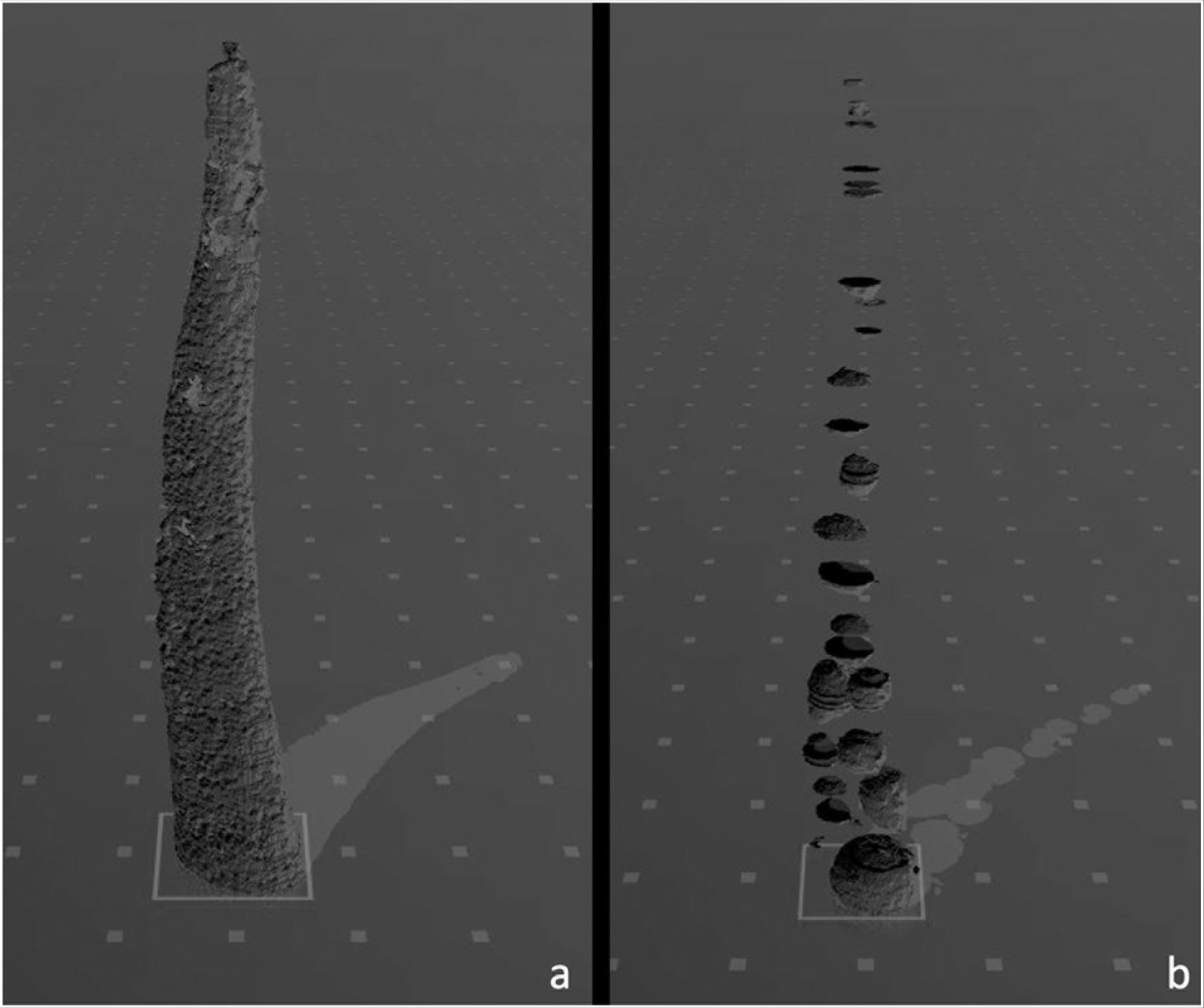
An extraction technique was used to calculate the internal void (IV) volume. First, all the voids detected in the filling material and between the filling materials and root canal walls were filled. The original canal filling volume was removed from this image. The voids of each sample were measured in mm3 with CTAn software and calculations of IV volume were made (Figure 4). The percentage of internal void volume (PIV) was calculated using the following formula:
(a) Volumetric 3D view of the filling material in the obturated root canal. (b) Volumetric 3D view of the internal voids that remained in the root canal after obturation.
PIV = IV volume/Filling material volume ×100.
Root canal volumes (pre- and postobturated volumes, POV, IV, and PIV) were calculated by another operator who did not know what material and technique was used for the obturation.
Statistical Analysis
Statistical analysis was performed using SPSS statistics software (IBM SPSS statistics, version 24.0, IBM Corp., Armonk, NY, USA). Descriptive statistics of the variables are expressed as mean ± standard deviation. The normality test of the variables was performed using the Shapiro–Wilk test. Comparison of the variables of the groups was performed using the Kruskal–Wallis test because nonparametric test conditions were met. Paired comparisons between the groups were performed using the Mann–Whitney U test. For all tests, P value of < .05 was considered statistically significant. To evaluate the reliability of the measurements in the study, the second measurement of 20 randomly selected teeth was performed by the same researcher one month after the first measurement. Intraclass correlation coefficient (ICC) was used to evaluate the two measurements. Accordingly, the ICC coefficient was determined to be between 0.718 and 0.833.
Results
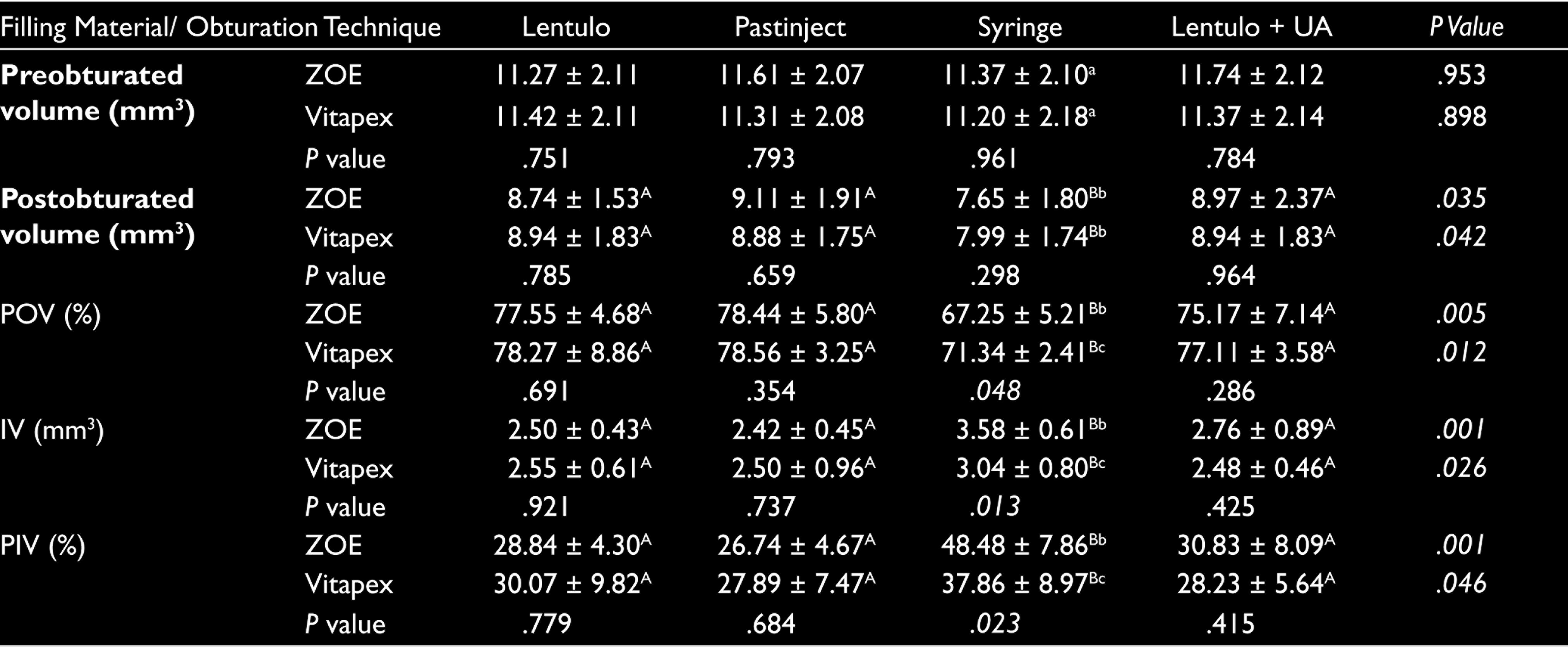
Preobturated volume, postobturated volume, POV, IV, and PIV values according to filling materials and obturation techniques are presented in Tables 1 and 2. When ZOE and Vitapex were compared, there was no difference between the preobturated and postobturated volumes, POV, IV, and PIV (Table 1). A comparison of the obturation techniques revealed a statistically significant difference between the postobturated volumes, POV, IV, and PIV (Table 2, P < .05). Compared to other obturation techniques, the postobturated volume and POV values were significantly lower, and the IV and PIV values were significantly higher in the local anesthesia syringe group (Table 2). The pre- and postobturated volumes, POV, IV, and PIV values of filling materials stratified by the obturation techniques are shown in Table 3. Preobturated volume did not differ significantly between the groups (Table 3). According to the obturation techniques and filling materials used, a significant difference was observed in the postobturated volumes, POV, IV, and PIV values (Table 3, P < .05). For both filling materials, the local anesthesia syringe technique had a significantly lower postobturated volume and POV and a significantly higher IV and PIV than the other techniques (P < .05). There was no significant difference between the lentulo spiral, pastinject, and lentulo spiral–ultrasonic activation techniques. In the local anesthesia syringe technique, Vitapex showed a significantly higher POV and lower IV and PIV values compared with ZOE (Table 3, P < .05).
Pre- and Postobturation Volume of Root Canals (mm3), Percentage of Obturated Volume (POV), Internal Voids Volume (IV), and Percentage of Voids Volume (PIV) for Each Filling Material Group

Pre- and Postobturation Volume of Root Canals (mm3), Percentage of Obturated Volume (POV), Internal Voids Volume (IV), and Percentage of Voids Volume (PIV) for Each Obturation Technique Group

Pre- and Postobturation Volume of Root Canals (mm3), Percentage of Obturated Volume (POV), Internal Voids Volume (IV), and Percentage of Internal Voids Volume (PIV) for Each Obturation Technique Group According to Filling Material
Discussion
This study compared the effects of two different filling materials and four different obturation techniques used in primary teeth based on root canal filling quality. The samples were prepared using a specific biomechanical preparation technique, and the quality of obturation was evaluated by 3D imaging using micro-CT.
ZOE is a is widely used canal filling material in clinical applications and studies that evaluate different filling materials or obturation techniques.11,12,17–20 However, ZOE has some disadvantages, such as poor resorption when it overflows into the apical region, irritation of the periapical area and permanent teeth germ, and limited antibacterial activity in the canals. 21 To eliminate these disadvantages, canal filling materials containing calcium hydroxide or iodoform have been manufactured for primary teeth. 22 Filling materials containing iodoform are rapidly resorbed when they overflow into the periapical area and do not cause a foreign body reaction. Iodoform does not have undesirable side effects on permanent tooth germ and has strong antiseptic properties.23,24 Based on this, ZOE and Vitapex materials were used in this study.
The disposable injection technique is a practical and economical method used in primary teeth canal obturation. The local anesthesia syringe technique provides successful canal obturation in primary teeth.25,26 Similarly, the lentulo spiral is an effective and economical obturation technique widely used in primary teeth root canal treatments. The design and flexible structure of the lentulo spiral are advantageous for advancing materials into the narrow and curved root canals in both the primary and permanent teeth.20,27 Similar to the lentulo spiral, pastinject is a device specially designed for transferring material into the canal. Several studies have evaluated pastinject for the transfer of intracanal medicaments, such as calcium hydroxide, in permanent teeth. However, only a few studies have evaluated pastinject as an obturation technique for primary teeth.28,29 Apart from these techniques, ultrasonic activation is applied to canal filling materials (pastes), especially in permanent teeth, to adapt them to the root canals. The treatments performed by applying ultrasonic activation to filling pastes have shown an increase in paste penetration into the lateral and accessory canals.8,30 While there are a few studies evaluating the effect of ultrasonic activation of the filling paste in permanent teeth on the quality of the canal filling, no evaluation has been found on primary teeth.8,28,30 Therefore, in this study, we evaluated the use of pastinject and ultrasonic activation in obturation, which has not been sufficiently studied in primary teeth.
Radioisotope, dye penetration, fluid filtration, bacterial leakage, microscopic analysis techniques, scanning electron microscopy, and radiographical methods are generally used to evaluate the quality of root canal obturation. 31 With these imaging methods, 3D images of the samples cannot be obtained, and their cross-sections have to be taken for examination. This may result in material loss, and a detailed examination is not possible because of the limited number of sections. 32 3D imaging has been obtained by spiral computed tomography (CT)17,20,33 or cone-beam CT (CBCT)11,12,18 in different studies, but low-resolution images were acquired compared with micro-CT. 13 Micro-CT provides detailed 3D images of samples without the need for an invasive procedure. 34 Using micro-CT, root canal volumes can be calculated, and quantitative analysis can be performed by creating a 3D image of the distribution and continuity of the voids in the canal after root canal filling.35,36 Despite these advantages, only one study, to the best of authors’ knowledge, has examined the quality of root canal filling in primary teeth using micro-CT. 13
Previous studies that have compared canal filling materials in primary teeth have varied in focus. Babashahi et al. evaluated obturation quality using spiral CT and found no significant difference between the POV values of the root canals that were filled with ZOE and Metapex. 37 According to Aragão et al., root canals filled with ZOE and Vitapex did not have significant differences in POV, PIV, and the number of IVs. 13 In this study, similar POV, PIV, and IV values were obtained for the canals filled with ZOE and Vitapex (Table 1). However, a significant difference between ZOE and Vitapex was observed in the local anesthesia syringe group; significantly higher POV and lower IV and PIV values were obtained with Vitapex compared to ZOE (Table 3). Asokan et al. reported that a more effective canal filling is provided with Vitapex and Metapex than ZOE, which is consistent with our findings. 20 However, ZOE was administered using a lentulo spiral, whereas Vitapex and Metapex were administered with special syringes in this study. The significant difference was attributed to the lack of standardization across obturation techniques.
Some studies have evaluated the obturation quality using the radiography method. In two different studies conducted by Deveaux and Öztan, the obturation efficiencies of lentulo spiral and pastinject techniques were investigated, and the outcomes were consistent with our study; there was no significant difference between the two techniques.28,29 Grover et al. reported that the pastinject technique provided a significantly more effective canal filling than the lentulo spiral technique, and this difference was because of the specially designed flat blade structure of the pastinject. 38 Similarly, Gandhi et al. compared the lentulo spiral, pastinject, and disposable injection techniques and observed that the pastinject technique produced optimal obturation and least voids. 27 In this study, the disposable injection technique produced the highest number of overfilled canals, whereas the lentulo spiral technique produced the highest number of underfilled canals. In all of these studies, canal filling quality was evaluated two dimensionally using radiography. In this study, there was no significant difference between pastinject and lentulo spiral techniques, and we postulated that this was because of the 3D and detailed evaluation of the obturation quality with micro-CT.
Memarpour et al. compared the lentulo spiral and local anesthesia syringe using the radiography method, and they showed that more effective canal filling was achieved with the lentulo spiral. 19 Nagaveni et al., in two different studies using spiral CT and CBCT, reported that more effective canal filling was obtained with a lentulo spiral than a local anesthesia syringe.17,39 Similarly, in this study, while there was no difference between the lentulo spiral, pastinject, and lentulo spiral–ultrasonic activation groups, in the local anesthesia syringe, statistically lower POV and higher PIV and IV values were obtained compared to the other three techniques. In the study by Aragão et al., there were no significant differences between the obturated and IV volumes of the lentulo spiral and local anesthesia syringe groups. 13 Furthermore, the number of IVs was less than that for the syringe technique. This difference is attributable to the use of pressure or material-specific syringes in their study.
Özer et al. radiographically evaluated the effect of ultrasonic activation on the quality of obturation in primary teeth and reported that the application of ultrasonic activation did not improve the root canal obturation efficiency. 40 In this study, the effect of ultrasonic activation on canal obturation in primary teeth was evaluated using micro-CT; it was not expected that ultrasonic activation would decrease canal filling efficacy, although it was not statistically significant. Primary teeth have a thinner root canal morphology compared to permanent teeth. Hence, owing to the primary teeth morphology, ultrasonic activation may not have enough root canal volume that can have a statistically significant effect. Therefore, in this study, ultrasonic activation did not increase the root canal obturation efficiency in primary teeth.
Depending on several factors, including root canal anatomy, quality of canal preparation, clinician’s expertise, and obturation technique used, voids may occur in the canal after obturation. 16 In this study, the biomechanical preparation was performed by a single person using a single technique to ensure repeatable and consistent results. However, the type, viscosity, and density of the filling materials can affect the number and size of voids that form in the canal,13,27 and this may explain the differences between the filling materials observed in this study. Microleakage owning to voids that may remain in the canal after obturation may facilitate the reproduction of microorganisms, cause recurrent infection, and increase the risk of disease after treatment. Studies on filling materials and obturation techniques may facilitate their optimal selection in clinical scenarios. This study was in vitro and conducted on primary incisor teeth. Further in vitro and in vivo studies with larger samples, including primary incisors and molars, are recommended to reveal differences between filling materials and obturation techniques.
Conclusion
The lentulo spiral, pastinject, and lentulo spiral–ultrasonic activation methods had similar efficacy in root canal filling; however, they were more effective than the local anesthesia syringe. Additionally, ultrasonic activation did not positively affect canal filling quality in primary teeth. Finally, more effective root canal filling was achieved with Vitapex compared to ZOE, using the local anesthesia syringe obturation technique.
Footnotes
Acknowledgements
We would like to thank the Erciyes University Scientific Research Unit for financial support (Project ID: TDH-2018-8490) for conducting this thesis project study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Financial support was received from Erciyes University Scientific Research Unit (Project ID: TDH-2018-8490) for this postgraduate thesis project.
Ethical Approval
The approval required for this study, conducted in accordance with the ethical standards recommended by the Helsinki Declaration (1964), was obtained from the Erciyes University Clinical Research Ethics Committee (Approval No: 2018/150).