
Abstract
Aim:
To compare new design implant-supported removable partial dentures retained with anterior fixed prosthesis with a conventional locater and bar attached implant overdenture prostheses retained by two or four implants via photoelastic stress analysis.
Materials and Methods:
Seven edentulous mandibuler acryclic models prepared and divided into two main groups; two to four implant models, subgroup separation as stated; for two implant models overdenture with locator attachment, crown design retained removable prosthesis with clasp retention, bridge design retained removable prosthesis with clasp retention, bridge design retained removable prosthesis with precision attachment retention; and for four implant models prosthesis with bar attachment overdenture, fixed bridge design retained removable prosthesis with clasp retention, fixed retained removable prosthesis with precision attachment retention. A 300 N load was applied to the first premolars. Photoelastic stress analysis method that is a specific method concerning stress visualization, and does not require statistical analysis, was used. The stress distributions were seen in optically using a poloriscope.
Results:
In the models with two implant-retained removable partial dentures, the stress distribution was found to be lower than that with the four implant-retained removable partial dentures. Nonsplinted implants caused high stress around the distal implant on the loading side.
Conclusion:
The stress loads were transmitted to other implants by splinting. Implant-supported removable partial dentures with an anterior fixed prosthetic design show lower stress distributions compared with bar retained prosthesis. These dentures appear to be advantageous in terms of stress transmission.
Keywords
Introduction
The use of a minimal number of implants, easier surgical procedures, and simpler prosthetic designs with prefabricated attachments are the most commonly known advantages of mandibular implant-retained overdentures.1,2 The number and location of implants are important factors for stress distribution around implants and the supporting bone.3,4 Besides, the type of the attachment is also an important factor for implant-supported overdentures (IO). Unsplinted attachment as a locater or splinted attachment as a bar can be used for IO according to retention necessity. 3 In addition to retention capacity, stress transmission between the residual ridges of the implants, implant angulation, and patient satisfaction with both esthetic and functional properties are very important for choosing the correct attachment type and prosthetic design. 2 Previous studies focused on the selection of the type of attachment system. It is important to consider that the system must allow for optimum stress distribution around the implants, provide the most equal load transmission (both for soft tissue and the implant complex), and protect the bone from stress within physiological limits. This way, undesirable stress and complications are avoided and bones may be preserved.5,6
In recent years, a new alternative treatment protocol without complex surgical or grafting procedures has become popular in clinical dentistry. This new protocol is implant-supported fixed prosthesis into the interforaminal region with bilateral movable partial dentures. 7 This concept can provide a fixed restoration in the esthetic region which is not necessary to remove at night, has minimal or smaller removable prosthesis components, and easily compensates implant angulation. For the edentulous mandible, as well as IO prosthesis and fixed implant-supported prosthesis, an implant-supported fixed prosthesis with two or four implants in the anterior region combined with removable partial dentures may comprise a new alternative treatment protocol. 8 There are many clinical reports of this new treatment method in the literature,7–11 but there is no comparison or evaluation of the stress distribution.
Photoelastic stress analysis is a specific method concerning stress visualization, the distribution characteristics of the isochromatic fringe of strain and stress can be favorably seen in optical materials by photoelastic, and then the strain and stress fields can be also quantitatively analyzed, this technique is an observation method. The force details of the materials can be determined based on the photoelastic response of the materials as viewed in polarized light field while recording useful additional information in the normal light field. Recently, the photoelastic experimental method has been widely used into the geotechnical mechanical experimentations like biomechanical dentistry.12,13
The aim of this in vitro study was to compare this new anterior implant-supported fixed prosthesis combination with removable partial dentures, with a conventional locater and bar attached implant overdenture prosthesis on two and four implant-supported photoelastic edentulous models, to evaluate the ideal attachment type for this new design prosthesis and to examine the stress transmission of this increasingly popular treatment protocol on peri-implant areas. The null hypothesis was that there is no significant difference in stress transmission between different prosthetic designs.
Materials and Methods
This study was performed in Selcuk University, Faculty of Dentistry Research Laboratory. For the two implant edentulous model, four different types of prosthesis—overdenture with locator attachment, crown design retained removable prosthesis with clasp retention, bridge design retained removable prosthesis with clasp retention, bridge design retained removable prosthesis with precision attachment retention—and for the four implant edentulous model, three different types of prosthesis prosthesis with bar attachment overdenture, fixed bridge design retained removable prosthesis with clasp retention, fixed retained removable prosthesis with precision attachment retention were compared for stress distribution in a photoelastic stress analysis.
Preparation of Acrylic and Photoelastic Models
Six heat polymerized acrylic resin models (Kulzer Dental) were prepared to model an edentulous patient’s mandible (200 mm × 100 mm × 30 mm). Cylindrical implants (4.1 × 12 mm tissue level, Straumann, Institut Straumann AG) were embedded in the parasymphyseal area of each wax model by a parallelometer (Orthofex, Fogászat Gyártơ KFT). The implants were placed parallel to each other and the midline. For the two implant models, the distance between the implants were set to 22 mm, and the implants were located in the lateral-canine region. 4 For the four implant models, the distance was set to 11 mm. The acrylic models with implants were duplicated with a C-type silicone impression material by the putty-wash technique (Zetaplus, Zhermack). Silicone molds were cured for one week at 25 °C to eliminate the tensions that can occur in photoelastic models depending on the shrinkage of the silicone. The curing was performed to avoid the inaccurate and redundant fringes arising from polymerization shrinkage. The models were tested for residual stresses after setting and after the curing period of one week. The photoelastic resin (PL-2; 35 g) and the catalyzer (PLH-2; 35 g; Measurements Group Inc.) were used. Manufacturer recommended formula was used to calculate the ratio of resin.
Both resin and silicone molds were placed into an incubator for 1 h and heated to 46–52 °C. This heating process provided the lower viscosity and produced a more homogeneous mixture. After incubation, the catalyzer and resin were mixed with a glass pipette avoiding excessive movements and bubbles. The mixing resin filled the entire silicone molds. Mixtures in the silicone molds were polymerized at 25 °C for 24 h. Following this, all resin models were prepared and polished, and the prosthetic laboratory processes were started. For all prosthetic designs, silicone molds were used for standardization of settings for all steps like wax modelation, porcelain application, and artificial teeth settings. For light transmission, transparent acrylic resin (Akribel Hot Acryl, Atlas Enta Dental) was used according to the manufacturer’s recommendations 14 for all types of prosthesis. For gingival stimulation, the posterior areas of the prosthesis were removed at 3 mm thickness using a drill that marked 3 mm in advance to guide the removal. After removal of the prosthesis, the areas were filled with an artificial gingival mask (Zhermack Gingifast Elastic) and placed on the photoelastic models, and the outflows were removed for all types of prosthesis.
Preparation of the Implant-Supported Removable Partial Dentures
For the fixed components of implant-supported removable partial dentures (IRPD), 5.5 mm solid abutments were placed into the two and four implant models and torqued with 35 Ncm. For the laboratory stages, laboratory models were duplicated from the photoelastic models with vinylpolysiloxane impression material (Virtual, Ivoclar Vivadent). First, two and four implant-supported bridge design restorations were modeled, and then a silicone index was used to standardize the bridge precision attachment and crown design models. An extracoronal resilient precision attachment was used (Probolte Attachments, Kargı Dental). With small dimensions (2.0 mm height and 4.2 mm length), these attachments are used particularly in anterior regions with two abutment teeth. Good retention, lack of milling requirements, and simplicity of use are the most important properties of this system. 8 The casting procedures were performed according to the manufacturers’ recommendations with a Ni-Cr alloy (61% Ni, 25.60% Cr, 10.94% Mo, 1.51% SI, 0.01% Mn, and 0.01% C).
After the laying procedure, metals were sandblasted with 25–70 µm Al2O3 particles (Star Dental) and ultrasonically cleaned for 15 min before porcelain application. Porcelain (Shofu Vintage Halo, Shofu Inc., PN 6507) was applied and then checked on the master models.
For the removable prosthesis with clasps, I bar clasps were planned. All models were cast with a Cr-Co alloy; 64% Co, 28.5% Cr, 8% Fe, and 3% Mo (Wironium Plus, Bego, PN 50190). After the artificial teeth were set for all models. After checking the setting on the master models, the finishing procedures were made with standard methods. Laying and polishing procedures were then conducted.
Preparation of the Implant-Supported Overdentures
Initially, for the four IO models, SynOcta abutments (Straumann, Institut Straumann AG) and gold copings were screwed on. Bar attachments were cut according to the distance between the copings and blocked out with utility wax in order to set them 5 mm away from the tissue (3 mm gingival height, 2 mm distance from the tissue). The prepared bars were adjusted by millimeters, a pattern resin was used for splitting the bars, and the gold copings were unscrewed for the soldering procedures.
For the two implant models, locater abutments were fitted and torqued with a 35 N/cm force, and an acrylic base plaque was prepared and fixed to the locater matrix. After the positioning of the attachments, models were duplicated for the laboratory procedures. Artificial teeth settings were made according to the silicone indexes. All finishing procedures were completed according to the standard methods on the duplicate models. After the laying and polishing procedures, the prostheses were checked on the master models. A blue-colored retentive rubber with a retention force of 1.5 lbs = 66.7 N was used.
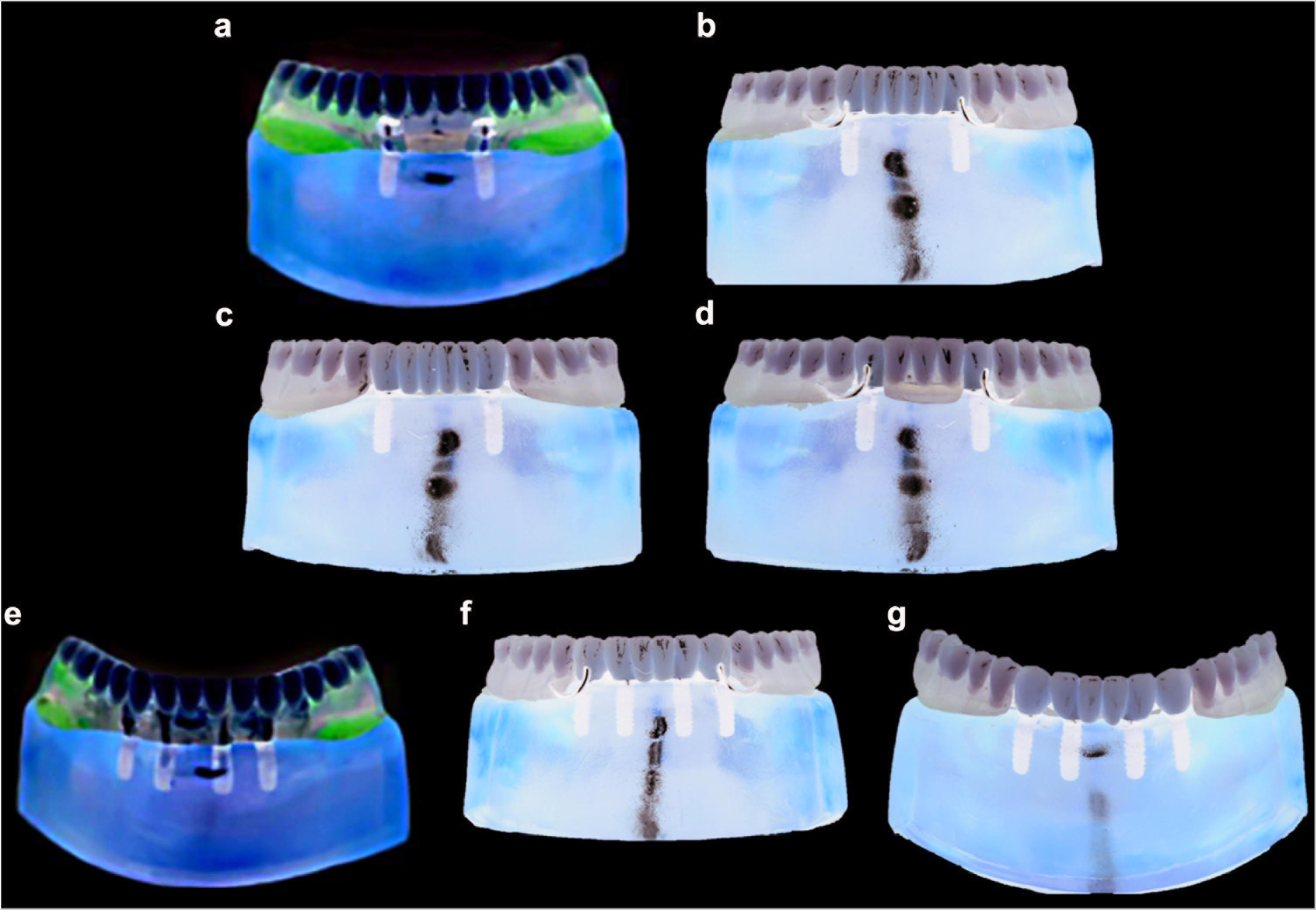
A 300 N vertical load was applied bilaterally to the central fossa of the first premolar occlusal surface by a universal test machine (TSTM 02500, Elista Ltd.). The models (Figure 1) were placed a special clamp-like device for stabilization so that there was no movement when the load was applied. During installation, the resulting stresses -were seen as the stress lines (Fringes) - were observed and recorded photographically (Powershot G3, Canon) in the field of a circular polariscope (Sharples 2026). The polariscope was placed into the universal test machine; the placement order from back to front was as follows: white light, source polaroid plates, the model, quarter-wave plates, and the photographic machine.
Photoelastic Models of Prostheses. (a) Two Implant-Supported Overdentures (IO) – Locator. (b) Two Implant-Supported Removable Partial Dentures (IRPD) Bridge + Clasp. (c) Two IRPD Bridge + Precision. (d) Two IRPD Crown + Clasp. (e) Four IO - Bar. (f) Four IRPD Bridge + Clasp. And (g) Four IRPD Bridge + Precision
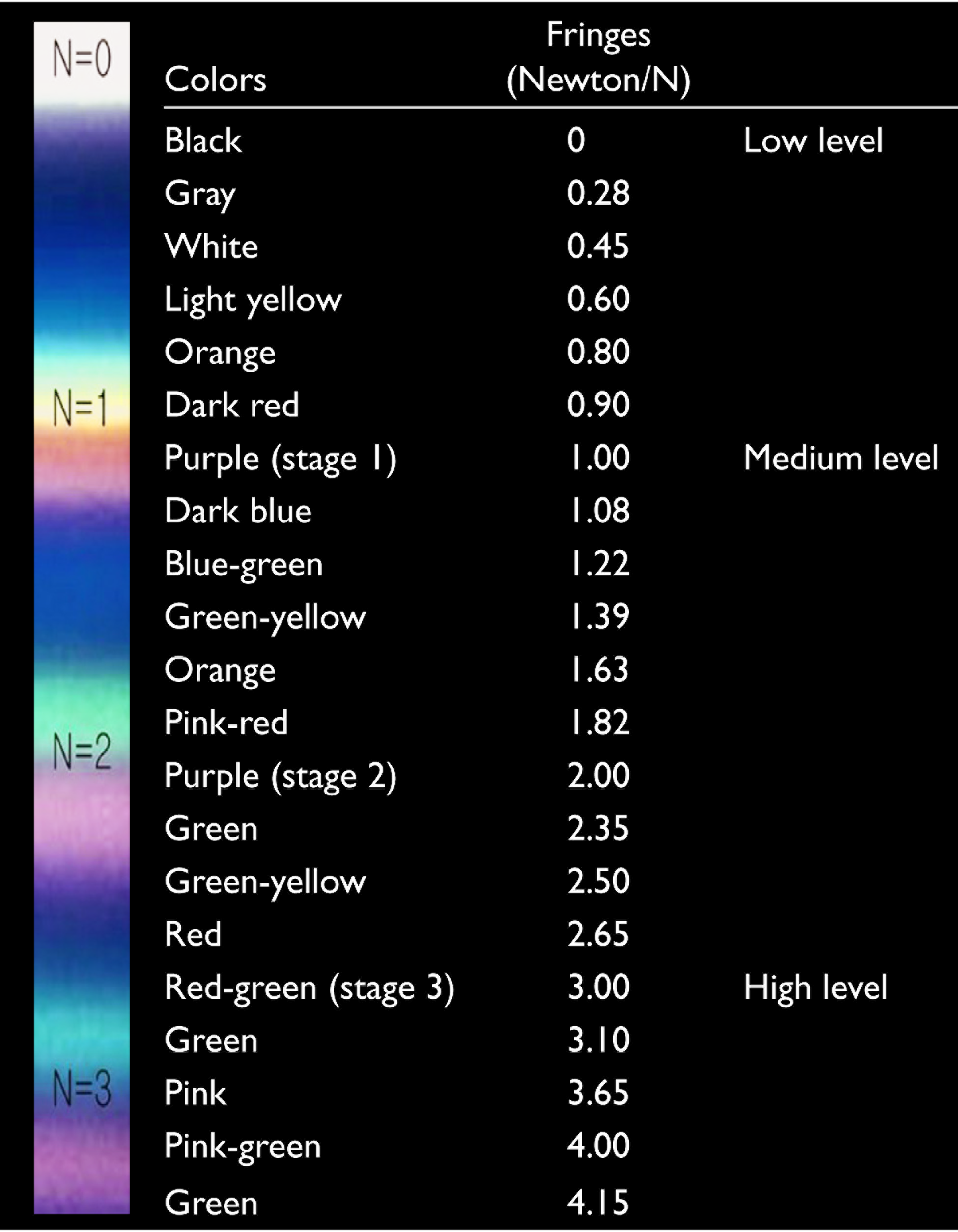
The stress fringes showed some properties such as color, frequency, and distribution that state the amount of strain. Fringes were composed of different color bands (isochromatic), and the border of these isochromatic fringes was determined by the amount of strain. The characteristic properties of isochromatic fringes are expressed numerically in Table 1.15,16
Isochromatic Fringe Values for Interpretation of Photoelastic Stresses
Results
Loading on the right and left side produced similar fringe patterns. Therefore, only results from the right side are presented. In particular, medium level stresses occurred in the regions numbered 1, 2, 3, and 4 (1.08-1.39 N) in the region of the implant on the loading side for IO prostheses with locator attachment that were combined implant-tissue supported. In addition, the fringes occurred in the crest region on the loading side. Low levels of stress generation were observed in the regions numbered 6 and 10 (0.28 N). The stress values in the apical regions of the implants were higher than in the neck regions (Figure 2a).
Stress Fringes of Dentures with Two Implants. (a) Stress Fringes of Dentures with Two Implants with Locator Attachment. (b) Stress Fringes of Removable Partial Dentures Over Implant with Two Bridge-Supported Clasp Attachment Implants. (c) Stress Fringes of Removable Partial Dentures Over Implant with Two Bridge-Supported Precision Attachment Implants. (d) Stress Fringes of Removable Partial Denture Over Implant with Two Crown-Supported Clasp Attachment Implants
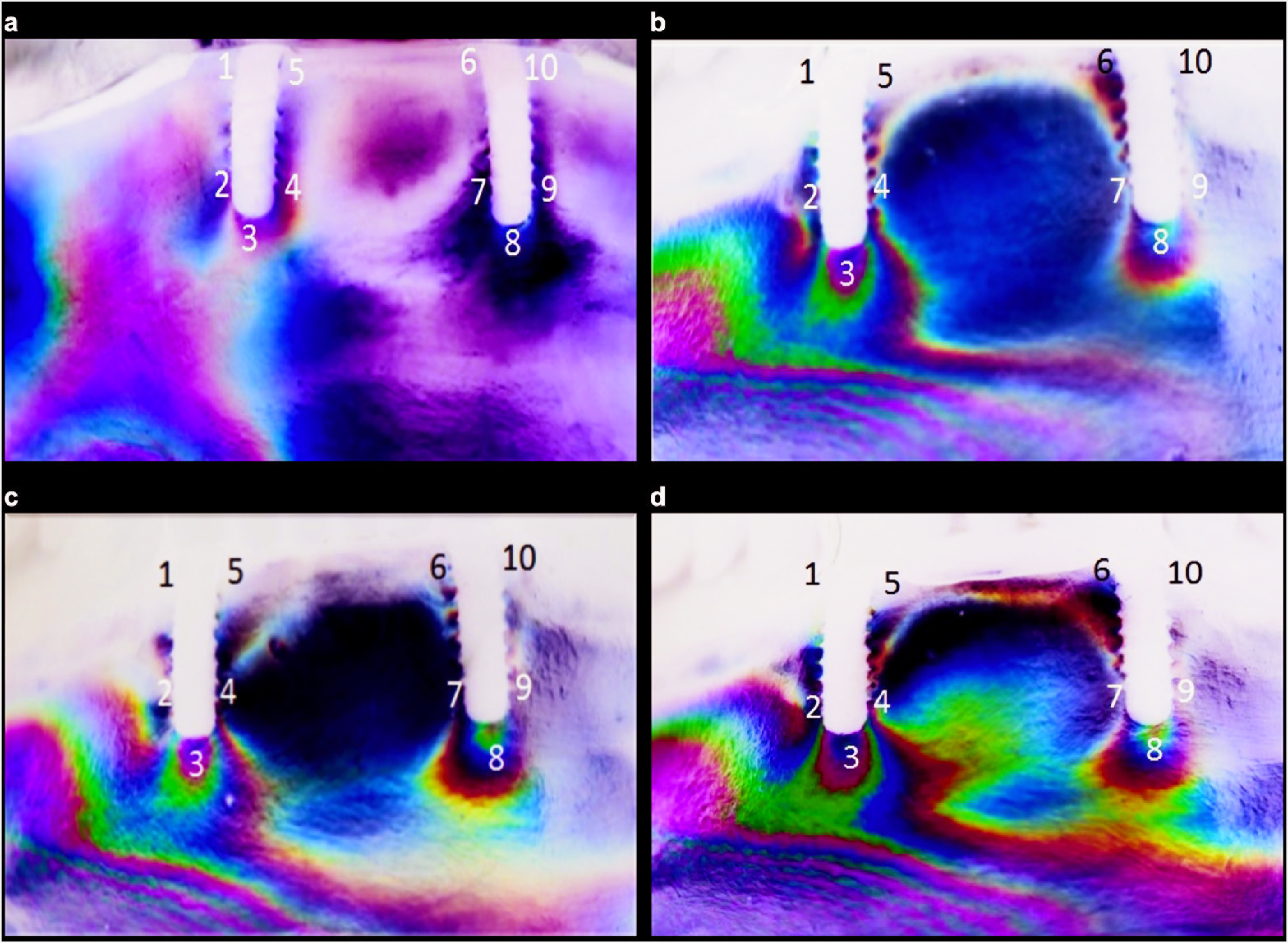
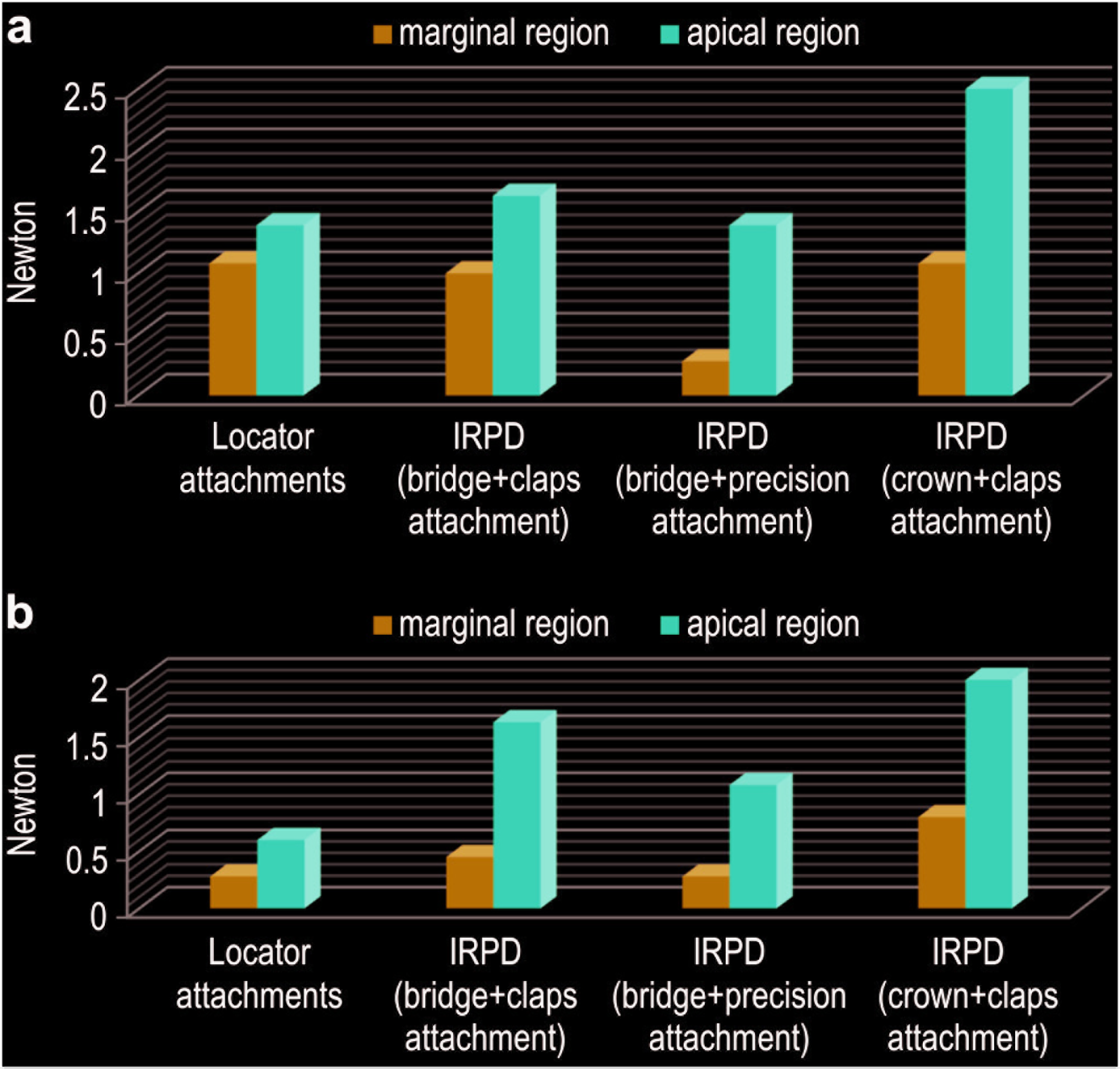
In region 8, medium level stress fringes was observed (1.63 N) for the IRPD with bridge design and clasp attachment. More fringes occurred in the apical than the neck region of the implants. A higher level of stress accumulation was observed on the loading side in the neck region of the implant regions 1 to 5 (1.00 N) than that in the neck region of the opposite side implant regions 6 to 10 (0.45–0.28 N; Figure 2b). Stress generation in region 8 for the two IRPD bridge + precision attachment was 1.08 N. Low levels of fringe line formation in regions 1, 5, 6, and 10 (0.28 N) was observed, and that the stress accumulation in the neck regions was lower in the models with precision attachment (Figure 2c). Stress generation in region 8 of the IRPD with a crown design and clasp attachment was 2.00 N, in region 1 it was 1.22 N, and in region 5 it was 1.00 N. The stress concentration was higher in the apical regions of the implants than in the cervical regions of the implants. (Figure 2d, Figure 3).
Stress Fringe Orders Around Loading Sides of Implants for Dentures with Two Implants. (a) Fringe Orders Around Loading Sides of Ipsilateral Implants for Two Implant-Supported Prosthesis: Apical and Marginal Regions. (b) Fringe Orders Around Loading Sides of Contralateral Implants for Two Implant-Supported Prostheses: Apical and Marginal Regions. IRPD, Implant-Supported Removable Partial Dentures
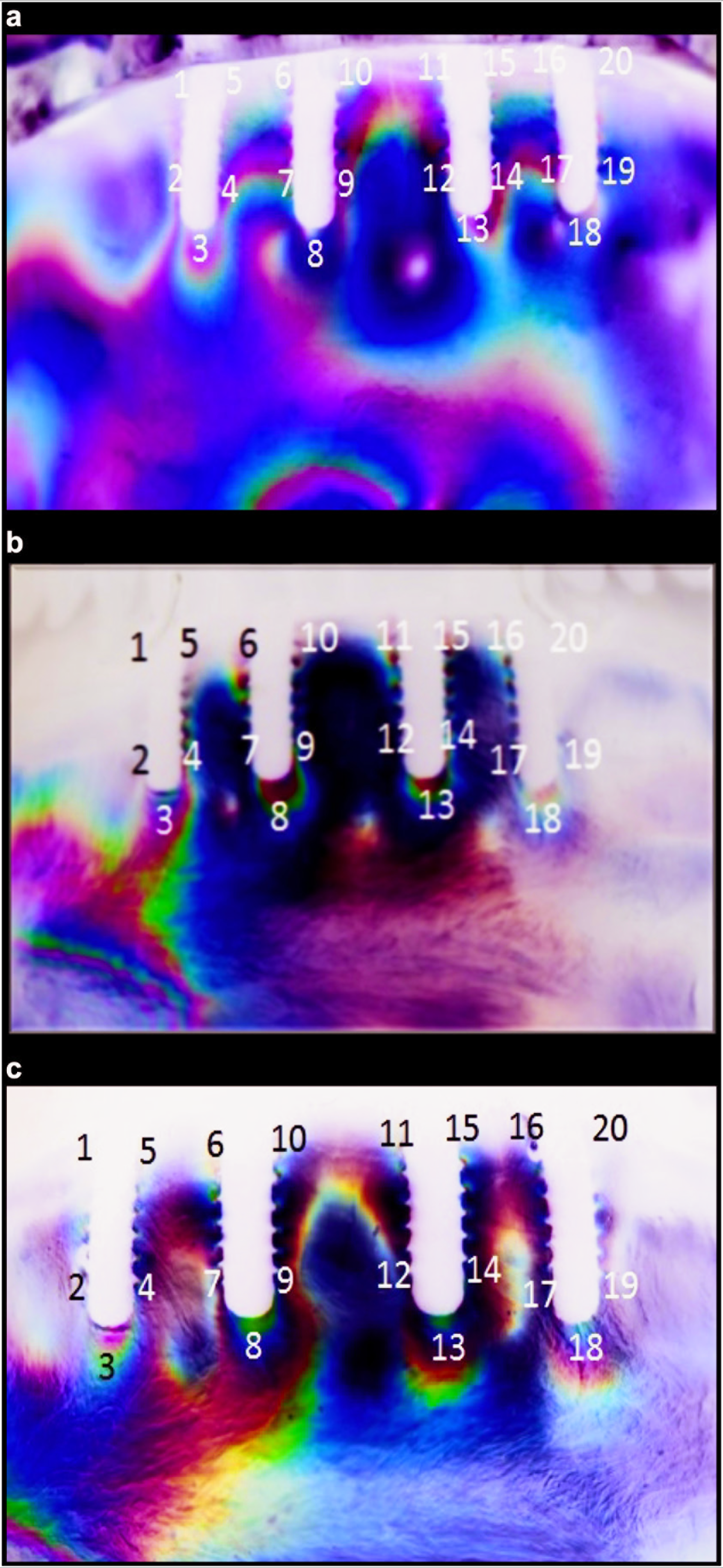
A greater concentration of stress was observed in the overdenture prosthesis with bar attachment IO than the locator attachment. However, stress concentrations occurring not only on the loading side implants but also on the opposite side implants (regions 11, 13, 15, and 18; 1.22–1.08 N). Fringes formed with reduced tissue support were less sparse than those in the edentulous areas. (Figure 4a). Medium level stress (1.08–1.39 N) fringes occurring in regions 1, 3, 5, 6, 8, 11, 13, 16, and 18 for the IRPD with clasp attachments. Lower stress concentrations were observed in the neck regions of the loading side and opposite side implant regions (Figure 4b). Stress fringes occurred on the second, third, and fourth implants for the IRPD with precision attachments. In general, as in all models, the lowest level of stress distribution was observed in the implant in the farthest region from the loading side (regions 16, 18, and 20) while high stress concentrations were observed in the implants on the loading side (regions 1, 3, 5, 6, and 10). Lower stress concentrations have been observed in the neck regions in a similar way with the clasp attachment (Figure 4c, Figure 5).
Stress Fringes of Dentures with Four Implants. (a) Stress Fringes of Overdenture Total Prosthesis with Four Implants and Bar Attachment. (b) Stress Fringes of Removable Partial Denture Over Implant with Four Implants and Bridge-Supported Clasp Attachment. (c) Stress Fringes of Removable Partial Denture Over Implant with Four Implants and Bridge-Supported Precision Attachment
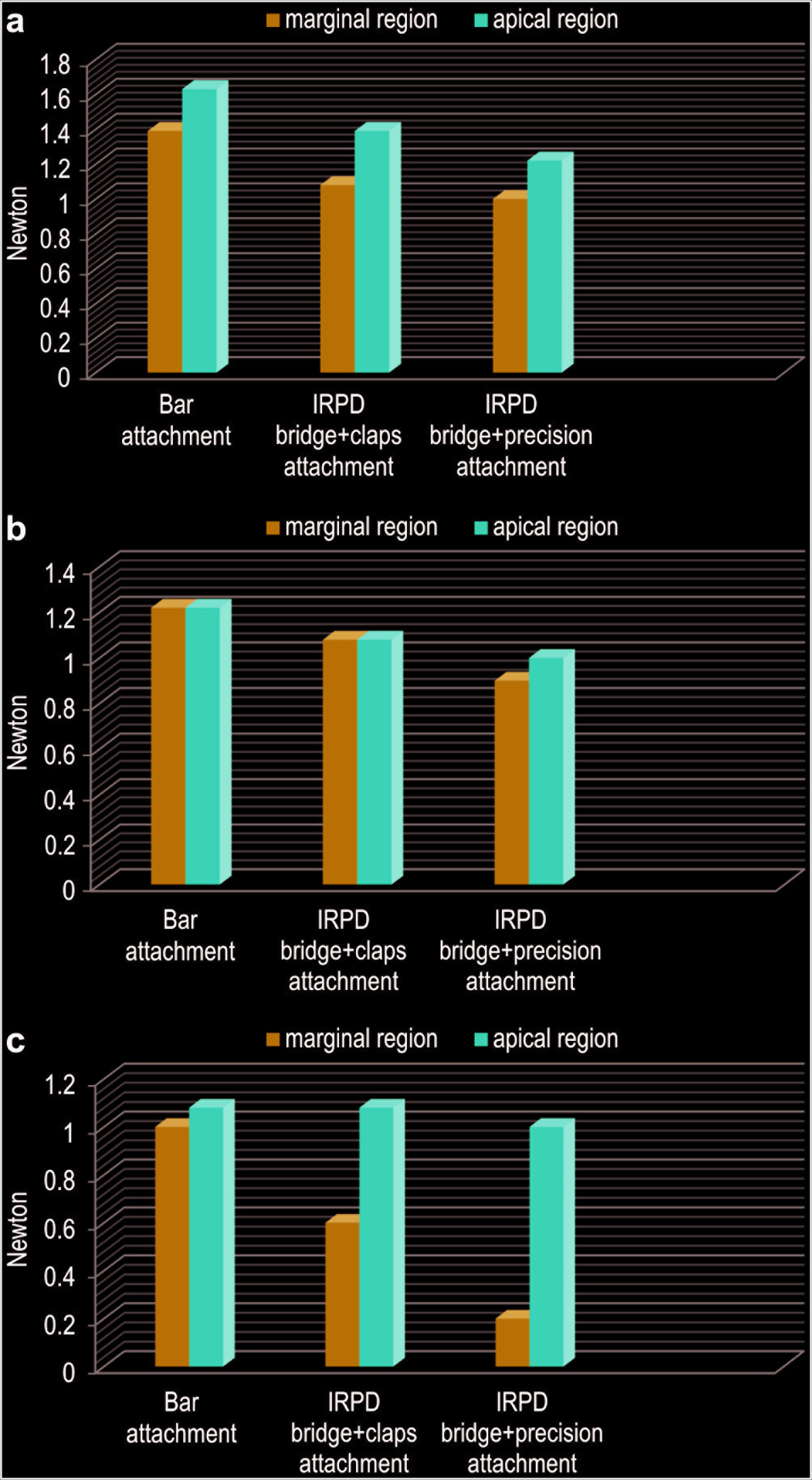
Stress Fringe Orders Around Implants for dentures with Four implants. (a) Fringe Orders Around Loading Side of Ipsilateral Implants for Four Implant-Supported Prostheses: Apical and Marginal Regions. (b) Fringe Orders Around Median Implants for Four Implant-Supported Prosthesis: Apical and Marginal Regions. (c) Fringe Orders Around Loading Side of Contralateral Implants for Four Implant-Supported Prosthesis: Apical and Marginal Regions. IRPD, Implant-Supported Removable Partial Dentures
Discussion
Results indicate that the overdenture with locater attachments show minimal stress concentration compared with IRPD for the two implants models; however, in the locater attachments, fringes were observed only around the loaded side implants because of nonsplit attachment-type of implant design. For IRPD, bridge design with precious attachments demonstrates minimum stress compared with the crown design and clasp attachments-type designs for both the two and four implants models.
In many studies, stress patterns in the photoelastic model have been reported to be very similar to those of natural structures. 17 This is because the stress distribution can be observed directly in the model and there is a similarity among the shape of stress, the area where it is formed, and natural structures. In photoelastic stress analysis models, cortical and cancellous bone are composed of a single resin. Therefore, even if the amount of stress changes, the areas where stress occurs will not; therefore, this method is useful for comparing stresses occurring in different prosthetic designs. 18 Maximum biting force in individuals with natural teeth differ individually in different areas of the jaw. The largest biting force has been previously measured in premolar region at 415 N for females and 475 N for males. Average values of bite forces in premolar region for females 345 N and 401 N for males. 19 Mericske-Stern and Zarb evaluated occlusal forces in a group of partial edentulous patients treated with an implant-supported fixed partial prosthesis and determined the maximum occlusal force to be 200 N for the first premolars and 300 N for the second premolars. 20 In our study, a 300 N20,21 vertical force was applied to the right and left first premolars. The reason for the selection of this loading site being that food is chewed between premolars and molars in anterior loading applications. 16 In addition, the shortened dental arch concept that came to the fore in the 2000s also reported that the premolar regions are sufficient for occlusal chewing. Especially in older adults, the use of shortened dental arch for the health of the remaining teeth or implants and surrounding tissues and for the protection of temporomandibuler joint has become a current issue. 22 Since the alternative prosthesis design mentioned in our study was mostly used in older adult patients, we preferred applied occlusal loading was made from the premolar region.
In a previous study, as a result of the application of laterotrusive load, a low level of stress was observed on the nonworking side of the implant in the bar-ERA attachment, and the opposite arch interaction was determined to be low by providing balanced side contact. 23 Furthermore, the highest stresses were formed in the posterior implants on the loading side.14,23,24 In our study, similar to the results of previous studies, the highest stress value in all models occurred in the posterior implant on the loading side. El-Anwar et al. 25 reported an FEA study compared the stress transmission of ball and locater attachments in edentulous mandible, as a result of the application of unilaterally load, a low level of stress was observed on the nonloaded side of the implant in the locater attachment. In addition, more stress accumulation was observed in the loaded side mucosa in systems with locater attachment. Similar to the results, the lowest stress level was observed in locator attachments where the implants were not splinted. In the study of Celik and Uludag, the fact that there were higher stress values in the locator attachments, in contrast to the present findings, might be because of the different retention forces of the retentive rubbers used. 26 In our study, a blue-colored retentive rubber with a retention force of 1.5 lbs = 66.7 N was used. This rubber was selected because the incoming forces are transmitted between the retentive rubber and the locator abutment, and a lower load is transferred to the implants. In this case, resilient design provides appropriate stress distribution characteristics. 26
In addition, the fact that a lower stress concentration was observed around the implant in the model with locator attachment may be because of the location of the implant further away from the loading site in the locator attachment. The increased mucosa support may also be because of the fact that a portion of the force is transmitted to the alveolar crest on the loading point.25,27,28 While very low stress was observed in the implant on the nonloading side in the locator attachment, a moderate level was observed in the middle implants in the bar attachment and a low stress was observed in the opposing implants. This can be explained by the fact that the implants are connected to the bars and the stress is transferred to the other implants via the bar and the locator attachment, a resilience attachment preventing implant overloading.25,29 However, the lack of stress distribution to the contralateral implant in the model with a locator attachment may be risky in terms of both bone loss monitoring in the implants on the loading side because similar to the results of Amornvit et al. 30 and Sheng-Chang et al. 31 when the force was applied along the long axis of the implant, the maximum stress was located around the neck of the implant and that may cause the bone resorbtion, in particular, the deformation of locator attachment rubbers because of single side loading. Zarei et al. 32 reported that increased number of implants 2 to 4 for edentulous mandibuler anterior region, reduces the amount of the stress around the implants. Also in the present study, more stress fringes were observed in the overdenture prosthesis with bar attachment IO than the locator attachment. However, stress concentrations occurring not only on the loading side implants but also on the opposite side implants (1.22–1.08 N) indicated that the load was distributed equally to all implants by splinting. Fringes formed in this type of prosthesis with reduced tissue support were less sparse than those in the edentulous areas.
Hu et al. evaluated the stress transfer of different overdenture attachment systems loaded directly over the implants, second premolar, and second molar regions. The authors stated that stress transfer to the edentulous crest region occurred and the stresses in the implants decreased as they approached the posterior area. At the same time, they observed that the difference between the stress transfer of overdenture attachment systems was also reduced as the load applied shifted to the posterior. 28 In our study, the low and moderate levels of stress values observed instead of high stress values, and the stress lines occurring in the region of the edentulous crest, might be because of the application of force from the premolar region. However, the stress lines observed in parts of the edentulous crest were greater in the two implant-supported models than in the four implant-supported models. This finding is comparable to those of a 10-year clinical follow-up by De Jong et al. in which the residual crest resorption of mandibular overdentures with two and four implants was compared. 33 De Jong et al. concluded that a significantly greater atrophy was observed in the cases with two implants than in the cases with four implants. This result was observed to be independent of peri-implant bone loss, and this atrophy was believed to be formed because of the movement of the posterior prosthetic base towards the tissue under occlusal forces.33,34
There are many case reports in which researchers have used removable partial dentures combined with implant-supported fixed prostheses.6,8–11,34–36 Clinicians usually experience difficulty in providing effective and affordable implant restorations for patients with resorbed edentulous jaws. The resorbed residual alveolar crest and other anatomical limitations can prevent the placement of implants in the desired positions, especially in the posterior regions of the mandible.37,38 Implant placement in posterior areas of the jaws with anatomical limitations may be difficult or may require advanced surgical techniques. Despite these anatomical limitations, implant placement in the anterior regions of both jaws is generally reliable.37–39 The effective use of implants with a minimal number of removable dentures provides a more economical and comfortable treatment option for edentulous patients.38–40 Some of the total edentulous patients prefer implant-supported fixed restorations in the anterior region and removable partial dentures without requiring advanced surgical methods in the posterior regions while treatment options are being discussed. 9
The present study evaluated the different IRPD designs, also. This study is the first report evaluating the different type of IRPD designs. According to our results, the stress concentration of crown-support and clasp attachment prosthesis was higher in the apical regions of the implants than in the cervical regions of the implants. However, when compared with other precious attachment models, the dentures with two implants with crown-support and clasp attachment generated higher stresses in the neck region, which can lead to marginal bone loss. It is thought that the use of precision attachments in IRPD prevents bone resorption in the implant and its surrounding.39–40
Bilhan et al. evaluated the stress transfer of two-interforaminal implant-retained bridge and a removable partial denture with strain gauge method. 29 They reported that, according to retentive anchors or bar attachments, the lowest strains occurred in the new design IRPD. This supports the results of our study. In the models with both two and four implants, the precision attachment of removable partial dentures generated less stress concentration then clasp attachment designs. Also splitting the anterior implants decreased the stress observation around the implants for this new treatment protocol. Crown design IRPD with clasp attachment was observed the highest stress values around the implants.
As mentioned in the case reports in the literature, the use of IRPD in total edentulous jaws enables more comfortable patient movement in terms of chewing, esthetics, and speech.6,10,37 When an overdenture is compared with full dentures, the pressure forces in the residual crest are also less common in IO prostheses. 40 At the same time, chewing movements become more balanced and regular in patients using IRPD.38–40 Bilhan et al. also mentioned that the new design implant supported anterior bridge retained removable dentures with precision attachments eliminates two problems of conventional systems ease of hygiene with regard to bar attachment prosthesis and increased stability in severe resorb mandible according to single attachments. 29
As shown in a clinical study comparing removable partial dentures and conventional total prostheses; while the retention and comfort satisfaction of patients using removable partial dentures for mandibular prostheses was higher, a greater dissatisfaction in total prosthesis patients with mandibular prostheses was recorded. 41 This suggests that the use of IRPD in total edentulous mandibular jaws is more appropriate. Collapse is observed in all physiological functions with old age; therefore, implant overdentures in elderly individuals should be designed to show satisfactory retention, be easily placed and removed, easy to clean, and cover a minimal surface area. In addition, it is important for younger total edentulous patients to feel comfortable in social settings with increased retention and to meet their esthetic expectations. 30 IRPD and implant-supported fixed prosthetic restorations in the anterior region can have esthetic and psychologically positive effects so increase the self-confidence for young patients. In addition, prosthesis parts requiring less space for older patients can offer less complex retentive structures, and prosthetic components that will cause less plaque accumulation and are easy to maintain. Besides, in a recent study, wear of the matrices of unsplinted attachments are more remarkable especially the implants inserted not parallelly, 42 that cause more adjustment and maintenance in a short span of time. It was mentioned that splinting the angulated implants is a suitable solution and IRPD may also be a good alternative in this situations.
The present study is in vitro and presents limitations as follows: In vivo studies and studies with other methodologies, such as
finite element and strain gauge analysis, are necessary to complement
the results found. Stress transmission evaluated with static occlusal loads that
limits the generalizability of our results. In fact, natural chewing is
a dynamic movement and involves oblique forces. It would be beneficial
for future studies to evaluate the stress transfer under different load
directions. In this study, implant-supported removable prosthetic designs were
compared but for edentulous mandibles implant-supported fixed prosthetic
design such as hybrid prosthesis are commonly used in clinically.
Therefore, for future studies both fixed and removable types can be
investigated to extend the comparison.
Conclusions
In line with the results of this study, the following conclusions were drawn: for two implant-supported locator attachment prostheses, less stress was observed compared with the overdenture prosthesis with four implant-supported bar attachment prostheses. However, it should be considered that the stresses generated in the edentulous crest region are higher in the two implant-supported models. For IRPD with precision attachment, the stress concentration was similar in two and four implant-supported removable dentures but was less than in clasp attachment designs. However, IRPD with precision attachment in the models with four implants showed lower stress intensity compared with the IO prosthesis and the IRPD with clasp attachment.
Based on the findings, it can be concluded that IRPD prosthesis retained by an anterior bridge design with precision attachments is a suitable alternative treatment option. In particular, it can be used for patients who have anatomic inhibitions for full-mouth implant-supported fixed prosthesis, high esthetic expectations, denture adaptation difficulties, and inclined implants that block the retention of bar and locater attachments.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study received financial support from Selcuk University Research Committee (grant# 111020222) and also was supported by the Scientific Research Projects Coordination Unit (grant# 11102022). The funders have no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.