
Abstract
Radicular cysts are the most common inflammatory cysts of the jaws. Surgical intervention aims to eliminate periapical pathology in order to allow bone regeneration and healing of periapical tissues. Autologous platelet-rich fibrin is a healing biomaterial in oral surgical defects with the new perspective of accelerated healing. Titanium-prepared platelet rich fibrin (T-PRF) is a third-generation platelet concentrate developed to overcome the harmful effects of silica in glass tubes and also has a longer resorption rate. The purpose of this case report is to present the effects of T-PRF applied to the bone defect that occurs after the enucleation of the radicular cyst. A significant increase in bone density was observed after eight months of follow-up. T-PRF has been shown to be effective in the treatment of bone defects. Therefore, it is thought that it can be used as the only regenerative material in the treatment of bone defects.
Introduction
Radicular cysts are the most common inflammatory odontogenic cysts localized in the jaws. They develop from the epithelial remnants of the Malassez of the periodontal ligament, which are stimulated to proliferate by an inflammatory process originating from an infection or the pulp necrosis of a nonvital tooth with the development of a periapical granuloma. 1 The treatment of radicular cysts can be performed nonsurgically or by surgical methods such as marsupialization and enucleation, depending on the size and location of the cyst, bone integrity of the cystic wall, and proximity to vital structures. 1
Radicular cysts can cause large defects that require augmentation, and various materials are used for its healing, of which platelet-rich fibrin (PRF) is the second-generation platelet concentrate enriched with growth factors, where platelets lie between the top layer of acellular plasma and red blood cells at the bottom. 2 Titanium-prepared platelet-rich fibrin (T-PRF) is a new platelet concentrate based on the hypothesis that titanium tubes may be more effective in activating platelets compared to the glass tubes used in the method of Choukroun. 3 This case report presents the effective use of T-PRF following the enucleation of the maxillary cyst.
Case Report
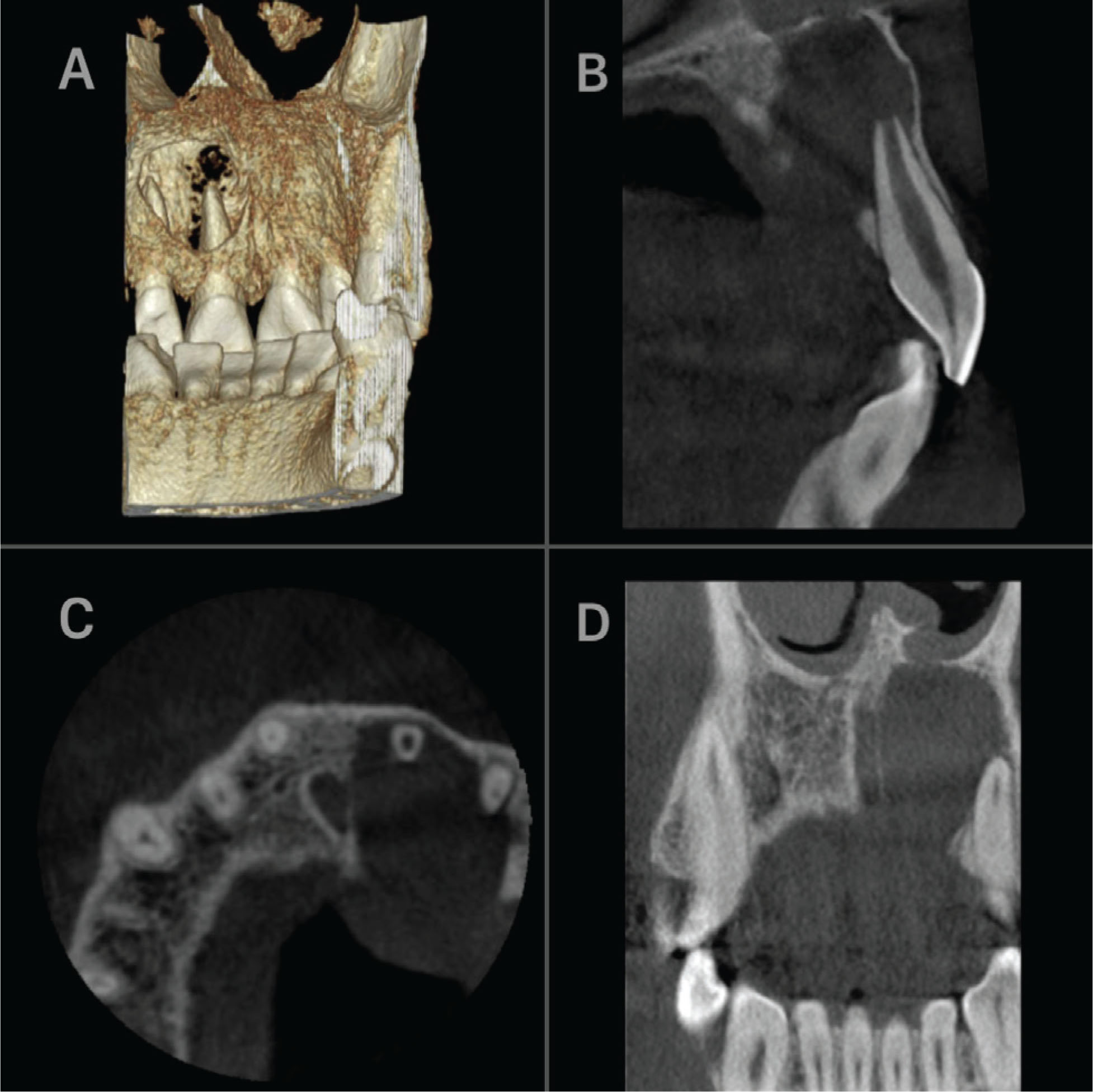
An 18-year-old male patient with no systemic disease presented to our hospital with the complaint of pain in the left upper jaw anterior tooth for ten days. There was a history of trauma about nine years ago. In the intraoral examination, there was a crown fracture at the enamel level in the left upper central incisor, and there was no mobility in the tooth. Fluctuant swelling was observed in the palatal mucosa extending from the central tooth to the canine area, and not exceeding the midline. A panoramic radiographic examination revealed round-shaped, well-circumscribed periapical radiolucency covering the roots of the teeth numbered 21 and 22 (Figure 1). It was observed that the pulp chamber of tooth number 21 was wider compared to the symmetrical tooth, and its apex was open. In the electrical pulp test, it was determined that the tooth numbered 21 was devitalized. In the cone beam computed tomography (CBCT), a round-shaped lytic lesion with regular margins was observed in the anterior region of the maxilla associated with the root of tooth number 21. Its dimensions were 14, 10 × 15, 69 × 17, 60 mm (buccolingual × mesiodistal × coronoapical). It had caused wide destruction in the palatal bone and it was expansile in the labial direction (Figures 2A–C). It had also caused thinning in the base of the nasal cavity (Figure 2D).
Preoperative Panoramic Radiography. Radiolucent Lesion in the Left Maxillary Anterior Region

Preoperative CBCT image of the cyst. In 3D reconstruction image (A) and the sagittal (B) and axial (C) sections, the destruction of the palatal bone and expansion in the labial direction (B). Thinning of the base of the nasal cavity in the coronal section (D)
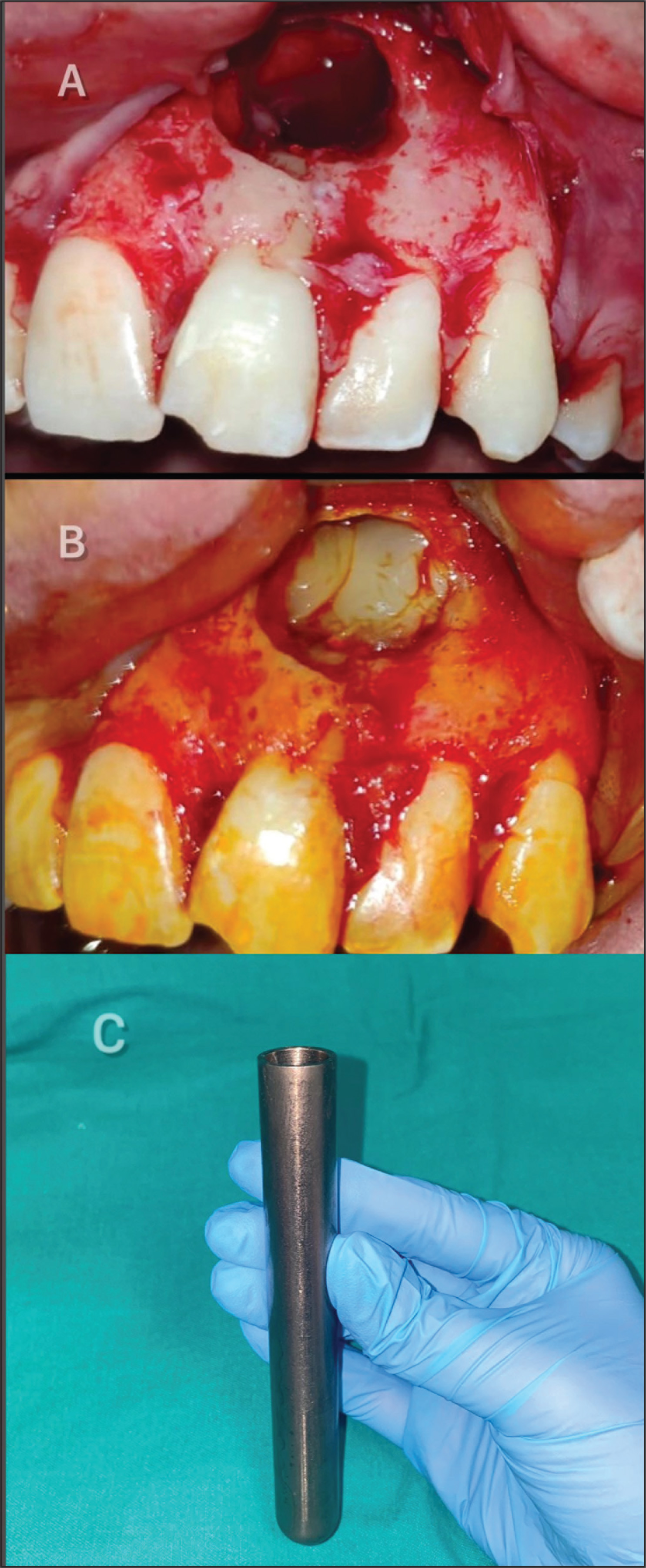
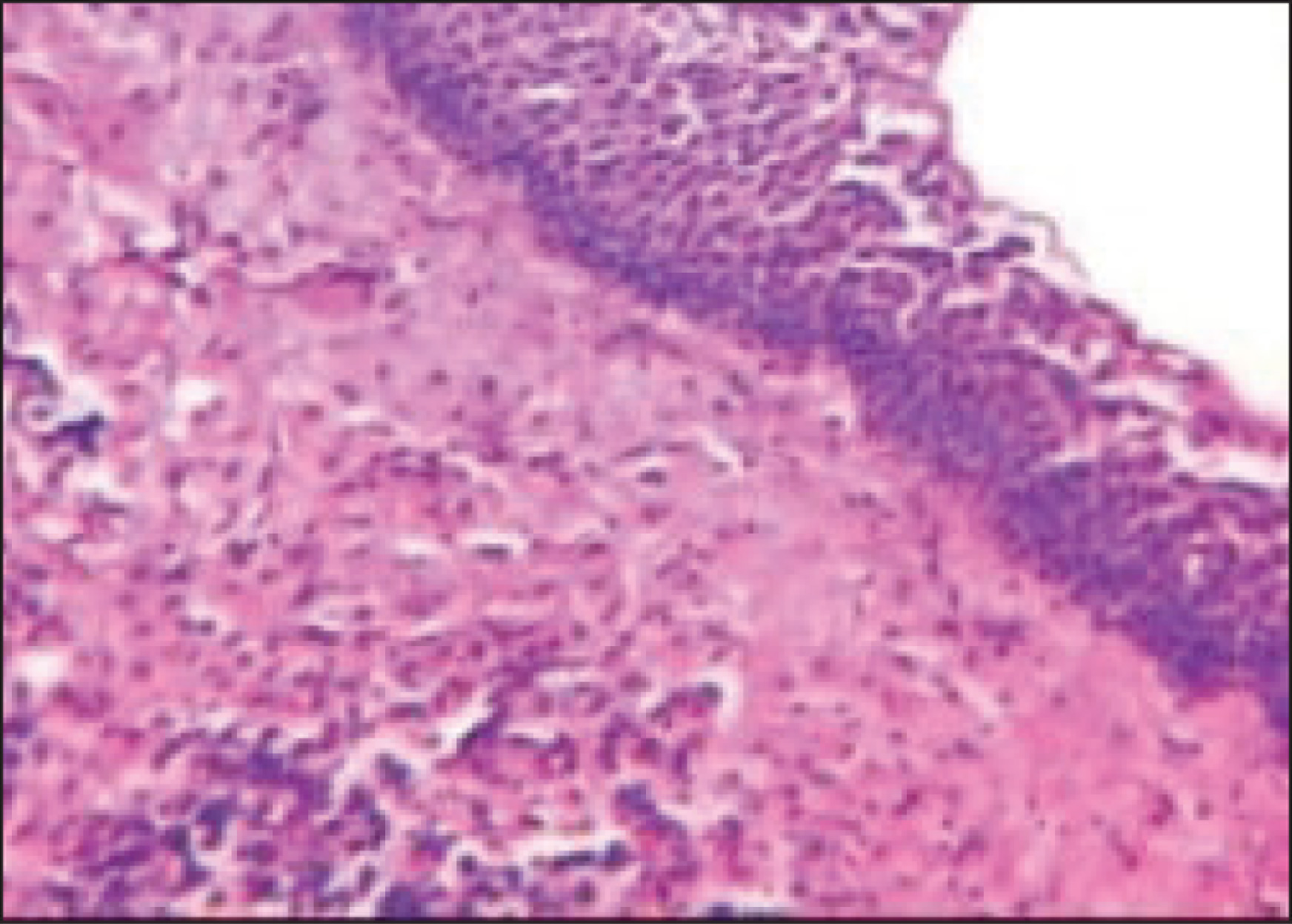
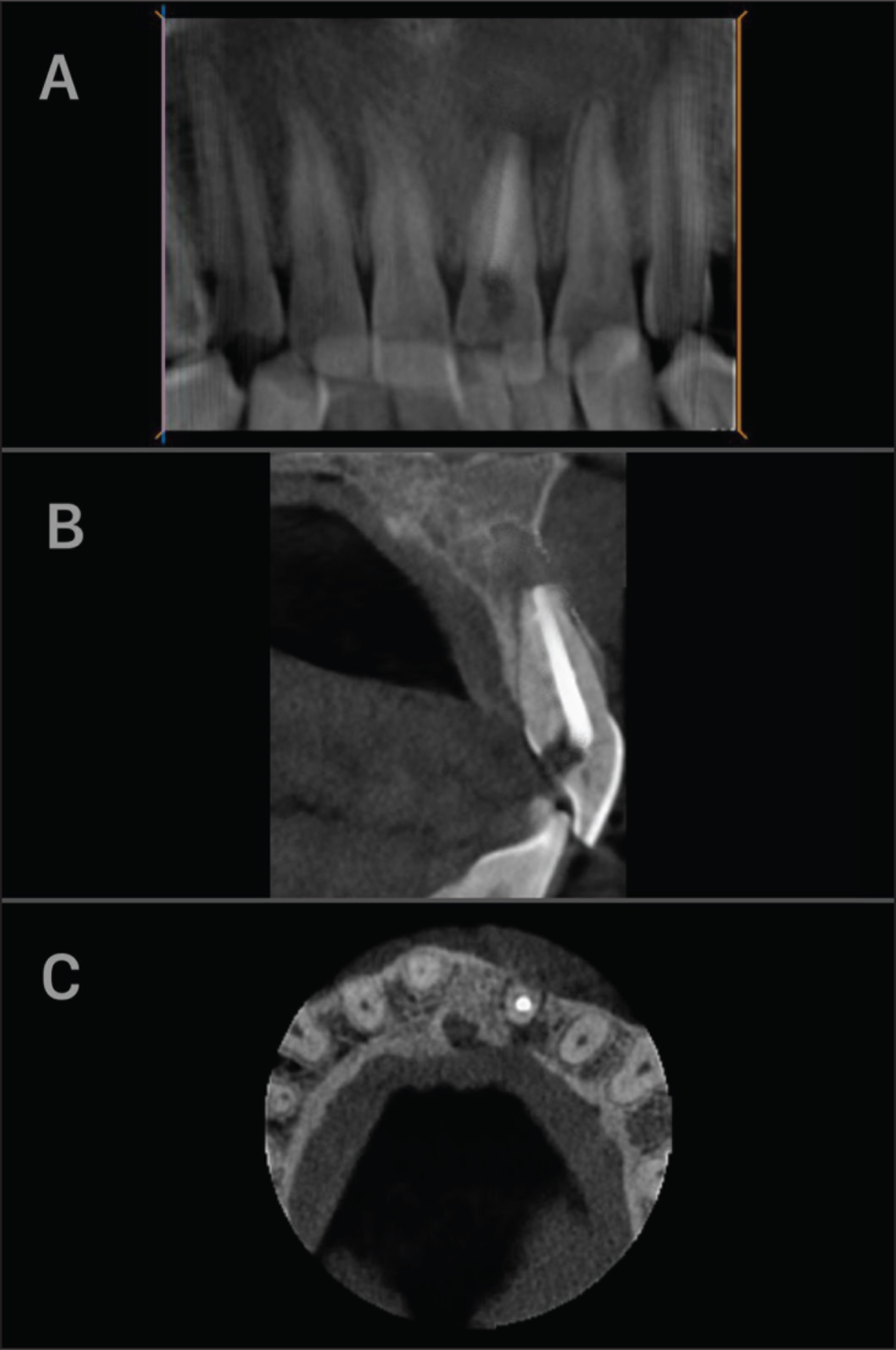
It was decided to enucleate the cyst following the administration of root canal treatment on tooth number 21 with the prediagnosis of the radicular cyst. Informed consent of the patient was obtained before the surgical operation. Under local anesthesia, the envelope flap was lifted from the area. The cyst membrane was accessed from the labial region, and the cyst was completely enucleated. Apical resection was performed on tooth number 21. Because of the large defect caused by the lesion after the enucleation (Figure 3A), it was decided to administer T-PRF to the operated area in order to accelerate the healing process. Similar to the conventional PRF procedures, T-PRF was generated by centrifuging blood taken from the patient into sterile titanium tubes without any anticoagulants (2800 rpm, 12 min). 4 (Figure 3C). The fibrin obtained was placed in the defect area (Figure 3B), and the flap was primarily sutured. The excision material was submitted for a histopathological examination, and it was reported to be compatible with the radicular cyst (Figure 4). Postoperative instructions were given to the patient; analgesic and antibiotic (2 × 1, amoxicillin + clavulanic acid 825/125 mg) drugs were prescribed for one week. The patient was maintained under a regular clinical and radiographic follow-up. In the eighth month follow-up CBCT, it was observed that there was bone formation in the peripheral of the lesion, and its size was reduced (Figure 5A). An increase in cortical bone was observed, partly in the labial bone and mostly in the palatal bone (Figures 5B and C). The postoperative course of the patient was uneventful, and no recurrence was observed.
Bone Defect (A) After Cyst Enucleation and T-PRF Applied to the Defect Area (B, C)
Histopathological View of a Radicular Cyst with Nonkeratinized Squamous Epithelium (Hematoxylin–Eosin Stain, ×100)
Increased Bone Density in Panoramic Reconstruction Image (A) and Cortical Ossification in Palatal and Labial Directions in Sagittal (B) and Axial (C) Sections
Discussion
Radicular cysts are the most common odontogenic cysts affecting the maxilla three times more than the mandible. Their occurrence in the anterior maxilla is more common; etiological factors may be trauma, caries, and old silicate restorations in the anterior teeth. 5 In the present case, the reason behind the lesion formation was trauma.
Radicular cysts are generally asymptomatic until they are detected on routine radiographs. These long-standing cysts sometimes exhibit acute exacerbation and give symptoms such as swelling, the mobility of teeth, and the displacement of an unerupted tooth. The teeth involved are always devitalized; they may sometimes change colors. Clinically, they are observed as buccal or palatal swelling in the maxilla, while it is usually buccal and rarely lingual in the mandible. At first, it is bony hard; however, as the size of the cyst grows, the bone wall becomes very thin. As seen in the present case, the swelling becomes fluctuant when the cyst completely resorbs the bone. 6
The treatment of radicular cysts depends on the size and location of the lesion. It can be treated with endodontic treatment, tooth extraction, or surgical procedures such as enucleation and marsupialization. 7 In the present case, root tip resection, surgical enucleation, and curettage of the cyst were preferred following the endodontic treatment. The primary objective in healing of surgical wounds with a large bony defect is the bone regeneration inside the defect in order to fill the cavity. Regeneration has been defined as the reconstruction or reproduction of a lost or damaged part in order to restore the structure and function of the periodontium. It is possible to achieve this with growth factors and bone grafts. 8 Many growth factors such as platelet-derived growth factor and transforming growth factor are released from PRF, affecting the healing of the wound and bone. Recently, PRF has been used as an autogenous graft material because of its ability to accelerate physiological wound healing and new bone formation. However, a silica-containing glass tube is required for the aggregation of platelet and formation of fibrin in PRF. Some researchers suggested that the silica particles in the glass tube can disrupt the fibrin structure and cause contamination during administration to the patient. 9 Tunalı et al. stated that titanium tube-induced platelet aggregation was similar to that found using glass tubes, and that the clot produced in titanium tubes was clinically identical to that in glass tubes. Although T-PRF is similar to conventional PRF methods, titanium-induced platelet activation provides characteristic features to T-PRF. Titanium is one of the metals with the highest corrosion resistance and strength-to-weight ratio. Titanium also has excellent biocompatibility, thanks to its noncorrosive properties.10,11 In addition, it was determined that the fibrin network formed by titanium tubes had a tighter network structure, the resorption period in the tissue was longer, and its osteoconductive property was good. 10
It was found that the use of T-PRF alone in sinus lifting procedures was successful in clinical and histomorphometric examinations. 12 In another study, it has been shown that T-PRF gives successful results clinically and radiographically in the treatment of intrabony defects. 13 In a clinical study in which 20 cyst cases were examined, after cyst enucleation, the use of autogenous PRF to the cyst cavity has been shown to yield successful results. 14 However, no study has been reported in the literature regarding the application of T-PRF alone to the cyst cavity. Therefore, we think that this case is the first case report of the use of T-PRF in the cyst cavity.
The use of T-PRF for the augmentation of the defect after enucleation was preferred in our case considering its positive features. As a result of the radiographic examination in the eighth month, satisfactory bone regeneration was observed. Complete bone formation was observed particularly in the palatal region, where the lesion caused severe bone destruction.
Conclusion
In the present case report, it can be considered that the use of T-PRF alone without bone graft provides regenerative benefits with good functional recovery. It can be concluded that T-PRF is effective in the augmentation of the bone defects. T-PRF is an autologous preparation, and it is more economical than other clinically effective regenerative materials available. However, more extensive and further clinical research is required to fully understand its effect on bone regeneration.
Footnotes
Acknowledgements
The authors would like to thank the patient for providing written informed consent for the publication of this case.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.