
Abstract
Aim:
To evaluate the periodontal status before and after orthodontic treatment and to analyze the confounding factors associated with it.
Materials and Methods:
The present retrospective study analyzed pre- and posttreatment records of a total of 60 patients. Intraoral digital photographs before and after the orthodontic treatment were used to measure the following three periodontal variables: (a) width of the keratinized gingiva, (b) gingival recession, and (c) the status of interdental papilla. The ImageJ 46 software imaging program was used to perform the required measurements. The clinical data were then analyzed in an association with the participants’ demographic data, the type of orthodontic tooth movement, and other confounding factors. The data obtained were manually entered into the statistical package and analyzed using a significance level set at P < .05. Descriptive statistics, paired t-tests, and Pearson’s correlation analysis were used to identify differences among the studied variables.
Results:
Among the 60 patients, the majority (66.7%) were females. Most cases of the treated malocclusion were Class II, and most patients underwent intrusion and retrusion movements. The width of keratinized gingiva increased for most sites of upper teeth. In contrast, the lower teeth showed a mix of improvement and compromised width of keratinized gingiva. As a measure of gingival recession, the difference of clinical crown height revealed the tendency toward a reduced clinical crown height for most sites. Upper left lateral incisors and canines showed significant values with regard to keratinized gingival width measurements and tooth movements such as extrusion and intrusion movements. Likewise, with regard to the clinical crown height, upper right central incisors showed significant differences when correlated with the interincisal angle, lower incisors to the mandibular plane, and upper incisors to the NA line. The upper lateral incisors also showed significant correlations to certain cephalometric measurements.
Conclusions:
The orthodontic treatment was found to exert a significantly positive impact on the surrounding periodontium, particularly in the upper canine areas. Likewise, various types of tooth movement were found to positively affect the periodontium.
Introduction
The healthy periodontium is mandatory for normal functioning of the teeth. The integrity of periodontal tissue components is essential for dental treatment mechanics, as periodontal compartments can influence certain treatment outcomes. In orthodontics, the center of resistance of a periodontally affected tooth would move apically, changing the magnitude and direction of the force needed to move that tooth safely. Periodontal problems have multifactorial influences. The extent to which these problems influence the malocclusion presentation and orthodontic treatment depends on the host resistance, compromised systemic resistance (diabetic and HIV), genetic conditions, behavioral influences (oral hygiene, smoking, diet), as well as on the composition of plaque in the gingival margin.1,2 Orthodontic movements may have an impact on the periodontal health status in different ways. Morphologically, orthodontics would change the position of the tooth, moving the periodontium to a healthier position. The biological effect of such treatment can be presented by the active turnover of periodontal ligament (PDL) cells and increase the likelihood that PDL would repopulate previously infected areas of the root surface. 3
Certain types of malocclusion, such as anterior deep bite, anterior crossbite, severe overjet, and overbite, can negatively affect the periodontium. Therefore, in order to improve the health of the periodontium, these types of malocclusion require correction.4,5 However, an association between malocclusion and periodontal health does not prove its causation and the subsequent orthodontic treatment may not restore periodontal health.1,4 The presence of orthodontic appliances and mechanical procedures may evoke soft-tissue responses in the gingiva, thereby reducing the efficient removal of bacterial biofilms. In order to evaluate gingival inflammation after the orthodontic appliance placement, previous studies used various indices, including the plaque index, gingival index, bleeding on probing, pocket probing depth, Quigley–Hein index (for bonded molars), bonded bracket index (for bracketed teeth), and a modified gingival index. Based on these indices, orthodontic appliances were found to act as reservoirs for bacterial plaque accumulation.6–8 Furthermore, Knoernschild and coauthors 9 found that orthodontic brackets retain an affinity to lipopolysaccharides (a product of a Gram-negative bacterial cell wall), which is dependent on the material composition, surface energy, and surface porosity.
The potential impact of specific orthodontic tooth movements has been widely investigated in the literature. It has been reported that the intrusion movement may increase the subgingival plaque; the teeth already harboring bacteria can develop infrabony pockets.10–12 However, in patients with healthy periodontium and dentition, intruding the teeth would promote connective tissue reattachment or else lead to the creation of new attachment caused by the stretched PDL.13–16 Extrusion movements can reduce infrabony pockets because of the coronal positioning of the connective tissue (attached gingiva moved by 80% of the extruded distance), thereby improving the alveolar bone defects, gingival aesthetics, and crown-to-root ratio.17,18 Therefore, both intrusion and extrusion can have favorable outcomes. Furthermore, the torque movement by lingualization of the tooth showed an increased bone apposition.19,20 Proclination of the anterior teeth is usually performed in orthodontics to camouflage certain malocclusion characteristics. Proclination movement rarely produces gingival recession, in such a condition that it does not exceed an acceptable limit (no more than 10 degree). 21
There are several complications of orthodontic teeth movements, such as recession, increased pocket depth, and alveolar bone loss. Localized gingival recessions have been reported to be caused by many etiologic factors, including trauma from occlusion, high frenal attachment, impingement of restorative margins, and increased orthodontic forces. 22 In order to determine the susceptibility to recession, the volume of gingival connective tissue has a greater significance than its width, and this has led to the recognition of thin gingival biotype as a risk factor for recession. 23 Interdental papilla has important functional and aesthetic roles. The interdental papilla status is influenced by the distance from the contact point to the bony crest, the divergence of roots of teeth,24–26 malformed teeth (wide incisally, narrow cervically), prominent frenum, and inter- and intra-arch tooth size discrepancies. 27
Overall, the major aim of the orthodontic treatment is to procure a healthy status of the periodontium as the ultimate outcome. 28 Although the response of the periodontium to orthodontic treatment has been widely investigated, very few studies have focused on the impact of specific orthodontic movements. Furthermore, most of the relevant studies did not consider multiple confounding factors associated with the orthodontic treatment and the potential periodontal changes induced by it. To bridge this gap in the literature, the aim of the present study was to evaluate the status of the periodontium before and after orthodontic treatment and to analyze the impact of the confounding factors associated with it.
Materials and Methods
This retrospective study was conducted on the records of 60 orthodontic patients, who visited the Orthodontic Clinic at the College of Dentistry, King Saud University, Riyadh, Saudi Arabia, from January 2013 to December 2013. First, in order to assess the needed sample size, sample size calculation was performed. The results showed that, in order to achieve the power of 80% at the 0.05 level of significance, 60 participants would be needed to detect a difference of 0.8 mm of keratinized gingival width, based on a previously published study. 29 Accordingly, pre- and posttreatment orthodontic records of a total of 60 patients were reviewed.
All participants fulfilled the following four inclusion criteria: (a) healthy individuals with no medications that could have altered the periodontium response, (b) no history of smoking (for adults), (c) no preexisting periodontal disease, and (d) no clear evidence of the deteriorating periodontal condition during orthodontic treatment. The participants were selected by convenience sampling, where each of the patients had a complete treatment record. These records included the treatment plan, progress notes, and final case analysis.
Digital photographs before and after orthodontic treatment were used to measure the following periodontal variables: the width of the attached gingiva, the width of keratinized gingiva, the loss of keratinized tissue, the presence of recession, the amount of recession, the presence of interdental papilla, and the amount of loss of the interdental papilla. In addition, the demographic variables such as patients’ age and gender were also collected. In the next step, the patients’ orthodontic progress and treatment notes and records were used to collect information about the following potential confounding factors: oral hygiene, molars classification, the amount of the overjet and overbite, the presence of crowding, treatment strategy (nonextraction, upper extraction, lower extraction, and upper and lower extraction), the use of intermaxillary elastics, and the type of movements (intrusion, extrusion, retrusion, protrusion, and controlled tipping).
The ImageJ 46 software system (J46, the National Institutes of Health, USA) was used to perform all measurements. The width of keratinized gingiva was measured from the marginal gingiva until the mucogingival junction, to detect the differences up to 0.01 mm. The clinical crown height was evaluated by measuring the tooth height from the midpoint (by drawing a box and calculating the midpoint) until the incisal edge. 30 Randomly selected photos were measured twice for all variables before the data collection phase. An intraclass correlation test was applied to investigate intraexaminer reliability.
Statistical Analysis
All data were then analyzed using the SPSS software statistical package (version 20, SPSS Inc., Chicago, IL). First, descriptive statistics (mean, median, range) were computed for each of the variables. Then, a paired t-test was used to test for statistically significant differences of periodontal indicators between the means of the pre- and posttreatment groups. Finally, Pearson’s correlations among the studied variables were computed.
Results
Medical records of a total of 60 patients (66.7% females) who fulfilled the inclusion criteria were added to the sample for further analysis. Table 1 indicates descriptive statistics of the pre- and posttreatment such as age, treatment duration, and overjet and overbite values. At pretreatment, most patients were in their teen years (mean age: 15.7 yr). The mean treatment duration was 2.4 yr, which falls within the normal range of the duration of a comprehensive orthodontic treatment. Furthermore, as reflected by the range reported for the overbite and overjet values, the sample contained a wide range of malocclusion discrepancies.
Descriptive Statistics of Pre- and Postorthodontic Treatment Records

Most of the treated cases were Class II malocclusion (n = 26; 43%), followed by Class I (n = 22; 37%) and Class III (n = 12; 20%). Most patients underwent intrusion and retrusion movements (51.7%), rather than extrusion and protrusion (31.7%; Table 2).
Frequency Distribution (%) of Extrusion, Intrusion, Protrusion, and Retrusion Movement in the Sample for the Upper and Lower Arch

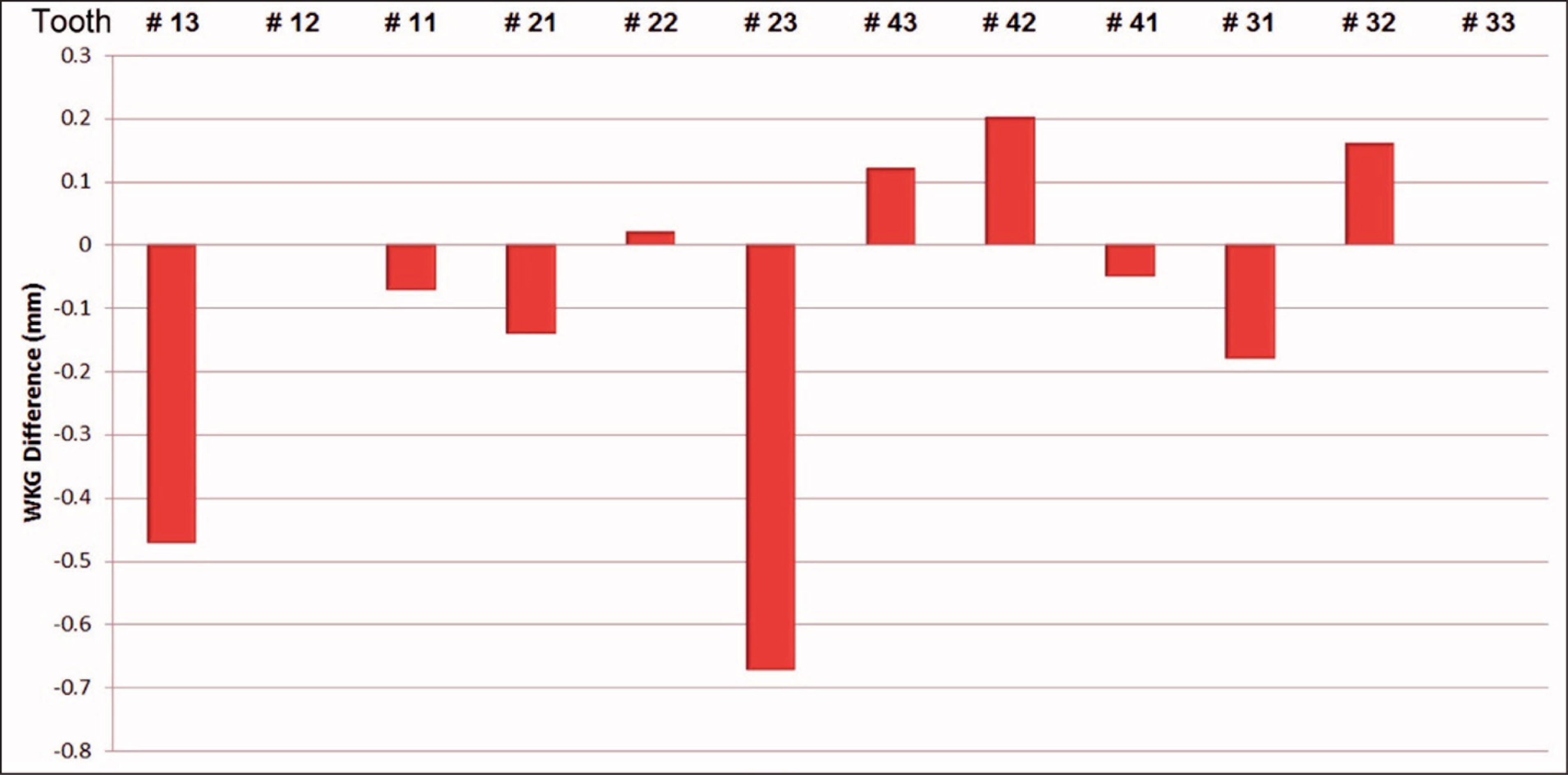
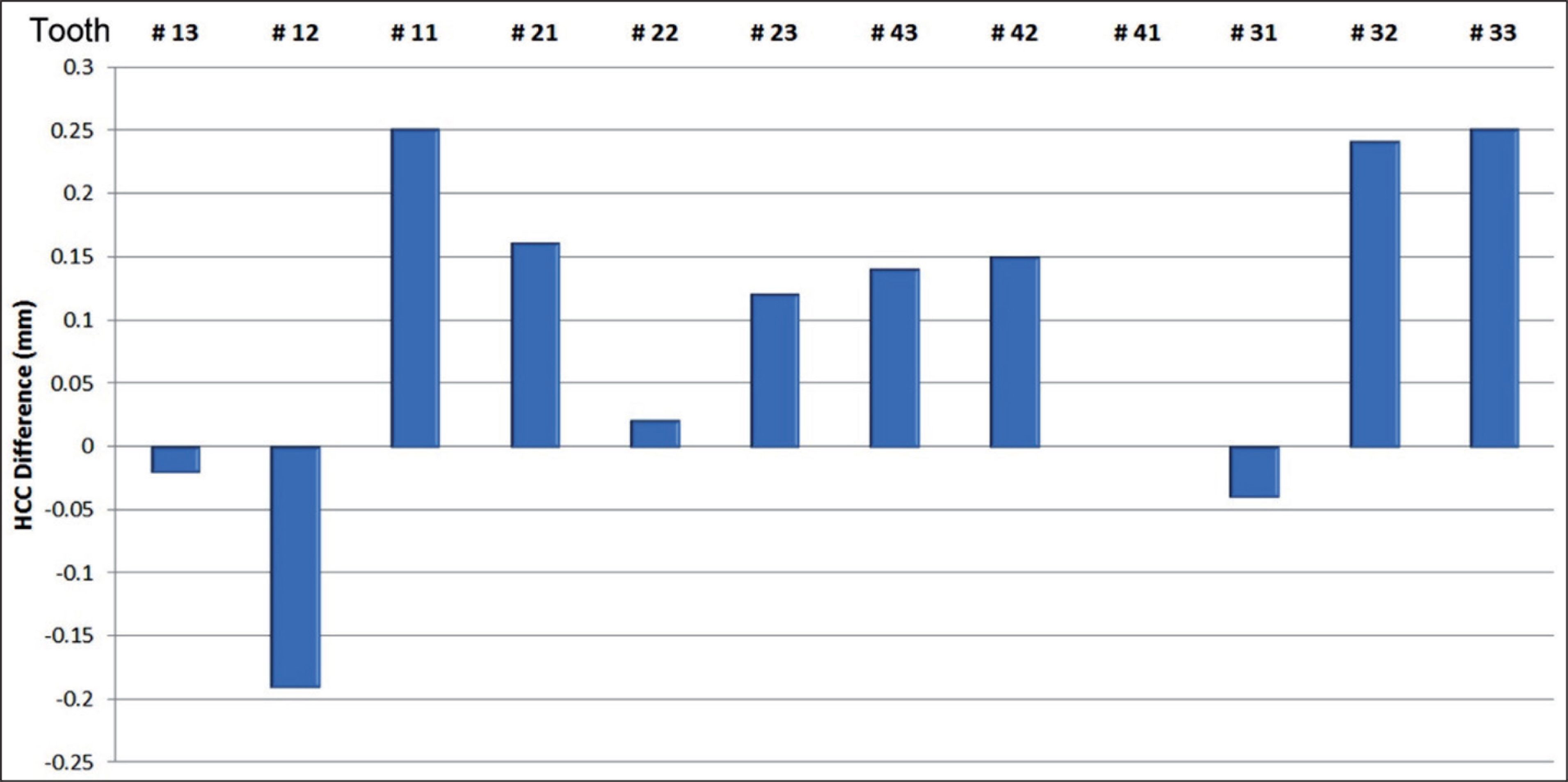
In order to assess the impact of orthodontic treatment on periodontium, the mean differences (i.e., differences between the values before and after treatment) were calculated for the width of keratinized gingiva, and clinical crown height, for upper and lower incisor teeth and canines (Table 3). The width of keratinized gingiva increased for most sites of upper teeth, particularly for upper left and right canines, by 0.47 and 0.67 mm, respectively (Figure 1). In contrast, the lower teeth showed a mix of improvement and compromised width of keratinized gingiva. As a measure of gingival recession, the difference of clinical crown height revealed the tendency toward a reduced clinical crown height (i.e., coronal migration of the gingival margin) for most sites (Figure 2). In some sites, only positive changes in both keratinized gingival width and clinical crown height were shown to be statistically significant (P < .05).
Descriptive Statistics for Mean Differences of the Width of Keratinized Gingiva and Clinical Crown Height Before and After Orthodontic Treatment

Mean Differences of the Width of Keratinized Gingiva (WKG) Before/After the Orthodontic Treatment for Upper and Lower Anterior Teeth
Mean Differences of the Height of Clinical Crown (HCC) Before/After the Orthodontic Treatment for Upper and Lower Anterior Teeth
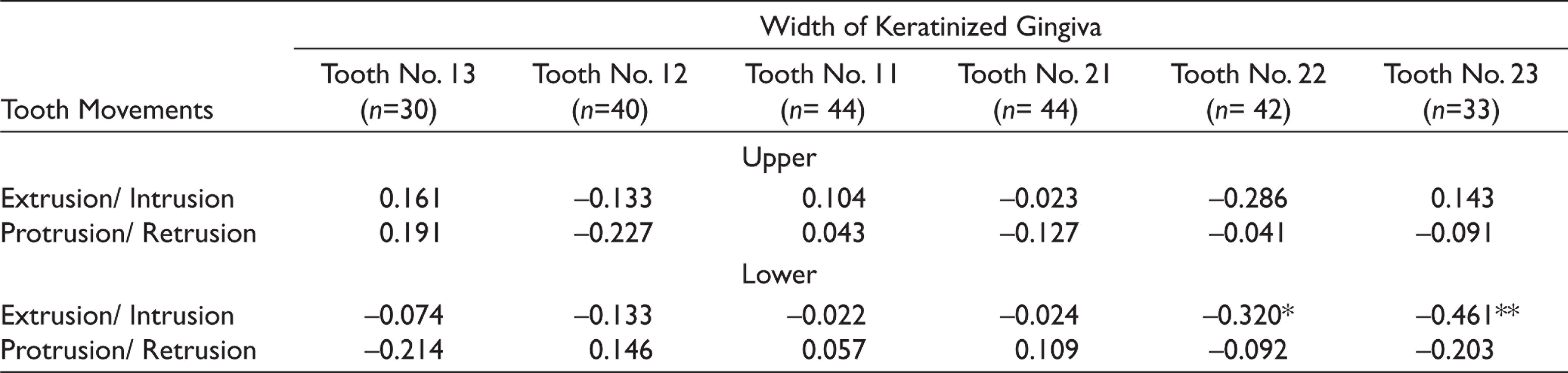
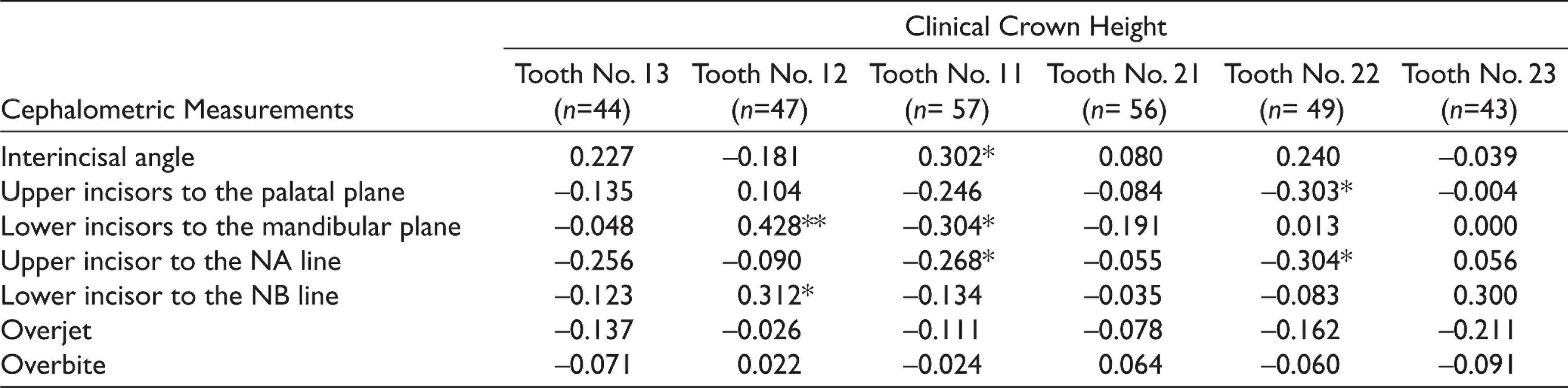
Mean differences of keratinized gingival width and clinical crown height were evaluated for any statistically significant correlations with other collected confounding factors such as the type of movement, pretreatment cephalometric values, and pretreatment overjet and overbite values (Tables 4 and 5). The upper left lateral incisors and canines showed significant values with regard to keratinized gingival width measurements and tooth movements such as extrusion and intrusion movements (Table 4). Likewise, with regard to the clinical crown height, the upper right central incisors showed significant differences when correlated with the interincisal angle, lower incisors to the mandibular plane, and upper incisors to the NA line. The upper lateral incisors also showed significant correlations to certain cephalometric measurements (Table 5).
Pearson’s Correlation Coefficient Between Width of Keratinized Gingiva and Different Types of Orthodontic Tooth Movement
Pearson’s Correlation Coefficient Between Clinical Crown Height and Different Types of Pretreatment Cephalometric Measurements
Discussion
Previous research has demonstrated a variable periodontal impact on different intraoral sites. The present study focused on the maxillary and mandibular anterior teeth. This decision was underpinned by the consideration that the bone surrounding these teeth is thinner and, therefore, may be more compromised than the bone surrounding the posterior dentition.
In the present study, the amount of keratinized gingiva increased by 0.46 mm as a sign of improvement. This finding is consistent with the results reported by Busschop et al., 31 who observed a comparable improvement at the upper canines site (0.57 mm). In contrast, the upper central and lateral incisors’ keratinized gingival width improvement observed in the present study was considerably lower than the one reported in the Busschop et al. 31 study (0.49 and 0.54 mm, respectively). Overall, the aforementioned improvement is well aligned with the research findings reported by Antoun et al., 32 who found that, in general, the controlled tooth movement has a positive impact on the periodontal supporting tissues.
Several other studies failed to replicate this pattern, showing instead the deteriorating periodontal effect after orthodontic treatment. For instance, Zachrisson and Alnaes found that the mean attachment loss in the patients wearing fixed appliances was higher, albeit insignificantly, than that in the control group (0.41 and 0.11 mm, respectively). 33 Obviously, this difference cannot be attributed solely to the orthodontic treatment per se. For instance, another factor that has previously been reported to increase during and after the orthodontic treatment with fixed orthodontic appliances is plaque accumulation. 6
In the present study, the width of keratinized gingiva of lower incisors showed a variable improvement and compromised response. This finding agrees with the results reported by Dorfman. 34 The variability of the keratinized gingival width outcomes for the lower anterior teeth can be related to the variable labial cortical bony plate thickness. In this respect, Choi et al. 35 found that lower incisors that are orthodontically proclined for the purpose of decompensation in Class III surgical cases could sustain some gingival recession and decrease in the height of alveolar bone.
There is a wide consensus that 2-mm-wide attached gingiva is adequate to withstand orthodontic forces and prevent gingival recession.36,37 Morris et al. reported the incidence of gingival recession to be 5.8% in teeth treated with fixed orthodontic appliances. 22 In the present study, the difference in clinical crown height decreased by 0.1 mm for the upper canines and by 0.2 mm for the upper central incisors. In a previous study of a total of 392 lower incisors, Ruf and coauthors 21 analyzed lateral head films, dental casts, and intraoral photographs with respect to the degree of orthodontic proclination, crown height, and gingival recession. Gingival condition was found to be unaf-fected or improved during the treatment in 380 teeth (97%), while gingival recession developed or was aggra-vated in 12 teeth (3%). The gingival recession in the latter 12 teeth was unpredictable and, in all probability, emerged because of the patients’ individual disposition and/or the presence of certain predisposing factors, such as the reduced thickness of the marginal gingiva, fenestrations, or bony dehiscence, as well as the quality of oral hygiene. Considering that the buccal bony root coverage on the central lower incisors is limited, these teeth are more susceptible to the development of gingival recession. 37
In the present study, according to the results of Pearson’s correlations, extrusion movements increased the width of keratinized gingiva in multiple sites. This result is largely congruent with many previous studies. For instance, many studies have demonstrated that, during supraeruption in the normal faciolingual position, the teeth tend to erupt with their investing tissues, thus possibly indicating a new means for increasing the width of a narrow zone of keratinized gingiva. 38 Furthermore, the results of several experimental studies on monkeys revealed that the free gingival zone moved by about 90% and the attached gingiva by about 80% of the extruded distance. The width of the attached gingiva and the clinical crown height increased significantly, while the position of the mucogingival junction remained unchanged. 39 Intrusion also showed a positive effect on the width of keratinized gingiva. Retrusion is one of the movements that improve the condition of the periodontium where it increases the amount of the width of keratinized gingiva. In the present study, in line with previous reports, protrusion movements showed a negative effect and a decrease in the amount of the width of keratinized gingiva.
The present study has several limitations. First, because we considered multiple cofounding factors, our results failed to clearly demonstrate a statistically significant association and differences. Furthermore, even though we performed the sample size calculation which showed that up to 0.8 mm of keratinized gingival width would be detected using 60 patients, the maximum mean difference observed in our results was 0.67 mm, indicating a possible lack of appropriate study power. Although some improvement sites were statistically significant, others were not. Therefore, in future studies, larger-scale samples would be needed to reliably detect potential consistent associations.
Conclusion
In this study, the orthodontic treatment was found to exert a significantly positive impact on the surrounding periodontium, particularly in the upper canine areas. Likewise, various types of tooth movement were found to positively affect the periodontium. However, a valid clinical trend could not be demonstrated. Therefore, further research with larger-scale samples would be needed for the detection of significant trends.
Footnotes
Acknowledgements
The authors gratefully acknowledge the valuable support of Doctors Al Ruwaithi, Al-Yousef, and Al-Eissa in the data collection phase.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.