
Abstract
The occlusal splint has been frequently used as an effective treatment in sleep bruxism patients. In the adjustment procedure of occlusal splint with an optimal occlusion, clinicians usually use conventional methods; however, they cannot measure the surface area of contacts, amount of force, and contacting time sequence. Recently, two separate technologies have been synchronized together: T-Scan III and BioEMG III. In the present case report, an occlusal splint in a patient with sleep bruxism was adjusted with synchronized T-Scan computerized digital occlusal analysis system and BioEMG III. Optimal occlusal parameters were generated, and quantitative analyses of occlusal scheme and muscle activity level were performed before and after the adjustment of the occlusal splint.
In the present case report, occlusion of the occlusal splint in a bruxism patient was adjusted with T-Scan III to fulfill the requirement of the optimal occlusion criteria. Before adjustment of occlusal splint, digital evaluation revealed unbalanced force distribution, lengthy occlusion (1.51 s), and disocclusion time (0.09 s) in centric relation. EMG activity of muscles was lower than expected values in centric relation. After adjustment of occlusal splint, canine protected occlusion with appropriate occlusion (0.2 s) and disocclusion (0.4 s) time were performed. Increased electromyography activity of the right anterior temporalis muscle showed a decrease in all excursive movements. Modern occlusal adjustment procedures provide a new standard of verification for the validation of occlusal splint fabrication with optimal occlusion.
Abbreviations
EMG: Electromyography
ICAGD: Immediate complete anterior guidance development
MM: Masseter muscle
TA: Temporalis anterior
TMJ: Temporomandibular joint
VAS: Visual Analog Scale
Introduction
Bruxism is defined as a “repetitive jaw-muscle activity characterized by clenching or grinding of the teeth and/or by bracing or thrusting of the mandible” with “two distinct circadian manifestations; either occurring during sleep (sleep bruxism) or wakefulness (awake bruxism)” 1
Although bruxism is not a life-threatening disorder, it can influence the quality of human life, especially through dental problems, such as tooth wear, frequent fractures of dental restorations, and pain in the orofacial region. 2 Masticatory muscle hyperactivity is a typical sign of bruxism and its mechanism have been explained previously by Okeson. 3
In order to reduce muscular hyperactivity, the occlusal splint has been frequently used as an effective treatment of sleep bruxism to protect teeth from damage caused by forceful jaw muscle contractions or to reduce orofacial pain. Most of the studies have examined changes in the masticatory muscles activity before and after application of an occlusal splint and they showed that occlusal splint treatment resulted in a decrease in nocturnal masticatory muscle activities in patients with bruxism.4,5 The reduced muscle activity also lessens the forces placed on the temporomandibular joint (TMJ) and other structures within the masticatory system. When these structures unloaded, the associated symptoms decreased. 5
In order to provide an occlusal splint with an optimal occlusion and an optimal force distribution, the following requirements should be performed. When the mouth closes, condyles seat musculoskeletally stable positions. In this position there is an even, bilateral posterior teeth contact and more lightly contact on anterior teeth than posterior teeth. All tooth contacts provide axial loading of occlusal forces. In all mandibular excursions, anterior teeth disclude all posterior teeth immediately. 6 In the adjustment procedure of occlusal splint, clinicians usually use conventional methods such as inked silk, articulating paper, or plastic. However, they cannot measure the surface area of contacts, amount of force, and contacting time sequence. They are not ideal occlusal analyzer due to their static nature and subjective interpretation. Moreover, current literature does not provide sufficient evidence of their reliability and reproducibility. 7 T-Scan occlusal analysis systems manufactured by Tekscan to overcome these limitations of qualitative assessment. The computerized occlusal analysis system records the sequence of occlusal contacts from the first point of contact to maximum intercuspation in real time. T-Scan system has the ability to quantify occlusal contacts timing and forces. 7 Recently, two separate technologies have been synchronized together: T-Scan III and BioEMG III (T-Scan/BioEMG linking software, Tekscan Inc/Bioresearch Associates technology partnership). They simultaneously record the changes in electromyographic activity (EMG) activity levels and occlusal contact force data with high definition. The simultaneous recordings allow clinicians to analyze and correlate specific occlusal contact with specific electromyographic changes that result from these occlusal contacts. 8
Kerstein et al. 9 were the first who measured tooth contact durations with the T-Scan I instrument and revealed that lengthy disclusion time (˃1.39 s) elevated levels of muscle contractions during excursive function and short disclusion time (˂0.4 s) dramatically reduce muscle contractions to near resting state. After that, they underwent a reduction of disclusion time with immediate complete anterior guidance development (ICAGD) procedure using T-Scan computerized occlusal analysis system. They reported the following occlusal parameters. (I); all teeth can occlude in ≤0.2 s, (II); all teeth can disclude in ≤0.4 s bilaterally and protrusion, (III); in maximum in maximum intercuspation, all teeth can contact bilateral force equality 50% ± 2%.
In the present case report, a sleep bruxism patient was treated with an occlusal splint, which was adjusted with synchronized T-Scan computerized digital occlusal analysis system and BioEMG III. Optimal occlusal parameters were performed following computer-guided occlusal adjustment. Measurable changes in occlusal scheme and muscle activity level was observed after adjustment of occlusal splints.
Case Presentation
A 13-year-old male patient visited the Faculty of Dentistry, Department of Prosthodontics clinic with a complaint of pain in the left masseter and TMJ region present from the past 1 year. Personal history revealed clenching of teeth during the night at least 3 days of a week. In clinical examination, patient had limited mouth opening (35 mm) and left masseter muscle (MM) pain on palpation with a VAS (Visual Analog Scale) score of 8. In examination of both of the TMJs, there is not any sound or pain. The diagnostic load test was accomplished without pain in either TMJs. Dental examination revealed parafunctional tooth wear. Based on anamnesis and clinical examination, the diagnosis of bruxism was given with no significant internal joint derangement. Impression of the upper and lower jaw was obtained with irreversible hydrocolloid impression material. A canine-guided occlusal splint was fabricated from self-cure clear acrylic resin that was described by Okeson 5 (Figure 1).
View of Canine Guided Occlusal Splint

Recording Devices
The computerized digital occlusal analysis was performed with T-Scan III (Software version 9.1, Tekscan Inc., South Boston, MA, USA). The appropriate size sensor and the holder are attached to the handle, which is connected to the computer. The recordings were made in Turbo mode. Sensor sensitivity adjustments were performed to fit the individual’s force level within the sensor’s responsiveness that only 3 or 4 red occlusal contacts were established.
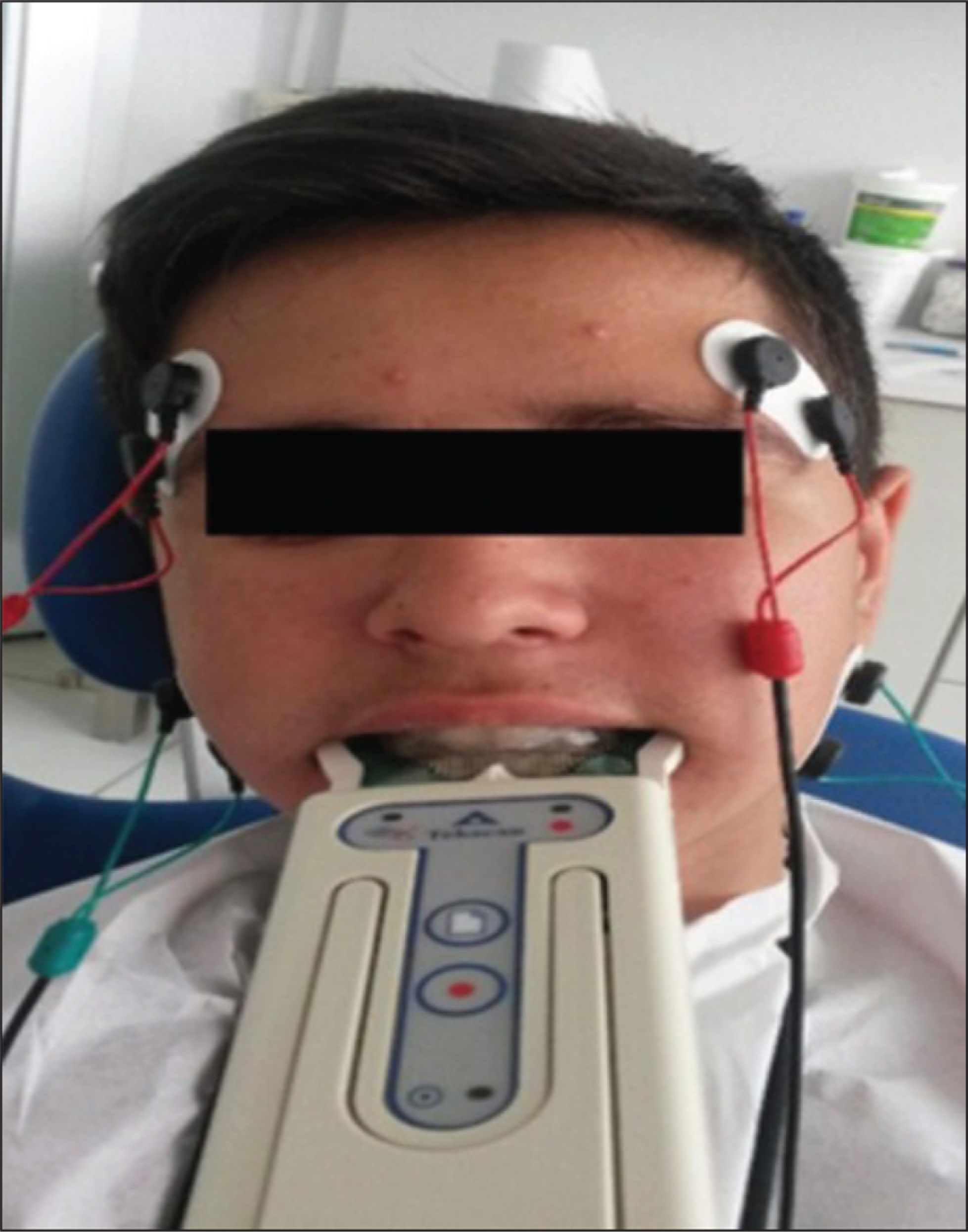
Electromyographic activity of masseter and anterior temporalis muscles were recorded with Bio EMG III (BioPAK, Bioresearch Associates Inc., Milwaukee, WI, USA). Before recordings, the patient’s skin was cleansed with alcohol. Self-adhesive bipolar EMG electrodes (Bioflex, Bioresearch Associates, Inc., Milwaukee, WI, USA) were placed bilaterally over the bodies of the superficial masseter and the anterior temporalis muscles and positioned parallel to the direction of muscle fibers. The reference ground electrode was placed on the neck. All EMG data were recorded through a Bio EMG III amplifier and the BIOPAK computer program.
Recording Procedure
Before the adjustment of the occlusal splint, simultaneous digital computerized occlusal analysis and the EMG activity of masseter and anterior temporalis muscles were performed in centric relation, and all lateral excursive movements (right, left, and protrusive excursive movements) (Figure 2). In centric relation, the patient repeats three clenches on their posterior teeth for 1–3 s, and the occlusion and the electromyographic activities of muscles were analyzed (Figure 3). In all excursive movements, the patient occluded in maximum intercuspal position for a period of 1–3 s, and then commenced the right, the left, or protrusive excursions.
View of Simultaneous T-Scan and BioEMG III Recordings
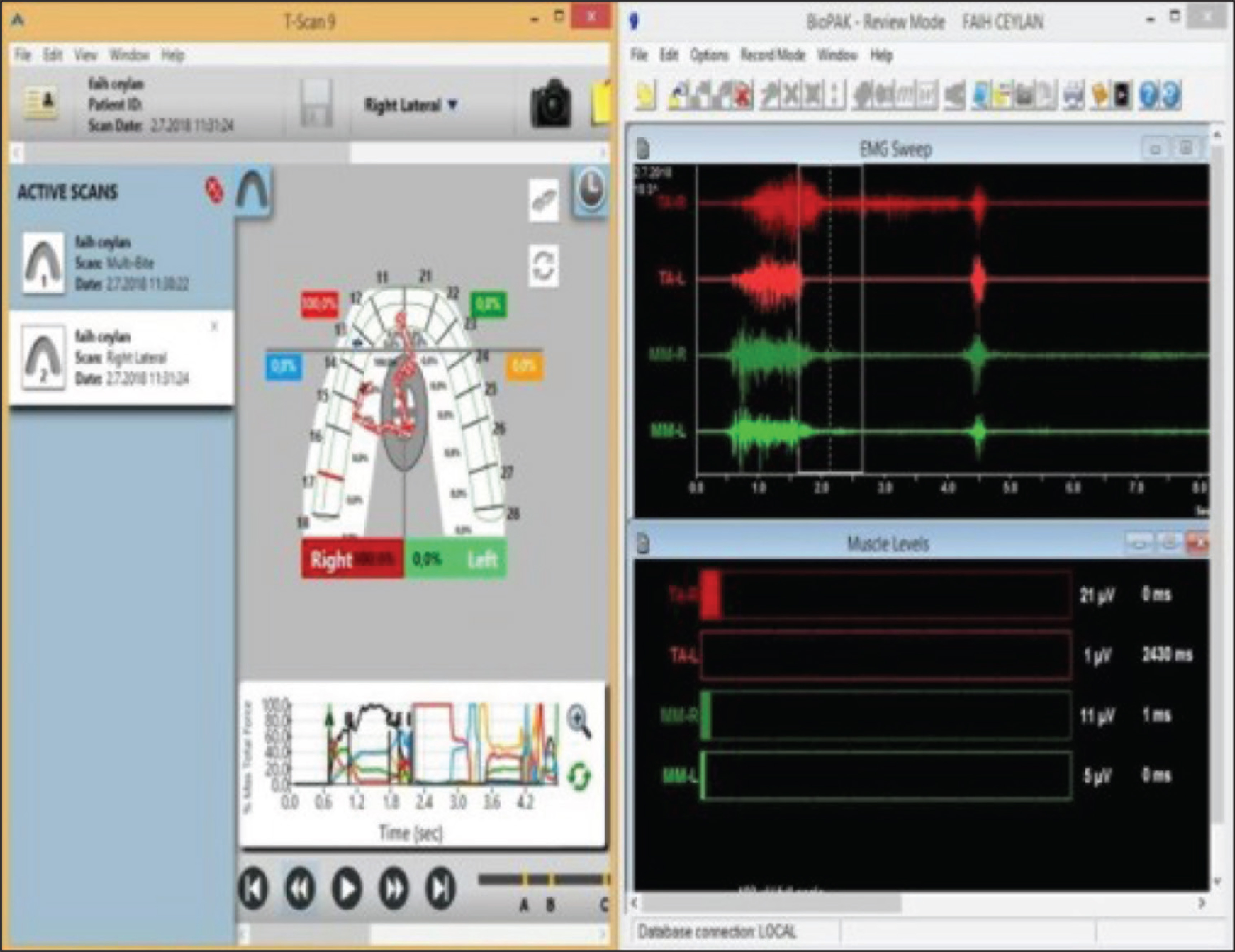
Simultaneous T-Scan and Bio EMG recordings
The occlusion of splint was adjusted with T-Scan III to fulfill the requirement of the optimal occlusion criteria. The occlusion was checked in both supine and upright positions so that any change in jaw posture does not create an uncomfortable contact. Occlusal contacts were checked both during patient self-closure and centric relation closure with the bimanual guidance for the optimal occlusal contacts. In centric relation, even tooth contacts on both sides and harder posterior tooth contact than anterior were generated. In all lateral excursions only the canine guidance contacts with occlusal splint with no posterior teeth contact. The canine contact was smooth, continuous line and the patient slid from medial to lateral and lateral to medial on this line without any “hitches” or “jerky movement.” After all the contacts of occlusal splint were perfected, simultaneously computerized occlusal analysis and the EMG activity of masseter and the anterior temporalis muscles were repeated in centric relation, left lateral, right lateral, and protrusive movements, respectively. In all excursive movements, the patient occluded in the maximum intercuspal position for a period of 1–3 s and then commenced the right, left, or the protrusive excursions until only canine were in contact.
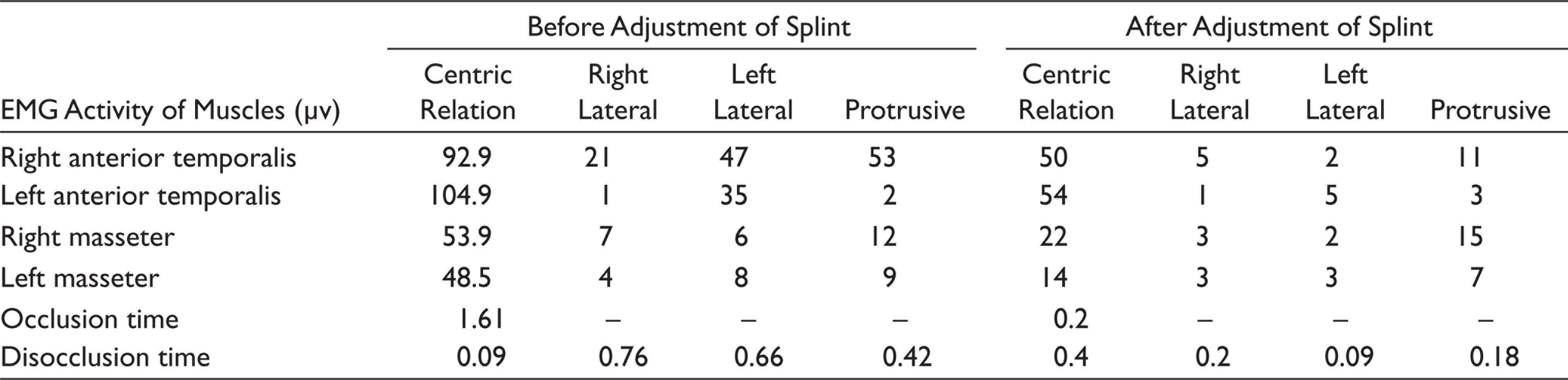
Before the adjustment of the occlusal splint, the digital evaluation revealed that in the maximum intercuspal position the force of distribution was %40.8 for the right side and %59.2 for the left side. And the patient had lengthy occlusion (1.51 s) and disocclusion time (0.09 s) in centric relation. EMG activity of muscles was lower than expected values (Table 1) in centric relation. Patient had canine guided occlusion in right lateral movements and group functional occlusion in left lateral movements with increased disocclusion time. Obviously, it has been detected that the right anterior temporalis muscle showed the increased activity in all excursive movements.
After adjustment of occlusal splint in centric relation even simultaneous contact with no premature contact was performed with appropriate occlusion (0.2 s) and disocclusion (0.4 s) time. Left and right force distribution was %50.1 and %49.9, respectively. In centric relation occlusion with the occlusal splint, heavier posterior teeth contacts were performed than anterior teeth on both the left and right sides. EMG activity of all recorded muscles showed a decrease (Table 1). In all excursive movements, occlusal splint occluded only the canine teeth, and the decreased disocclusion time was performed. After the adjustment of the occlusal splint, increased EMG activity of the right anterior temporalis muscle showed a decrease in all excursive movements.
Electromyographic Activity of Muscles Before and After Adjustment of Occlusal Splint in Centric Relation
Discussion
Before the adjustment of the occlusal splint, pain-side muscles indicated subnormal EMG activity in the clenching. The concept of the relationship between pain and sleep bruxism have been explained and sleep bruxism patient without painful symptoms have higher EMG activity compared to the bruxism patient with pain.10,11 Furthermore, Rompre et al. 12 concluded that sleep bruxism patients with craniofacial pain show the low frequency of the EMG activity.
In the present case report, before the adjustment of the splint in all excursive movements patient had the decreased masseter and temporalis anterior (TA) muscle EMG activity in the pain side and the increased EMG activity of the temporalis anterior muscle in the non-pain-side that could be related to the “pain adaptation model.” Previously, it has been shown in several clinical studies and in experimental muscle pain studies 13 that a decrease of the EMG activity in the painful muscle and an increase in the EMG activity in nonpainful muscles was found during the dynamic contractions. 14 Lund et al. 15 have described the interaction between the muscle pain and muscle coordination with the “pain-adaptation model” that lead to the increased activity of antagonistic muscle and the decreased activity of agonistic muscle during muscle pain. The changes in muscle activity and coordination will cause a reduction of movements, which is likely to serve as a protection of the painful muscle.
In addition to the beneficial protective effect of splints on the dentition, occlusal splints reduce nocturnal jaw muscle activity, and craniofacial pain. 12 Occlusal splint therapy can lead to a reduction in fatigue of the masticatory muscles, as demonstrated in a study by Zhang et al., 16 who found decreased EMG activity in the masticatory muscles following occlusal splint therapy as that found in the present study.
Before adjustment of an occlusal splint, the patient had unbalanced bilateral tooth contact in natural dentition (%40.9 and %59.1 in right and left side, respectively) with prolonged occlusion time (1.51 s). Occlusal interferences strongly have been correlated with temporomandibular disorders (TMD) with bruxism, which are retruded condylar position to intercuspal position slide, balancing–working side, and protrusive interferences.17,18 These occlusal interferences lead to orthopedic instability of TMJ and hyperactivity of muscles eventually lead to TMD. 19 Therefore, to eliminate the effect of natural dentition on bruxism, even bilateral posterior teeth markings were achieved by occlusal splint with decreased (˂0.2 s) occlusion time. After the adjustment procedure of occlusal splints, occlusal force distribution between the right and left side were balanced, and lighter anterior teeth contacts than posterior teeth were performed with the decreased occlusion and disocclusion time. EMG recordings with optimized occlusal contacts of splint in centric relation revealed a decrease in EMG activities of all recorded muscles.
On the other hand, Kerstein and Wright were the first who proposed that some TMD patients including bruxists could be treated by reducing the disocclusion time. 9 Their study showed a direct correlation between the contractile muscle activity and disocclusion time that lengthy of disocclusion time leads to an excessive muscle activity. They describe an “immediate complete anterior guidance development” technique for the occlusal adjustment procedure and post-treatment EMG, and T-Scan computer analyses revealed that shortening the disocclusion times less than 0.4 s in any lateral excursions lessened the excessive muscle activity to near resting-state values. 20 In the present study, ICAGD developed with the canine guidance of occlusal splint rather than nonreversible occlusal adjustment procedure, and the disocclusion time reduced to ˂0.4 s with this guidance. The pretreatment level of excursive muscle hyperactivity of the right anterior temporalis muscles was lessened and reached to near resting state. This reduction caused by the decreased occlusal contact time during excursive movements results in a decreased time of periodontal ligament compression. So that reduced duration of compressions does not add extra muscle activity and directly result in muscle activity level reduction in the masseter and anterior temporalis muscles.
As a limitation of the present case, the used protocol in the adjustment of occlusal splint has been described for one case without a follow-up visit. Further clinical studies with more patients and follow-up can be performed to entirely evaluate the described protocol. Although the use of T-scan technology in adjustment of the occlusal splint increases the cost and time, because of the advantage of technology the routine use of T-scan IIII in adjustment of occlusal splint should be investigated in future studies.
Conclusion
The present case report describes the adjustment of an occlusal splint in a patient with sleep bruxism with a modern occlusal adjustment procedure. This technology provides a new standard of verification for the validation of occlusal splint fabrication with the optimal occlusion verifying the occlusion of splint leads to predictable treatment results. In addition, T-Scan improves the ability to diagnose of existing occlusion and to create an optimal occlusion.
Footnotes
Author Contributions
Patient was examined by EDD and DK. Then, the treatment was planned by EDD and DK. The adjustment of the occlusal splint was performed by ED. Present study was written by DK.
Data Availability Statement
The data supporting the findings of this case study are available in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Declaration of Consent
Patient and the parents were informed about this case study and written parental consent was taken prior to treatment.