
Abstract
Aim:
To develop a simple approach to estimate quality-adjusted tooth years of teeth (QATY) treated for periodontitis and determine gains in QATY after undergoing cause-related periodontal therapy (CRPT). Quality-adjusted life years (QALY) gained for these patients were also determined.
Materials and Methods:
Patients newly diagnosed with periodontitis (n = 165, 58.8% females, mean age 43.3 years) were recruited from periodontal specialist clinics. They received CRPT within a period of one year. We used the EuroQoL 5 Dimension (EQ-5D) and the Malaysian Oral Health Impact Profile (OHIP-14) indexes to measure changes in quality-of-life after one year of periodontal treatment. We then used these two scores to calculate their respective utilities and subsequently calculated QALY and QATY.
Results:
Proportions of deep periodontal sites (≥ 4 mm) decreased from 32.7% to 23.2% and patients gained an average of 0.3 mm of clinical attachment level per tooth at post-treatment follow-up. Improvements in means of OHIP-14 scores from 20.30 to 12.7 were consistent with changes in EQ-5D utilities from 0.81 to 0.91. Treated teeth gained 20.4 years for longevity while patients gained 17 QATYs. This is in line with the increase of 3.8 QALYs. Both treatment outcomes and clinical parameters were statistically significant at P < .0001.
Conclusions:
The method of estimating QATY using utilities derived from OHIP-14 combined with tooth life expectancy demonstrated that it may be used to measure effective treatment outcomes and is found to be consistent with improvements in QALY scores as calculated using EQ-5D-3L.
Keywords
Abbreviations
MT: Marc Tennant
RA: Rasidah Ayob
SEWP: Sharifah Ezzat Wan Puteh
SMA: Syed Mohamed Aljunid
TMD: Tuti Mohd-Dom
Introduction
Periodontal disease is recognised as a major public health problem because of its widespread prevalence, quality-of-life (QOL) impacts on its sufferers and burdens on healthcare systems.1–4 The rapid advent of advanced technologies in clinical dentistry provides henceforth a range of treatment options and policy-makers would require evidence-based economic evaluations to assist in resource allocation decision-making across diseases, programmes and treatment modalities. Many clinical studies have reported successful outcomes of periodontal therapy, which are demonstrated as improvements in clinical parameters5–7 as well as oral health-related quality of life.8,9 However, most studies report these treatment outcomes as separate entities and do not capture patient experiences holistically using both qualitative and quantitative indicators.
In measuring clinical effectiveness for instance, the ultimate endpoint is ideally determined by the longevity of the periodontally affected tooth after it has undergone treatment. This would be determined by the number of years the tooth is expected to survive throughout the patient’s lifetime—the tooth life expectancy (TLE). The shortfall of this indicator is that while it predicts the quantity of tooth years after treatment, it gives no indication of the ‘quality’ of the tooth—whether one is able to chew well with it, is there any sensitivity or problems with its aesthetics—the tooth utility. It was almost three decades ago, that Birch (1986) first highlighted the deficiencies of a decayed and restored tooth in a way that it will not match qualities of a healthy one. 10 His early work was related to improving index for measuring dental caries experience where he described quality-adjusted tooth years (QATY) as ‘additional years of life of a tooth adjusted for its quality’. 10 This had been adapted from the concept of ‘utilities’, which refer to a measure of an individual’s well-being or preferences for outcomes. 11
‘Dental health state utility values’ have been explored using time-tested methods such as time trade-off (TTO) and standard gamble (SG) —methods that requires some sacrifice or trade-off to be made by the patient.10–17 For example, in the TTO method, a patient with a painful tooth is asked whether he would be willing to extract the tooth to avoid living with pain and discomfort. In the SG method, this same patient is offered the hypothetical choice between the sure outcome, A (live with the pain but keep the natural tooth), and the gamble, B. The gamble has a probability P of the best possible outcome after say, a root canal treatment, (optimal health and function, defined as 1) and a probability (1 – P) of the worst possible outcome (such as worsening of pain and requires extraction, defined as 0).
Similarly, in periodontal therapy, the life expectancy of periodontally treated teeth needs to take into consideration side-effects of the treatment or the disease itself because the quality of a treated tooth will not be as good as a healthy tooth. QATY as a critical consideration in determining periodontal treatment outcomes was not long after Birch’s conceptualisation of the idea demonstrated by works of Antczak-Bouckoms and Weinstein. 12 Unfortunately, there was no continuity of its application in the clinical setting. One reason may be attributed to the extensive work required to establish ‘utilities’ scores of the different periodontal conditions and the subjective method employed to estimate the TLE.
This concept of QATY had been adapted from the more established concept of quality-adjusted life years (QALY), which is a generic measure of disease burden which combines both the quality and the quantity of life lived. 18 It is used in economic evaluation to assess the value of medical interventions and can be used by patients to make personal decisions, and for policymakers to evaluate programmes and to set priorities for future programmes. Its use in clinical periodontology is worth pursuing. Interestingly, QALY as an outcome measure has not been used in dentistry in spite of oral health being recognised as an integral part of one’s overall health. Like QALY, QATY is derived by combining dental utilities with estimated TLE in a single metric. Its use in the clinical dental setting will provide deeper insight on consequences of the dental treatment from both clinician and patient perspectives. Its potential use to compare outcomes across all dental treatment outcomes may serve as a useful basis for economic evaluation and resource allocation in dental services.
An attempt to develop a utility index for deriving QALY from an oral health related quality of life index has been made by Brennan and Spencer in 2006 by mapping out the Oral Health Impact Profile (OHIP), an oral health measure, to a generic health state measure—the EuroQol (EQ-5D). 19 OHIP is a well-established quality of life index that has been used to measure patient-reported outcomes of dental care with regards to impacts of the oral condition on the patients. 20 Improvements after treatment will be reflected as reduction in OHIP scores. As for EQ-5D, it is a generic health-related quality of life index, which will reflect increase in scores when quality of life improves. 21 However, the algorithm developed for the transformation of OHIP scores into EQ-5D utilities in that study has yet to be tested for use in any specific oral condition.
The purpose of this study was to develop a simple approach to estimate QATY of teeth treated for periodontitis using established QOL instruments as measures of utilities. The product of the multiplication of these utility values with TLE was used to illustrate and estimate the quantum of QATY gained after patients receive periodontal therapy.
Materials and Methods
Setting and Design
This was a quasiexperimental health service research conducted at periodontal specialist clinics within the purview of the Ministry of Health, Malaysia. Patients who were newly diagnosed with chronic periodontitis were recruited and received cause-related periodontal therapy (CRPT) within a period of one year. CRPT included supra- and sub-gingival debridement, oral hygiene instruction, restorations, root canal therapy and dentures. Two instruments namely the EQ-5D-3L and OHIP-14 were used to score changes in QOL after one year of periodontal treatment. Utilities derived from these two scores were used to determine changes in QALY and QATY.
Sampling and Data Collection
Study participants were recruited from the pool of chronic periodontitis patients who had been referred to five selected specialist clinics in the Ministry of Health, Malaysia, over a period of eight months. Screening of patients using the Basic Periodontal Examination (BPE) were done at the referring primary dental clinic and patients must have scored at least 4 mm probing pocket depth (PPD) at any one sextant. To be included in the study, they must be older than 18 years old, attending these specialist clinics for the first time, have not had any periodontal treatment done at least six months prior to the study and were not pregnant.
Periodontal Assessments
Full-mouth periodontal assessments of the patients were conducted by periodontists based at their respective dental clinics. They examined all hard and soft tissues in the oral cavity per standard routine clinical examination using standardised charting and assessment protocols. Periodontal examinations included the following clinical parameters: probing pocket depths (PPD), gingival recession, clinical attachment levels (CALs), plaque levels and presence of bleeding on probing (gingivitis). These measurements were completed at baseline and at follow-up visits after the CRPT is done, on all teeth present and with probing at six sites per tooth. Diagnosis of chronic periodontitis was made according to the classification of the American Academia of Periodontology. 22
Quality of Life Outcomes
Two instruments were used to measure patient-reported outcomes after CRPT:
The EuroQoL-5D instrument is a generic health-related quality of life measure with the three-level version (EQ-5D-3L) consisting of the EQ-5D descriptive system and the EQ visual analogue scale (EQ-VAS).
21
Permission to use it was granted by EuroQoL. The EQ-5D-3L descriptive system comprises five dimensions, namely mobility, self-care, usual activities, pain/discomfort and anxiety/depression. EQ-VAS on the other hand records the respondents’ self-rated health on a vertical, visual analogue scale where the endpoints are labelled ‘best imaginable health state’ and ‘worst imaginable health state’. OHIP-14 (Oral Health Impact Profile-14) is an oral health-related quality of life measure comprising 14 questions addressing the following dimensions: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability and handicap. Each item was scored using a five-item Likert scale and scores were added up as a range from 0 to 56. The instrument was developed by Slade and Spencer
20
and validated in the Malay language for use among Malaysian adults for both its original version as well as the short-form version.23,24
A global rating to assess changes in patients’ perception and satisfaction with general and oral health was also included to obtain an overall view of patients’ self-awareness of their own conditions All study respondents were interviewed face-to-face by trained assistants. A pilot study was undertaken at a university dental clinic setting prior to actual execution of study.
Calculation of Quality-Adjusted Life Years
QALY is calculated by multiplying the utility values by life expectancy of the patients according to life tables of Malaysians, by age and gender. 25 Utility values measured using EQ-5D had been derived by using time trade-off value sets for Thailand provided by EuroQol official group for the corresponding health states. 26
Calculation of Quality-Adjusted Tooth Years
QATY is calculated by calculating the utility values and multiplying it by TLE.
The conversion of dental health state utility scores was done based on the OHIP-14 score and done according to the following steps:
Obtain OHIP-14 scores at baseline and 12 months after treatment. Establish correlations within OHIP domains to ensure there were no dominant domains causing the impacts of periodontitis on the patients. Pearson’s correlation analysis found all OHIP-dimensions correlated very well (over 70%) with the total scores indicating no dominance of any specific domains. Convert OHIP-14 scores (which had a range of 0–56) to utilities (with a range of 0–1). This is first done by mapping the value of 0–56 into 0–1. As the value of ‘0’ for OHIP-14 is the best state imaginable (no oral health-related QOL impacts) its value needs to be reversed. Similarly, the highest score for OHIP-14 is 56, which signifies the worst state imaginable (maximum score for impacts), this too needs to be reversed. Hence, y is calculated as (1 – x/56). For example, if a patient scores 14 on the OHIP-14 scale, then the utility score, y is calculated as (1 – 0.25) = 0.75.
In the absence of actual data on TLE, we had made an assumption based on a method proposed by Kay et al., 27 which hypothesised that tooth survival follows a simple declining exponential function and a constant annual tooth mortality rate (ATMR). According to this approach, TLE is expressed as the reciprocal of the tooth loss rate. Hence, TLE of teeth treated for periodontitis was estimated from secondary data of an ATMR of 0.03/patient/year, 28 which corresponds with the reciprocal value of 33.3 years. This means that teeth that have been periodontally treated will have a TLE of 33.3 years. As for periodontally affected teeth that are not treated, the estimated TLE is 4.5 years—this is estimated from the same study using the value of 0.22/patient/year as reported for noncompliant patients. 23
Statistical Analysis
Data analyses were performed using the statistical software package IBM-SPSS 20.0. 29 Normality (Kolmogorov–Smirnoff test) and homoscedasticity (Levene’s test) of both patient-reported and therapeutic outcomes appeared to be valid. Hence, changes in QOL measures and clinical parameters after CRPT were analysed using paired t-test (for changes in means) and McNemar’s test (for changes in proportions), with a significance level set as α < 0.05. Only 134 (79.4%) patients completed CRPT and attended the end of 12-month recall visit, hence analyses related to treatment outcomes were done using intention-to-treat analysis, with the last observation carried forward.
Results
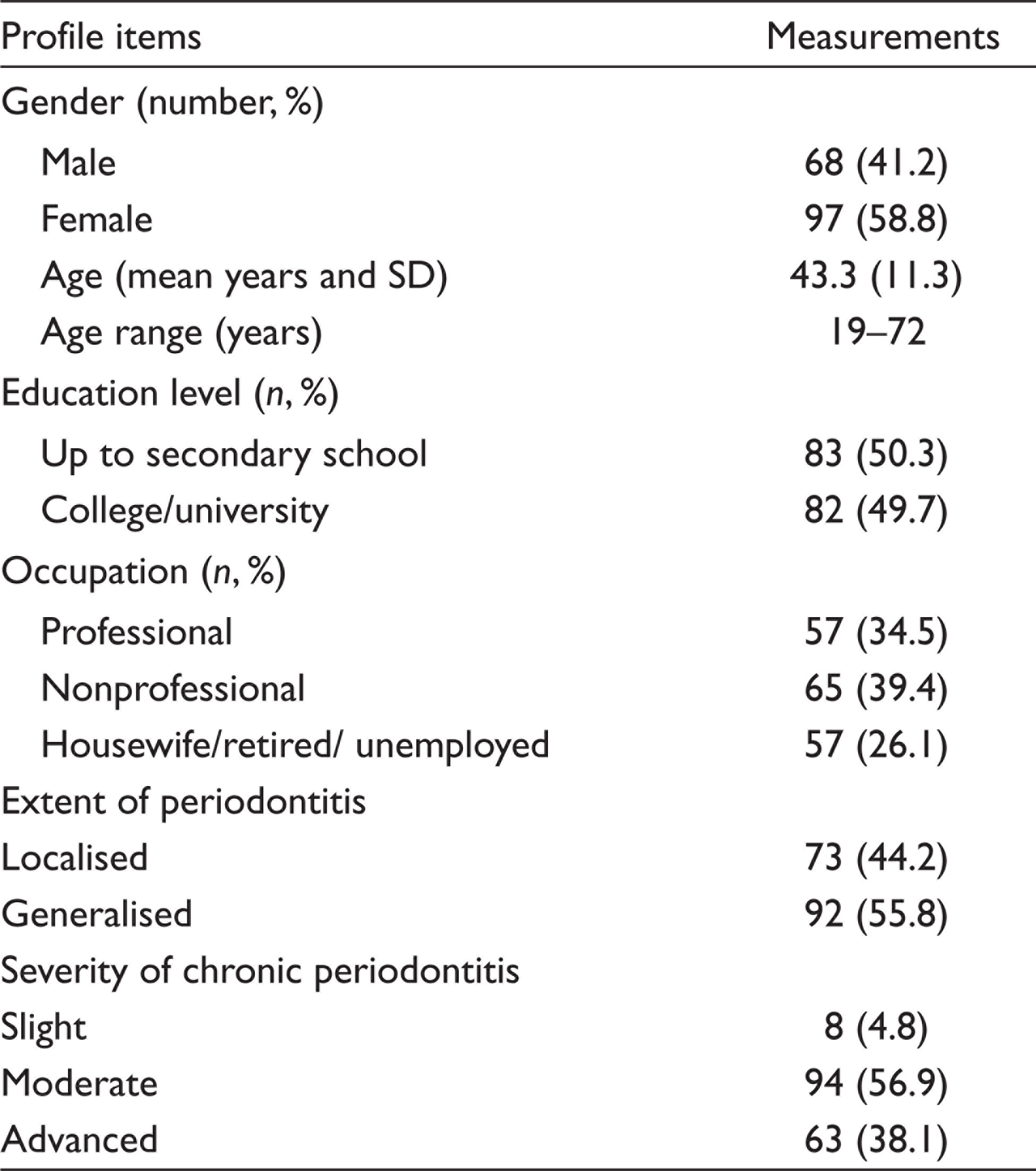
Table 1 describes background characteristics of the sample cohort. About 60% of these patients were females and about half studied at least up to secondary school. Only about one-third worked as professionals, while the others either had nonprofessional occupations or were unemployed. With regard to the extent and severity of periodontitis, there was a balance between patients with localised and generalised chronic periodontitis, while majority had moderate periodontitis.
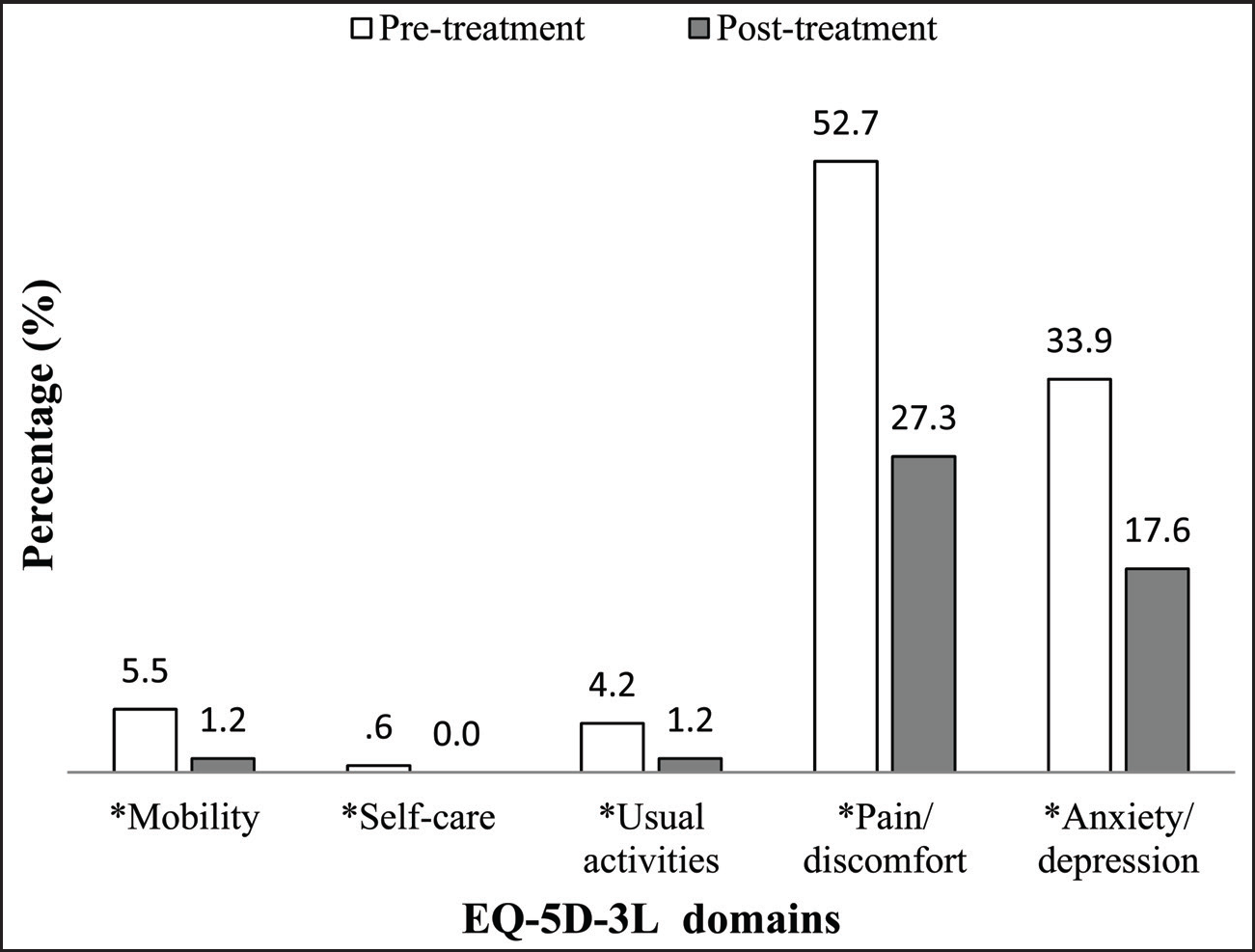
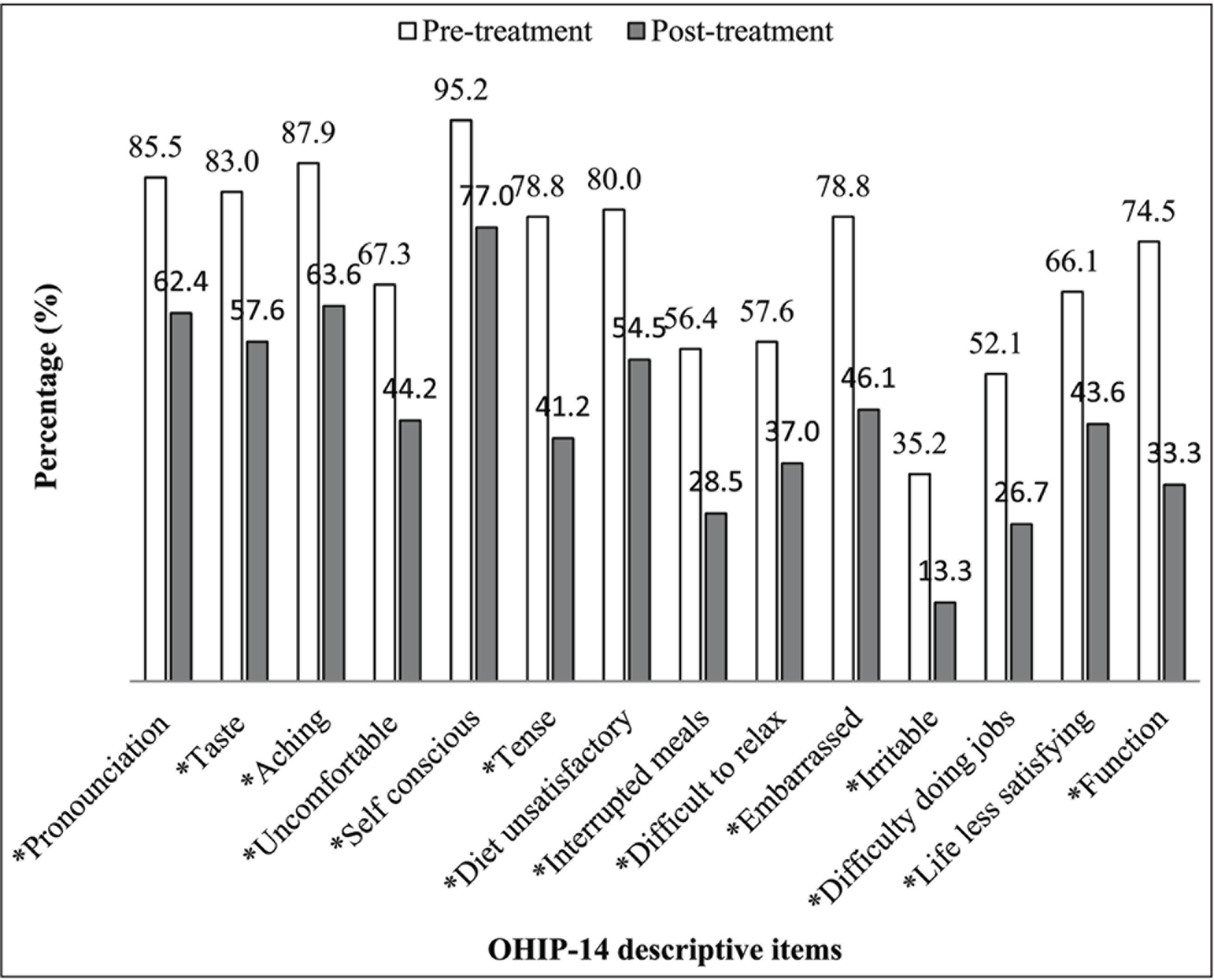
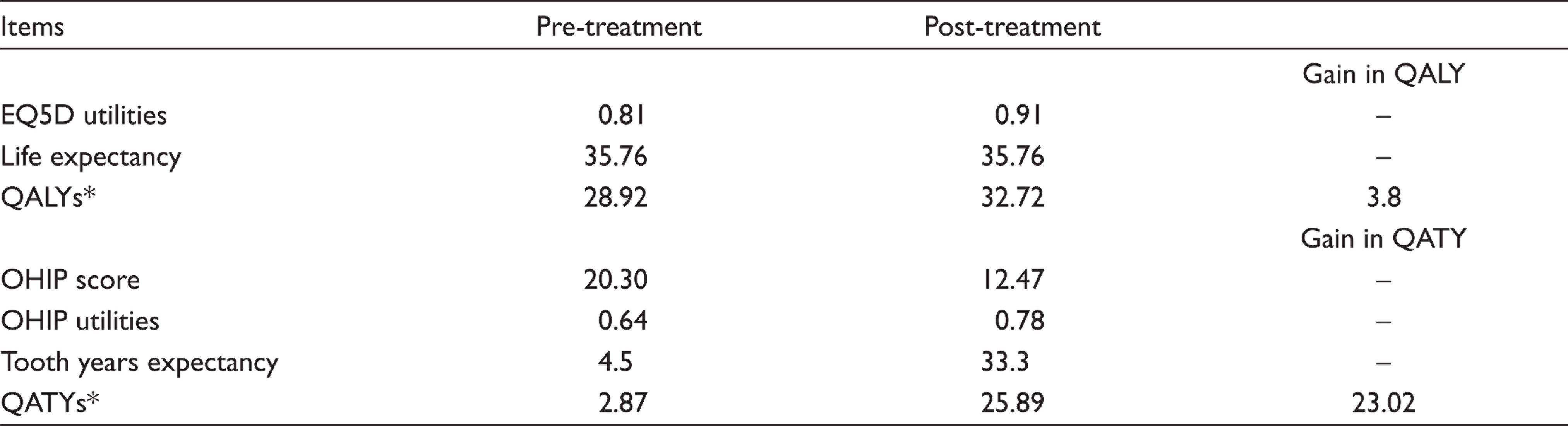
CRPT resulted in statistically significant improvements in clinical and quality of life measures (P < .0001) (Table 2, Figures 1 and 2). Table 2 illustrates reduced percentages for plaque and bleeding scores suggesting reduced disease activity, as well as reductions in PPDs and CAL suggesting gains of attachment and healing had taken place. Figure 1 illustrates significant reductions of pain/discomfort and anxiety/depression after one year of periodontal therapy. In Figure 2, the greatest improvements were observed for items related to going out, being confident and smiling; patients reporting affected by these items reduced by at least half (50%–62%) in their respective proportions. In addition, EQ5D utilities scores improved significantly, contributing to an average increase of 3.8 QALYs post-treatment (Table 3). Utilities converted from OHIP-14 also increased significantly, contributing to an average gain of 23 QATYs (Table 3).
Characteristics of Sample Cohort (Total n = 165).
Periodontal Parameters, Pre- and Post-treatment.

Improvement in EQ-5D-3L Descriptive Items, Pre- and Post-treatment Level of Significance (α = 0.05, *McNemar’s test).
Improvement in OHIP-14 Descriptive Items, Pre- and Post-treatment Level of Significance (α = 0.05, *McNemar’s Test).
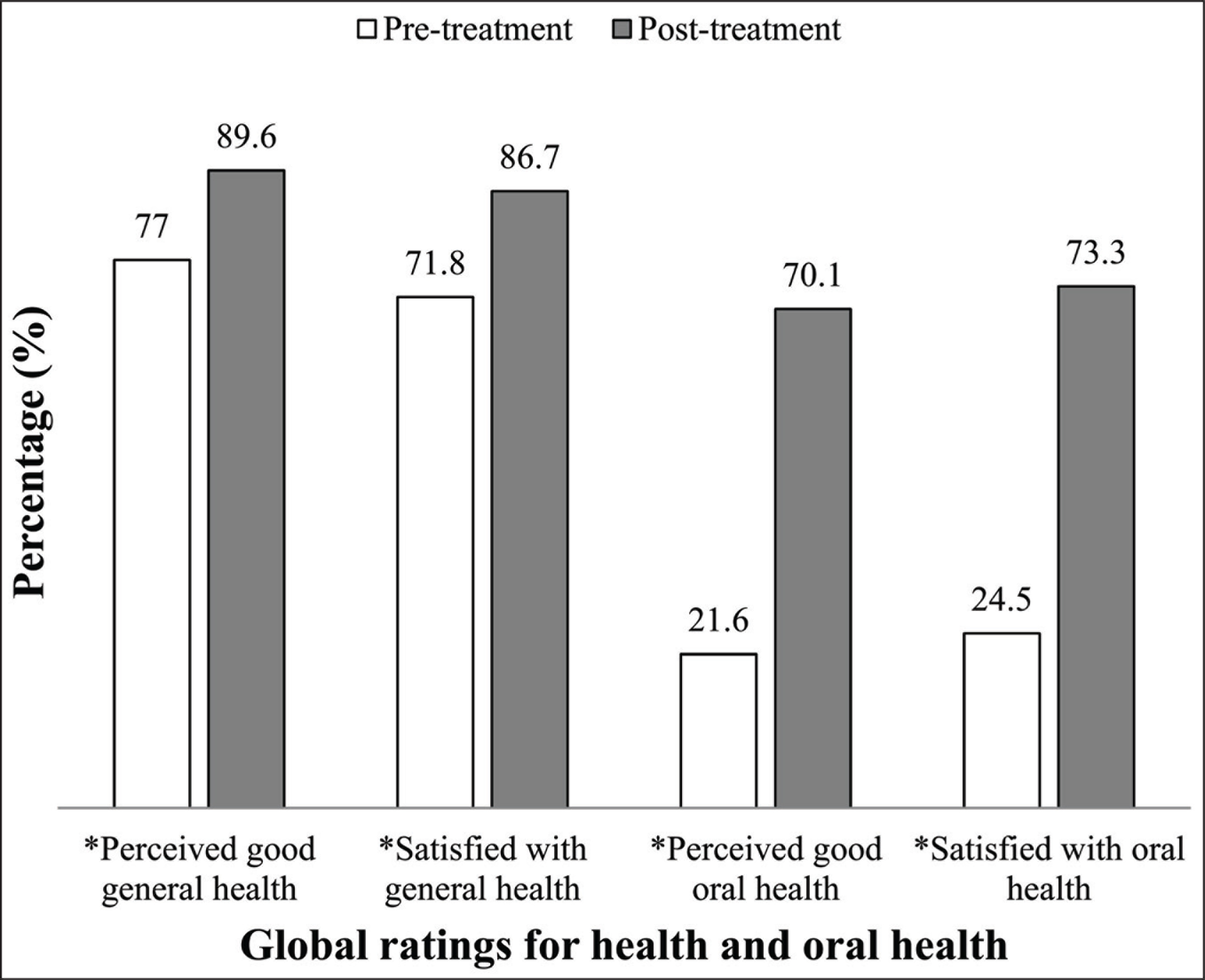
In terms of global ratings of general and oral health, proportions of patients who were positive about their general and oral health improved significantly (Figure 3). Higher gains of perceived health status and satisfaction were observed for oral health (40%) ratings compared to general health (10%) and these observations were consistent with changes in OHIP-14 and EQ-5D scores.
Quality-Adjusted Life Year (QALY) and Quality-Adjusted Tooth Year (QATY), Pre- and Post-treatment.
Perception and Satisfaction with General and Oral Health Status, Pre- and Post-treatment.
Discussion
The rapid advent of advanced technologies in periodontal therapy has given rise to the need for healthcare providers and patients to be more objectively selective about treatment options. A chosen therapy must not only improve the clinical outcomes but also improves patients’ quality of life (QOL). A measurement that combines both the quality and quantity of years (QALY) or tooth-years (QATY) in a single unit would then be highly desirable. In the absence of practical methods to utilise QATY as an outcome measure in the clinical setting, this study developed a simple approach toward this end by using an established instrument QOL, namely the OHIP-14, to estimate the measures of utilities for periodontitis. We then combined these utility values with estimated TLE after periodontal treatment to measure gain in QATY as an outcome measure.
Measurements of dental health state utility values have been explored for conditions such as dental caries,10,12 periodontal disease,13,14 tooth loss, 15 endodontics 16 and dentofacial deformities. 17 Consistently these studies had employed time-tested methods such as TTO and SG—methods that are consistent with the utility concept that requires some sacrifice or trade-off to be made by the patient. 30 For example, in the TTO method, a patient shall be asked to choose between his remaining life expectancy in the state ‘alive, bed-ridden’ and a shorter life span but able to walk. Another method is use of scaling method such as Visual Analog Scale to measure disutilities of tooth loss. 31 Estimating utilities from a QOL instrument such as the OHIP-14 has been criticised as not adhering to the utility concept. 30 Nonetheless, its ease of administration and potential use across all oral conditions may provide a balance toward its usefulness in allocating resources for oral healthcare, and this prompted us to conduct this study.
Generally, there were improvements in the clinical parameters and QOL indicating positive treatment outcomes. The gain of 0.3 mm CAL is acceptable compared to published literature on periodontal clinical treatment outcomes. 32 Improvements in OHIP-14 scores and EQ5D utilities are consistent with findings of studies that use QOL as a patient-reported outcome of periodontal intervention.8,9
The measurement of QALYs for periodontitis patients was included in this study as little has been studied about this. The value of QALYs for periodontitis patients that have yet to be treated is 28.92, which is lower than the life expectancy of this patient cohort, which is 35.76 years (Table 3). This suggests that by using EQ-5D utilities scores it is possible to conclude that chronic periodontitis does impact general health and that it lowers the QALY of the sufferers. It also allows objective comparisons to be made across other systemic conditions when decision-makers need to allocate resources coming from a common source.
Higher gains in QATYs versus QALYs are not surprising. QALYs used life expectancy for measure of improved mortality—this measure is age-dependant and does not change after treatment. Hence, gains in QALYs are greatly influenced by improvement in morbidity. On the other hand, QATYs used TLE for measure of improved tooth mortality—this is not entirely age-dependant as its value changes considerably after treatment. Hence, gains in QATYs measure improvements in both tooth morbidity and mortality. Related to this, it must be noted that estimates of TLE do not consider a patient’s age upon receiving periodontal treatment; therefore, theoretically TLE may appear to exceed the life expectancy of the patient, although in reality that is not the case.
Global ratings were consistent with clinical findings and QOL items. They indicated higher magnitude of improvements in oral health compared to general health which is not surprising. Improvements in health as an outcome of periodontal treatment confirms the role of oral health in improving general health outcomes
We found the method of estimating QATY using utilities derived from OHIP-14 combined with TLE as performed in this study to be practical and convenient. The inclusion of QALY measures in this study demonstrated that chronic periodontitis can impact patients’ QOL and consistent with that of tooth-related quality of life (as demonstrated by OHIP-14). Reasonable gains in both QALYs and the newly developed QATYs are statistically significant (P < .05) following periodontal treatment, allowing for the null hypothesis to be rejected. Further, improvements in these utilities scores were consistent with those of clinical measures as well as patients' global ratings of health.
The use of both QALYs and QATYs in this study demonstrated consistencies with those of clinical measures as well as patients’ global ratings of health and suggests its usefulness as a basis for cost-utility studies. Since use of utilities in various aspects of oral healthcare are still relatively scarce, further efforts to investigate its applicability and usefulness in resource decision-making are much needed. Nonetheless its acceptability as a true utilities measure is limited due to the absence of a sacrifice or trade-off component and hence requires further refinement.
Footnotes
Acknowledgements
The authors gratefully acknowledge the permission given by the Ministry of Health, Malaysia, to conduct the study at the government dental clinics. Special thanks to the Director-General of Health, Malaysia for permission to publish the article and to all the staff on data collection sites for their kind assistance. The views expressed in this article are those of the authors, and do not necessarily reflect the policies of any organisation.
Authors’ Contributions
TMD: study conception, data collection, data acquisition and analysis, data interpretation, manuscript writing; RA: data collection, data acquisition and analysis, data interpretation, proofread the manuscript, SEWP: study conception, data interpretation, proofread the manuscript; MT: study conception, data interpretation, manuscript writing; SMA: study conception, data analysis, data interpretation, proofread the manuscript. All authors approved the final version of the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding was received from the Ministry of Higher Education, Malaysia (ERGS/1/2011/SKK/UKM/02/73).
Ethical Policy and Institutional Review Board Statement
Permission to conduct the study was granted by the Ethics and Medical Research Committee of the National Medical Research Registry of the Ministry of Health, Malaysia (NMRR-10-603-6147), dated May 31st, 2010. All the procedures have been performed as per the ethical guidelines laid down by Declaration of Helsinki (2008).
Patient Declaration of Consent
Informed written consent was obtained from all patients for participation in the study and publication of the data for research and educational purposes. Participants were given freedom to withdraw from the study at any point. Regular care was ensured to the participant in the case of withdrawal.
Data Availability Statement
The data set used in the current study is available upon request from the corresponding author.