
Abstract
Aim:
To assess the dental and oral morbidity in multiple myeloma patients as expressed in dental radiographs before autologous stem cell transplant.
Materials and Methods:
A retrospective study involving 79 multiple myeloma patients was designed to collect data prior to their autologous stem cell transplant. Patients were seen at the oral medicine clinic at the University of Florida College of Dentistry during the years 2010–2013. Through available patient data and interpretation of radiographs, the following variables were recorded: age, gender, carious lesions, periodontal disease, and periapical radiolucency. In addition, the incidence of root fragment retention and the presence of punched-out osteolytic lesions were recorded. Cochran–Mantel–Haenszel (CMH) tests and logistic regression were performed for descriptive analysis and presentation of the data.
Results:
Seventy-nine multiple myeloma patients were recruited for this study. Ages ranged from 28 to 79 years (mean = 61, SD = 9.6), including 41 (51.9%) females and 38 (48.1%) males. The results demonstrated dental decay in 64.56% of patients, periodontal disease in 62.03%, apical rarefying osteitis in 13.92% of patients, and punched-out lesions in 24.05% of patients.
Conclusion:
Our study indicates high dental morbidity in multiple myeloma patients prior to autologous stem cell transplant. The elimination of foci of infection is highly recommended prior to autologous stem cell transplant for this high-risk population because of the potential risk of bacteremia/septicemia from oral bacteria associated with dental morbidity.
Abbreviations
ASCT: Autologous stem cell transplant
CI: Confidence interval
CMH: Cochran–Mantel–Haenszel
FMS: Full mouth series
IRB: Institutional Review Board
MM: Multiple myeloma
NHANES: National Health and Nutrition Examination Survey
OR: Odds ratio
Introduction
Multiple myeloma (MM) is a malignancy, which is characterized by a monoclonal proliferation of plasma cells. The annual incidence of MM in the United States is around 5.6 per 100,000 persons. 1 According to the National Cancer Institute, there were approximately 22,000 new cases of MM reported in the United States in 2013. The incidence of MM comprises 1% of malignant diseases in general, while it constitutes 10% of hematologic cancers and is considered the second most common hematologic malignancy after the non-Hodgkin lymphomas.1–3 The clinical manifestations of the disease are seen as the result of an expanding plasma cell mass in the bone marrow and other factors produced by these cells such as light chain monoclonal immunoglobulin, Bence-Jones proteins, and osteoclast activating factors. 2
MM is most common in the sixth and seventh decades of life. The clinical signs and symptoms are bone swelling or pain, anemia, and fatigue. Although punched-out lesions may be asymptomatic, they might be seen radiographically involving multiple bones. 2
There is no definitive therapy for multiple myeloma, most patients require autologous stem cell transplant (ASCT) that usually results in immunosuppression and increases the patient’s susceptibility to oral and systemic infection.4–7,18 Oral infections can cause major complications for these patients by becoming a source of bacteremia/septicemia and may lead to acute respiratory distress syndrome along with acute respiratory failure in rare cases. 8 Therefore, it is imperative that MM patients are screened for dental morbidity and any evident potential source of infection in the jaws. 7
In spite of the potential importance of dental infections in the prognosis of MM patients, the literature regarding dental morbidity in MM patients is scarce. The purpose of this study was to evaluate dental morbidity in MM patients, as expressed in radiographs, and to study the oral radiological features of this condition. The null hypothesis proposed by the authors is as follows: There is no significant difference in gender with dental morbidity in MM patients undergoing pre-ASCT.
Materials and Methods
A retrospective study comprising radiographic interpretation of the dental charts as well as the radiographs of MM patients prior to autologous stem cell transplant (ASCT) was performed. The study protocol was reviewed and approved by the Institutional Review Board (IRB) of the University of Florida College of Dentistry, and all the participants had signed informed consent documents. All dental records of patients treated at the oral medicine clinic at the University of Florida during the years 2010–2013 were reviewed retrospectively.
Inclusion criteria for subjects were (1) a complete dental examination with at least one panoramic and full mouth series (FMS), (2) at least 14 teeth present in patients before ASCT, (3) patients prediagnosed with MM, and (4) patients undergoing ASCT.
Exclusion criteria for this study were (1) patients missing dental imaging, (2) patients with no prediagnosed MM, and (3) patients not undergoing ASCT.
To prevent any potential bias, two oral and maxillofacial radiologists individually reviewed the dental radiographs of the patients included in the study. The agreement between the two observers was 92%.
The following information was retrieved: age; gender; radiographic manifestation of carious lesions, periodontal bone loss, and periapical radiolucencies; and incidence of root tip retention. The presence and location of punched-out lesions were recorded as well.
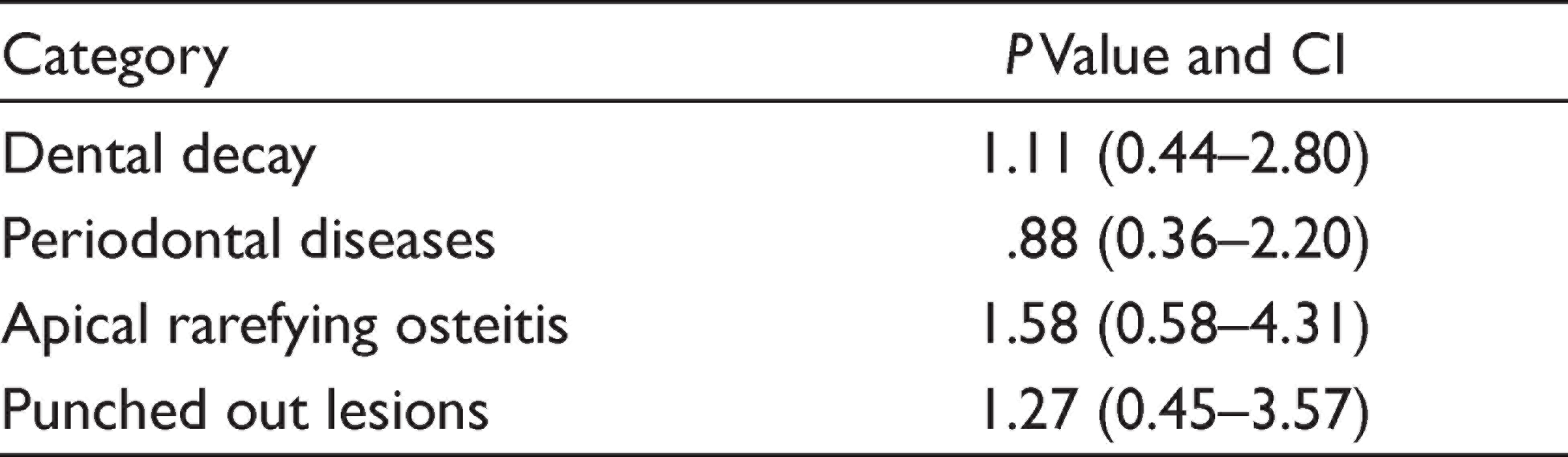
We performed descriptive analyses, and all statistical analyses were performed using the SAS v9.3 statistical software program (SAS Institute Inc., Cary, NC), which was used for Cochran–Mantel–Haenszel (CMH) tests and logistic regression at two-sided α = 0.05. The CMH test is used to measure the strength of the association between an exposure and disease. Here we used CMH and logistic regression to estimate dental morbidity in MM patients undergoing pre-ASCT. All data were evaluated at a significant level (P = .15, degree of freedom = 1, and 95% confidence interval) (Table 2).
Results
We collected data from 79 MM patients aged 28–79 years (mean = 61, SD = 9.6), including 41 (51.9%) females and 38 (48.1%) males. Four participants (two males and two females) were edentulous. Of the 75 dentate patients, 51 (68%) had at least one carious lesion and 49 (65%) had periodontal disease. Females had similar odds as males of having at least one carious lesion (OR = 0.88; 95% CI = 0.33–2.32) or periodontal disease (OR = 1.13; 95% CI = 0.43–2.92) after adjustment for age. Females tended to have fewer caries (two or less) vs. males (39% vs. 55%, respectively; P = .15).
Eighty-nine percent of patients presented with at least one radiological finding that needed dental treatment. Most of these lesions were untreated dental decay (68%), followed by periodontal disease (65%), retained root (12%), and periapical radiolucency (11%).
Dental Decay
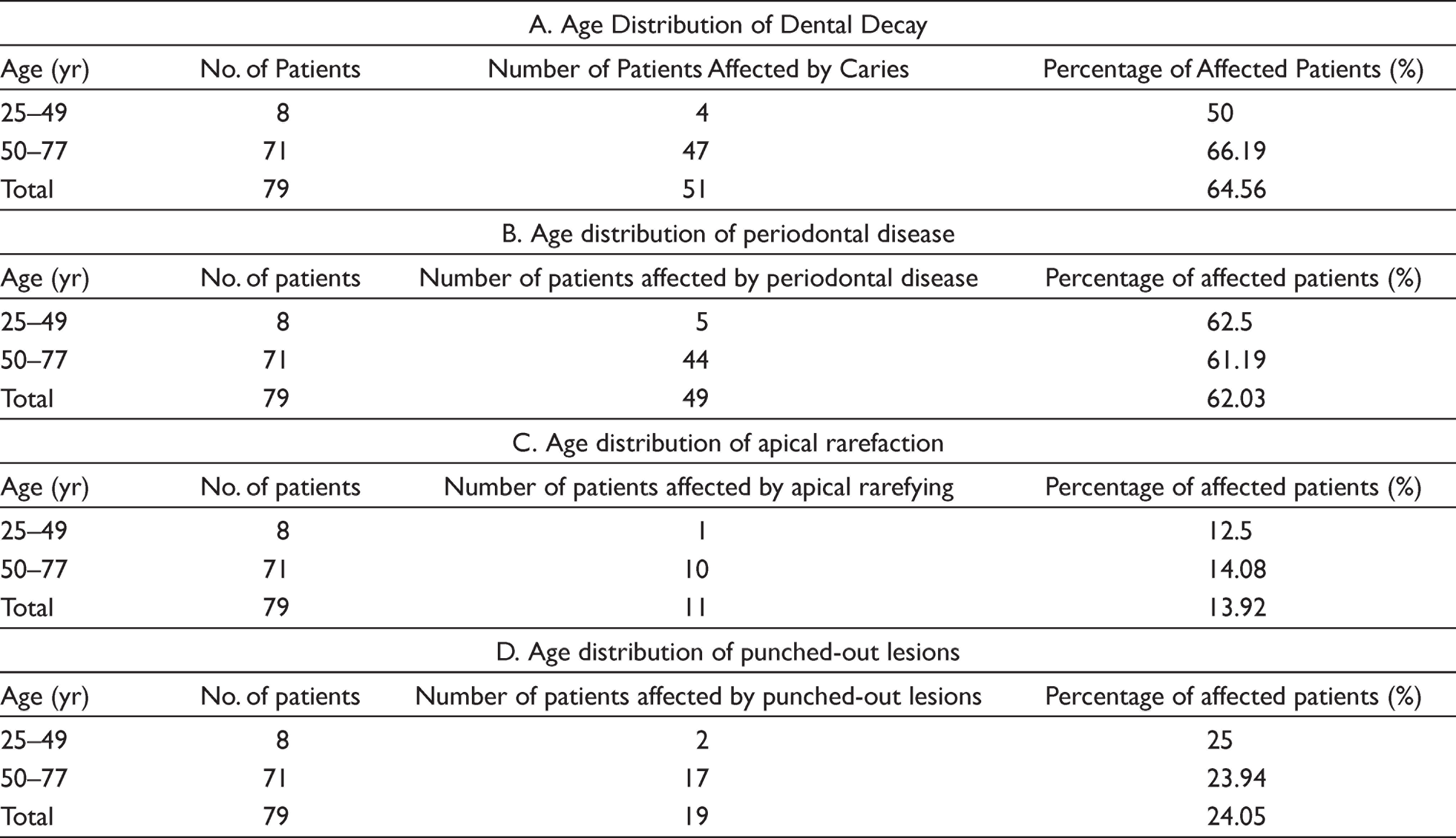
According to this study, 64.56% of patients had dental decay. The highest incidence (75%) was among patients aged between 50 and 64 (Table 1A). There was no significant difference between males and females (P value = 1.11) (Table 2).
Age Distribution of Different Dental Morbidities in Multiple Myeloma Patients Prior to ASCT
Difference in Dental Morbidity Among Males and Females Undergoing Pre-ASCT
Periodontal Disease
Sixty-two percent of patients were diagnosed with periodontal disease, i.e., periodontal bone loss with mild (31.4%), moderate (45.7%), and severe (22.8%) periodontal bone loss; 62.03% of patients had periodontal disease (Table 1B). There was no significant difference in gender (P value = .88) (Table 2).
Apical Rarefying Osteitis
Apical rarefying osteitis was found in 13.92% (Table 1C). It affected 14.63% of female patients and 10.52% of male patients with no significant difference in gender (P value = 1.58) (Table 2).
Punched-out Lesions
Punched-out lesions were observed in 24.05% (average) of patients (Table 1D) without significant difference in gender (P value = 1.27) (Table 2). Out of these patients, 28% were between the ages of 35 and 64 years with 94% of the punched-out lesions seen in the mandible.
Discussion
Septicemia in general is a cause of death in hematopoietic stem cell transplant recipients. In one study, 63.6% of total cases had a positive blood culture for septicemia. Twenty-six percent of septicemic cases were most likely of periodontal origin, 29.87% were most likely of oral origin (Streptococcus mutans, Capnocytophaga species, and Micrococcus species), and 63.63% were of other origin (Enterococcus faecalis, Staphylococcus epidermidis, Escherichia coli). 8 Oral infection can lead to septicemia in myeloablated hosts; therefore, eliminating oral disease may reduce the risk of bacteremia from oral origin. Fernandes studied the oral status of patients submitted to ASCT, the majority of them being MM patients (70.8%). The main limitation of this study, as reported by the authors, was that the data were underestimated since the patients were only examined clinically. 9 Therefore, in the present study, we concentrated on the radiological interpretation, as this may more accurately represent dental morbidity. 10
Some investigators report that periodontal status is associated with increased incidence of septicemia and bacteremia based on clinical parameters only.9,11 Although there is no sufficient literature on the impact of periodontal status in MM patients, in some studies it has been suggested that MM patients are usually vulnerable to periodontal diseases that range from mild bleeding to severe tooth mobility. 3 In our study, we observed that the majority of MM patients had some form of periodontal disease (65%). Data from the National Health and Nutrition Examination Survey (NHANES) 2009–2010, which was based on clinical examination, found that 57.2% of US dentate adults aged between 50 and 64 years had periodontitis. 12 A study conducted in Japan by K. Yamagata found that a total of 18.2% of subjects exhibited crestal alveolar bone loss of 20% or greater in whole-mouth radiographs, which was characterized as signs of destructive periodontal disease. However, this result included all age groups (Table 3). 13
Present Study Compared to Other Studies

In our study, apical rarefying was found in 25.31% of patients (Table 3). This is consistent with the study by Yamagata et al. that demonstrated that 26.76% of subjects were diagnosed with apical periodontitis. 13 It has been proposed that these lesions, having originated from the pulp tissue, may spread to the surrounding connective tissue, bone, lymphatic system, and blood stream. Through this pathway, the bacteria can reach the blood and cause septicemia.8,15
We have found the greatest incidence of untreated dental decay of 68% for patients aged between 50 and 64 years. This was higher as compared to NHANES, which is considered an important source of information on oral health and dental care in the United States. NHANES had reported only 22.14% of adults aged between 50 and 64 years with untreated decay. 12 The overall incidence of caries in all age groups in our sample was 64.56% (Table 3).
Punched-out osteolytic lesions are common in MM patients, and their occurrence is considered one of the important signs of the disease.2,14 Some of these lesions are often seen in late stage MM. 2 We have identified punched-out lesions in the jaws of 26.32% of MM patients (Table 3). In an earlier study, 5.18% of MM patients had typical osteolytic alterations of the jaws. 14 In the same study, all the lesions were in the mandible, whereas the maxilla was never involved. 9 However, we recommend further investigation into the rate of occurrence of myelomatous lesions in the skeletal structures of the oral cavity, in large series of patients undergoing systematic radiologic screening, both at the time of diagnosis and after the start of chemotherapy during the course of the disease.
The limitations of the present study are that a control group could not be established due to problems with matching hospital-based control groups and time limitations. Therefore, our study was not a case-control study. Also, our present study is limited to dental radiological reports and does not include clinical oral examination. Further clinical examination may illuminate oral hygiene status and reveal more pathological findings. There was also a lack of information on patient race and socioeconomic status as well as systemic diseases, such as diabetes, and risk factors such as smoking habits, and a limited number of patients appropriate for the study. No confounding factor was found that affected our results, and this was one of the limitations of this study. Considering the limited period available for pre-ASCT dental treatment, minimal dental intervention to treat only the sources of potential infection is recommended.16–18 However, a protocol defining the appropriate detailed treatment modality according to the severity of each dental disorder remains to be described. This study was retrospectively carried out to assess the dental and oral morbidity in multiple myeloma patients prior to autologous stem cell transplant. Future research can be focused on the establishment of detailed treatment criteria for minimal intervention in potentially detrimental dental disorders and to judge the effectiveness of the protocol with a larger sample size.
Conclusions
As ASCT patients are immune suppressed to prevent rejection, any infection can become a source of septicemia in these hosts. Therefore, eliminating the source of infection is important. Our study results indicate a high dental morbidity in pre-ASCT MM patients with no significant difference in gender. The elimination of foci of infection are highly recommended before and after ASCT for this high-risk population.
Future scope: Future scope of a research can be focused on the establishment of detailed treatment criteria for minimal intervention in potentially detrimental dental disorders and to judge the effectiveness of the protocol with a larger sample size.
Footnotes
Acknowledgements
The authors would like to thank the University of Florida College of Dentistry for the support and help rendered.
Author Contributions
Taggreed Wazzan designed the research project and collected data, Rohan Jagtap analyzed the data and wrote the article including drafting and revision of the manuscript, Mahmoud Mona assisted with analysis and interpretation of data, and Joseph Katz helped with concept, design of the work, drafting, and supervision of the research project.
Data Availability Statement
Due to privacy and ethical concerns, neither the data nor the source of the data can be made available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Policy and Institutional Review Board Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Declaration of Consent
Informed consent was obtained from individuals for participation in the study and publication of the data for research and educational purposes.