
Abstract
Aim:
The concept of minimal intervention in dentistry is one of the most important stages of the preventive dentistry, and caries risk assessment (CRA) is an application that needs to be primarily evaluated in order to perform minimal intervention approaches. This study was aimed to evaluate the awareness of CRA and whether CRA is included in daily practice by dentists in Turkey.
Materials and Methods:
This study used a questionnaire survey. A survey was prepared and sent to the dentists who were registered with the Turkish Dental Association via e-mail. A total of 790 dentists returned and 95 respondents were excluded. All the registered dentists filled and returned their survey. Descriptive and logistic regression analyses were performed (n = 695).
Results:
A total of 86.9 percent dentists who took the survey said that they performed CRA in daily practice. “Lack of time” was specified as the most important factor by the respondents who did not perform CRA in daily practice (61.5%). Current oral hygiene status (96.4%) and the presence of one or more active caries lesions (74.5%) were considered the most important risk factors for not performing CRA. Results of multiple logistic regression analysis showed that clinical experience, number of patients treated per day, and type of practice were mostly associated with whether or not performing CRA (P = .012, .018, and .035, respectively).
Conclusions:
It can be concluded that most of the dentists are aware of the importance of conducting CRA and, with differences in the factors considered, CRA is required in their daily practice in Turkey. The concept of minimal intervention in dentistry is one of the most important stages of preventive dentistry, and CRA is an application that needs to be primarily evaluated in order to perform minimal intervention approaches.
Introduction
Dental caries is a generally preventable, fairly common, multifactorial, and dynamic disease that affects individuals of all age groups.1,2 In upper middle-income countries, prevention and minimal intervention of caries lesions are more important than treatment of caries at further stages. Therefore, the modern cariology concept aims to identify caries at the earliest possible stage and prevent caries development, including patient-specific factors.3,4 Because caries is a multifactorial disease affected by microbiological, behavioral, social, and individual factors, the increasing awareness of both physicians and patients about these risk factors is crucial for preventive dentistry approaches.
Minimal intervention dentistry is a philosophy that suggests useful strategies for both preventive dentistry and treatment of caries lesions.5,6 This philosophy allows the dentists to both accurately and early diagnose the lesions and prevent the disease recurring with protective procedures. 7
Caries risk assessment (CRA) is the first step of the minimal intervention and preventive dentistry, 8 and it should be obligatory of every initial examination for clinicians because personal habits that define the caries risk may change with time. This change may affect the treatment plan of patients. CRA is defined as the development of new caries lesions or continued progression of existing lesions in a patient at a time interval, where all etiological factors such as diet, time, sensitive tooth surface, and plaque levels are assumed to be constant. 9 Determination of risk factors is important for clinicians to classify patients as low, moderate, and high caries risk groups, and manage the appropriate and individualized treatment plan for each patient.
With the understanding of the prevalence of CRA and importance of identification of individual risk factors, many studies have been examined whether or not dentists include risk assessment during their daily treatment approach, and the significance of risk factors.8,10,11 However, to the best of the authors’ knowledge, no previous studies conducted in Turkey have examined the dentists’ CRA knowledge and investigated the risk factors that they consider in adult patients.
The aims of this study were to quantify the awareness of the dentists’ decision about CRA and evaluate the dentists’ rating of the importance of specific risk factors when they develop a CRA plan in adult patients. We tested the hypothesis that performing CRA situations is significantly associated with the practice pattern characteristics of dentists.
Materials and Methods
Study Design
A study consisting of a questionnaire survey was conducted which was administered to dentists in Turkey between January and June 2018. The study followed the approval from the Ethics Committee of the Gazi University (No: E107384) in accordance with the Declaration of Helsinki.
Participants and Questionnaire Survey
A questionnaire form similar to the one that was previously prepared by Riley et al. was prepared for data collection. 8 The questionnaire was translated into Turkish and coordinated according to the dentists working in Turkey to evaluate their knowledge and practice patterns about CRA. It consisted of 11 questions including the following parts: demographic and descriptive characteristics of respondents; gender, clinical experiences and PhD or proficiency situations as educational information, type of practice, practice busyness Questions relating to the dentists’ behavior concerning the use of CRA during treatment planning, reasons why dentists do not undertake CRA, risk factors considered during CRA, reading of scientific articles, and believe in the importance of CRA.
The questionnaire was sent via e-mail by the Turkish Dental Association (TDA) to registered dentists with a letter describing the study and including an informed consent. A reminder card was sent by email 15 days later to all dentists for the purpose of optimizing the response rate. Incomplete and incorrectly filled questionnaire forms were excluded. Dentists were asked about their educational information, type of practice, years of practice, daily practice patterns, CRA status and risk factors they consider.
Statistical Analysis
All analyses were performed using IBM SPSS Statistics version 17.0 (IBM Corporation, Armonk, NY, USA). Descriptive statistics were calculated for the participants about professional and practice information. Pearson’s chi-square test was used for the analysis of the categorical variables.
Multivariate logistic regression analyses were performed and odds ratios (ORs), with the confidence interval at 95 percent (95% CI), were calculated to indicate the associations between the use of CRA and practice pattern factors of the participants and socio-demographic characteristics of the respondents. For all tests, a significance level was set at P < .05.
Results
Among 790 respondents, 95 were excluded owing to incomplete and incorrectly filled questionnaire forms, and valid responses were collected from 695 (88%). Table 1 shows the comparison of demographic, clinical experience, and the practice pattern characteristics of the respondents whether or not performing CRA. The majority of the dentists in this study were general practitioners (81.9%) and working in private clinics (83%). A total of 86.9 percent respondents performed CRA as a part of their treatment planning.
With regard to experience since graduation, when the respondents were evaluated on whether they performed CRA or not, those who had been graduated for 1–5 years were found to be statistically significantly higher (P = .006) and those who had been graduated for more than 20 years were found to be less (P = .012). When the respondents who performed CRA were evaluated on practice type, the percentage of respondents who were in the private practice was 84.3, and it was higher than those who were in public practice (P = .035). In terms of practice busyness, the percentage of respondents who treated more than 20 patients per day and claimed not to perform CRA in their clinical practice was 23.1 and that was significantly higher than those who were performing CRA (P = 018).
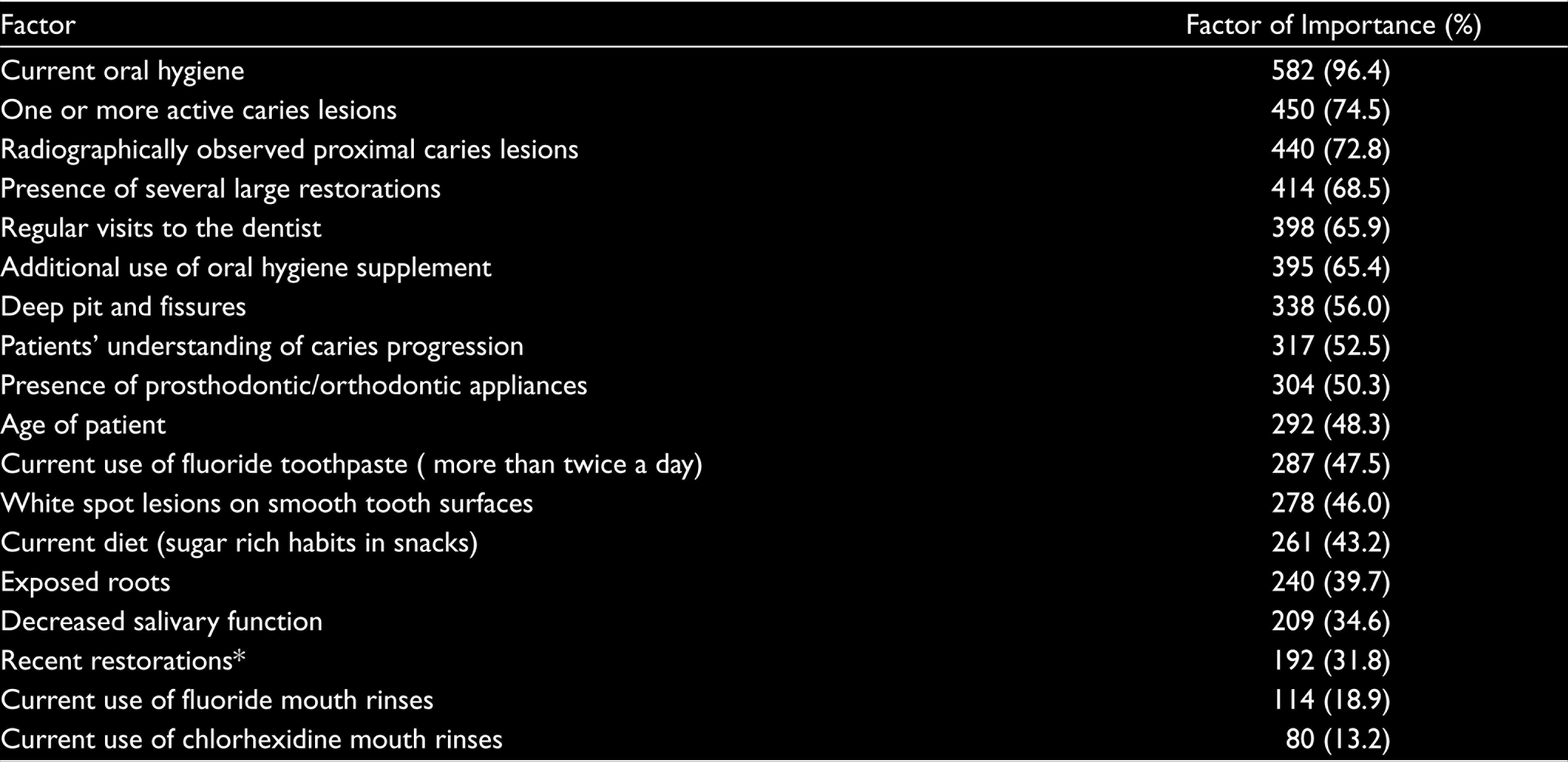
Table 2 shows the rating of the importance of caries risk factors when performing CRA. Current oral hygiene (96.4%), the presence of one or more active caries lesions (74.5%), and radiographically observed proximal caries (72.8%) were rated as the most important risk factors. Conversely, current uses of chlorhexidine (13.2%) and fluoride rinses (18.9%) were rated as the least important risk factors when performing CRA.
Comparison of Demographic, Descriptive, Practice Characteristics of Respondents by Whether or Not Performing CRA
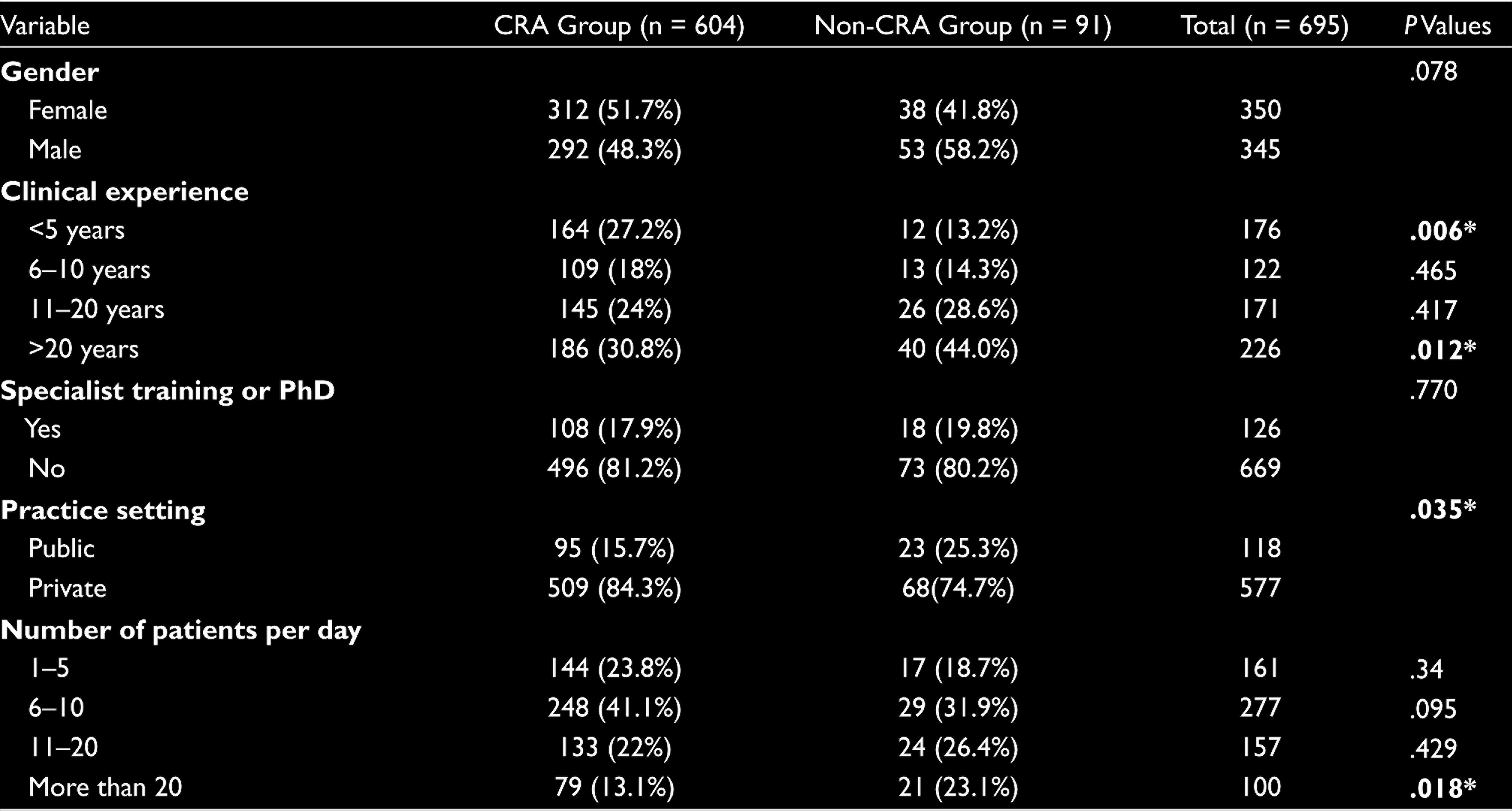
*Statistically significant differences are highlighted in the bold font (significant at the .05 level).
Percentage Distribution of Risk Factors to be Considered by Respondents in a CRA (n = 604)
Of the respondents, 13 percent reported that treatment plans were not included in the assessment of caries risk. Table 3 presents the summary of the reasons why some respondents do not undertake CRA. Lack of time (61.5%) and insufficient attention of patients (48.4%) appear to be the most important factors identified.
The multivariate logistic regression performed to analyze the association between performing CRA during daily treatment plans and the factors affecting is shown in Table 4. The findings indicate that the most important factors for not performing CRA were clinical experience, number of patients treated per day, and the number of respondents in public practice, respectively. ORs (95% CI) for the “clinical experience between 11 and 20 years” and “more than 20 years” were 2.51 (95% CI: 1.215.23) and 3.45 (95% CI: 1.716.97). Additionally, ORs for “working in public” and “treated more than 20 patients per day” were 1.85 (95% CI: 1.053.25) and 2.41 (95% CI: 1.174.97), respectively.
Reasons Why Respondents Do Not Perform CRA (n = 91)

Results of Multivariate Logistic Regression Assessing the Association Between the Performing CRA and the Factors That Might Affect It
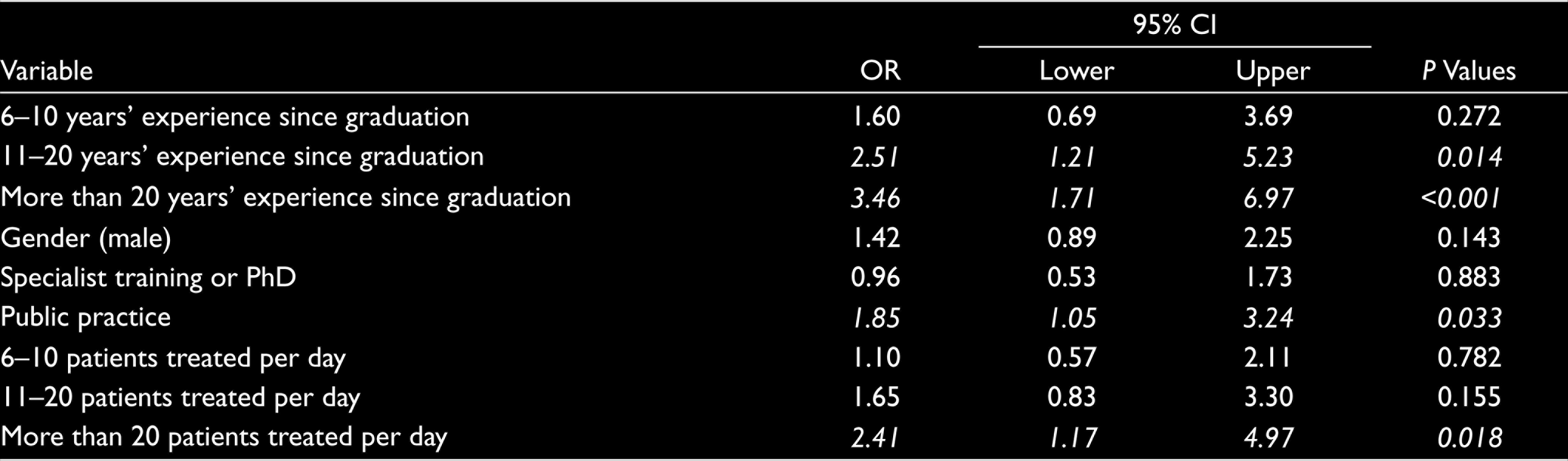
Statistically significant odds ratios are highlighted in bold italic font.
Discussion
To the best of the authors’ knowledge, this is the first study that investigates the knowledge and decision of Turkish dentists to conduct CRA in adult patients in their daily dental practice. The questionnaire used in this study was designed for dentists in Turkey but was based on that performed by Riley et al. 8 before. The questionnaire was sent to the respondents who were registered with TDA via e-mail. For this reason, the number of respondents was lower than we expected, and hence this represents a small group. Although this questionnaire survey study was conducted with a limited number of groups, the findings provide guidance on dentists’ knowledge, decisions, and choices in the application of CRA in routine clinical practice in Turkey. In this regard, it is very important to evaluate and interpret the findings of the surveys. CRA is the key factor for the clinicians in both managing a minimal invasive and individualized treatment plan and defining the potential for future caries development and taking the required precautions. Therefore, the identification of the risk factors is the first and the most important step for clinicians to perform CRA. A study conducted in Turkey showed that previous caries lesions were an important indicator for the determination of the patient’s caries risk level. 12 In accordance with literature, in our study, current oral hygiene and one or more active caries lesions were rated the most important factors considered by the respondents during caries risk management.12,13
In this study, 86.9 percent of respondents responded that they undertook CRA in their daily clinical practice. In this survey, most of the respondents were not working in public clinics. In private clinics, patient appointments and number of patients to be treated per day can be organized by dentists in Turkey. The number of respondents performing CRA in this study might be related to this situation, depending on the increase in time allocated by the physician to a patient in private clinics. In our study, it was noted that lower rates of performing CRA were associated with dentists who worked in the public sector and treated more than 20 patients per day. The finding is, however, different from the 31 percent stated by Riley et al. 8 for the United States and Scandinavian dentists who belong to the Dental Practice-Based Research Network (DPBRN) and much lower than 74 percent reported by Kakudate et al. 10 for Japanese dentists who were affiliated with the DPBRN in Japan.
Findings about respondents performing CRA in daily practice, obtained in our study may provide a more positive picture than observed in the clinic but is still promising and must be supported by increasing the awareness of patients about risk factors and protection for caries development. The incidence of caries lesions in societies can only be reduced by raising the awareness of the patients and coordination between physicians and patients. The high rates of performing CRA in this study may be related to the number of respondents participating in this study. Therefore, in further studies, the questionnaire may be applied to a larger group, and results may be expanded and compared with these findings. Among the respondents who claimed that they do not use CRA, 61.5 percent mentioned that the biggest reason for not performing CRA in daily practice was the lack of time and 48.4 percent stated that the cause was insufficient attention of patients about oral hygiene motivation. Based on these findings, time allocated for a patient and patients’ interests about their oral health are the key factors for a practitioner to improve minimal invasive and preventive dentistry approaches. The population investigated in that study was only adults and elderly people in Turkey. In the study, a total of 3176 people were examined between the ages of 35–44 (adults) and (65–74) elderly due to the standards determinated by WHO fundamental principles guide. Therefore, the information about the exact numbers for both adults and elderly against the total population is not included. Adults visited the dentist more than a year was 57% in that study. 14 These results and our findings indicate that in Turkey, patients’ requirements and knowledge about their oral health care are still limited and must be improved for protective approaches. In a survey study conducted in France, similar findings were obtained regarding the causes for not performing CRA among practitioners. 13 This French study and a survey study in England emphasized the importance of patient-centered treatment planning and informing patients adequately about CRA by physicians in parallel with our findings.13,15
In this survey, it was not questioned whether the respondents used a special form when assessing caries risk. It may be beneficial to use a special form or a chart for CRA to record the data and evaluate the patients’ improvement about oral health care and increase the patientphysician collaboration for treatment planning. Actually, some different CRA systems have been reported before,16,17 and all of them remarked that the important thing for performing CRA is evidence-based data collection and proper identification of individualized factors. Certainly, it is important to save the information about patients in a form or a document, but it is also very important for the physician to perform CRA based on the currently available pieces of evidence.
CRA and informing the patients about this factors and precautions are the first steps of minimal invasive and preventive dentistry. Within the limitations of this survey study, the findings show that dentists need to spend longer and more productive time with their patients to inform them adequately about caries development and prevention. It is important to state that CRA is crucial not only for physicians to determine an effective treatment planning, but also for patients to be aware of individual preventive approaches and to reduce the incidence of caries in societies.
Conclusion
It can be concluded that most of the dentists are aware of the importance of conducting CRA and, with differences in the factors considered, CRA is required in their daily practice in Turkey. The concept of minimal intervention in dentistry is one of the most important stages of preventive dentistry, and CRA is an application that needs to be primarily evaluated in order to perform minimal intervention approaches.
Footnotes
Acknowledgements
The authors would like to thank all dentists who responded in this study and the Turkish Dental Associations for their support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Patient Consent:
Patient was explained before enrolling the participation. Informed written consent was taken for same.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.