
Abstract
Teeth with calcific metamorphosis pose a challenge to the endodontist in achieving proper access, identification, and debridement of the root canal. With the conventional technique, radiographs and bur orientation have dictated the access cavity preparation, which leads to the removal of more sound tooth structure and iatrogenic errors. To overcome these issues, the recent diagnostic imaging techniques such as cone beam computed tomography followed by three-dimensional fabrication of template have been proposed, which aid the clinician to accurately locate and negotiate the obliterated canal. The present case report describes the importance of conservative access cavity preparation with the use of the guided endodontic technique for the treatment of calcified canals in the maxillary central incisor.
Introduction
Dental trauma results in various complications, which pose an enigma to the practitioner. Calcific metamorphosis (CM) is one among the sequelae after trauma. According to the American Association of endodontists, it is defined as “A pulpal response to trauma that is characterized by deposition of hard tissue within the root canal space”. 1 It is also referred to as pulp canal obliteration, dystrophic calcification, diffuse calcification, and calcific degeneration. The mechanism for CM is unclear. According to Robertson, it may be caused due to the disturbance in the neurovascular circulation of the pulp. 2
According to the previous studies, 3 the incidence of calcification in canals was approximately 4%–24%. Endodontic treatment in calcified teeth is contradictable. Some studies suggest that these teeth need to be observed and a clinical followup is required before the endodontic procedure. 3 Teeth with symptomatic periapical pathology are considered to be ideal for intervention.
Teeth with canal obliteration can complicate easy access to the pulp canal leading to the difficulty in negotiation of the complete root canal, which can result in iatrogenic errors such as instrument separation and perforation, compromising the sound tooth structure. To minimize the procedural difficulties, Krastl et al. 4 have proposed a contemporary approach, guided endodontics, for early detection and negotiation of teeth with CM.
A good-quality radiograph in different angulations and different contrasts plays a major role in the diagnosis related to the extent of the calcification for proper endodontic access. However, the possible disadvantages in the radiograph such as faulty imaging technique, two-dimensional views, and processing errors have led to the search of newer imaging techniques.
Cone beam computed tomography (CBCT), a recent diagnostic aid in the field of endodontics, enables a three-dimensional (3D) view of hard and soft tissues and helps in the diagnosis and treatment planning. The present case report describes the clinical management of CM with symptomatic periapical pathosis seen in the maxillary central incisor using 3D prototyping techniques.
Case Report
A male patient aged 51 years had presented to the department of Conservative Dentistry and Endodontics with a chief complaint of pain in the maxillary central incisor from 1 month. The patient had a history of trauma 3 years ago. The pain was gradual in onset, intermittent, and dull aching in nature. He visited to a general dentist who advised endodontic treatment and prescribed medication. The patient did not undergo the procedure but took medication, which relieved his pain. Again 1 month later, he suffered with trauma in the same area of the involved tooth, resulting in dull, throbbing type of pain. The clinical examination revealed an intact crown with tenderness to percussion in relation to the maxillary right central incisor. No mobility was recorded. The tooth showed no response to vitality tests. The intraoral periapical radiograph revealed that there was radio-opacity involving the coronal aspect of the tooth and obliteration of the pulp canal associated with radiolucency involving the periapical region of 11 (Figure 1). The procedure was explained to the patient and an informed consent was obtained.
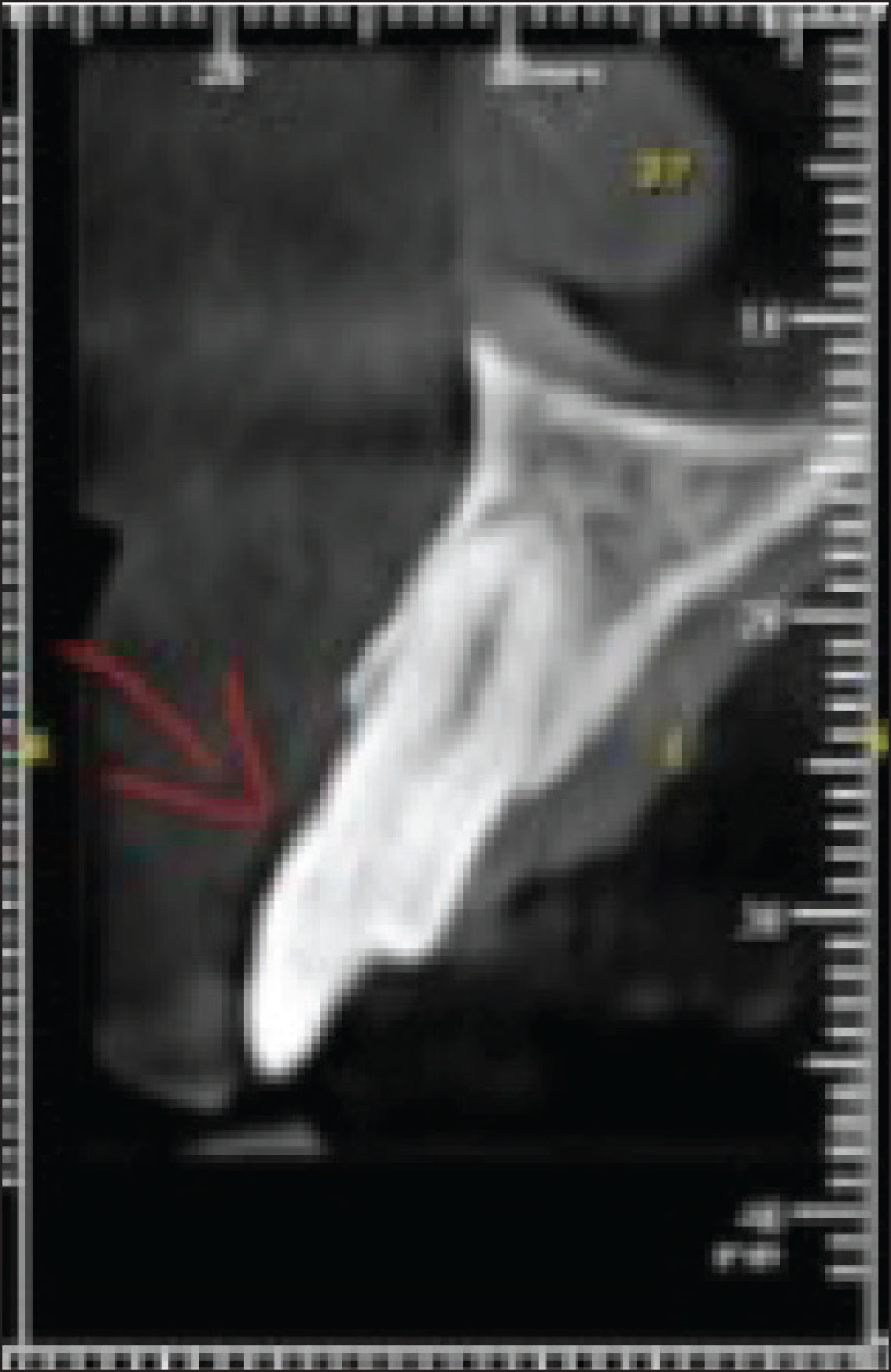
For accurate diagnosis and to know the extent of calcification, the patient was sent for a CBCT scan (HDX-WILL, Seoul, Korea) of # 11. The CBCT images revealed partial calcification involving the coronal part of the tooth approximating to the cervical third of the root (Figure 2).
Preoperative Radiograph

CBCT Scan
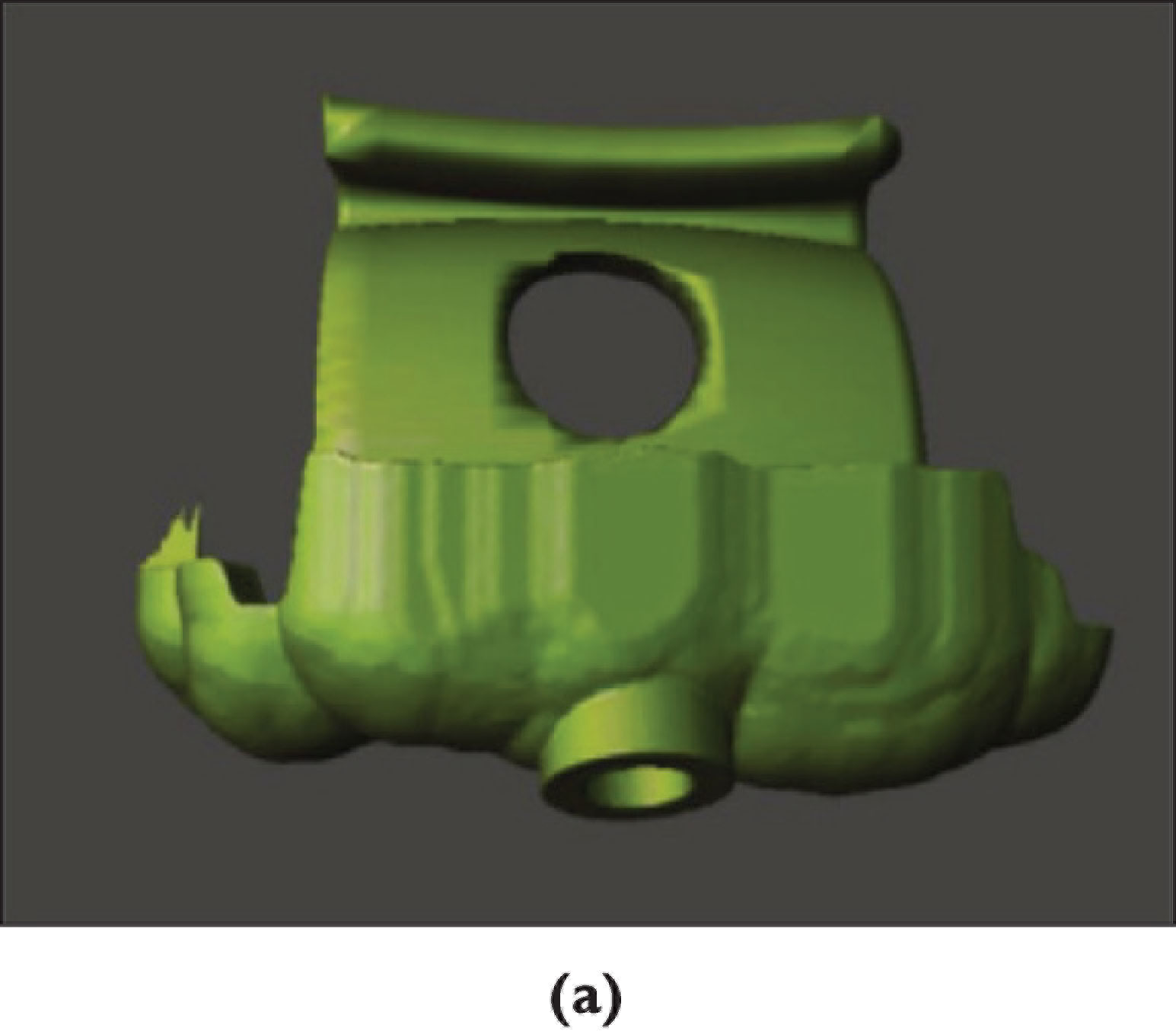
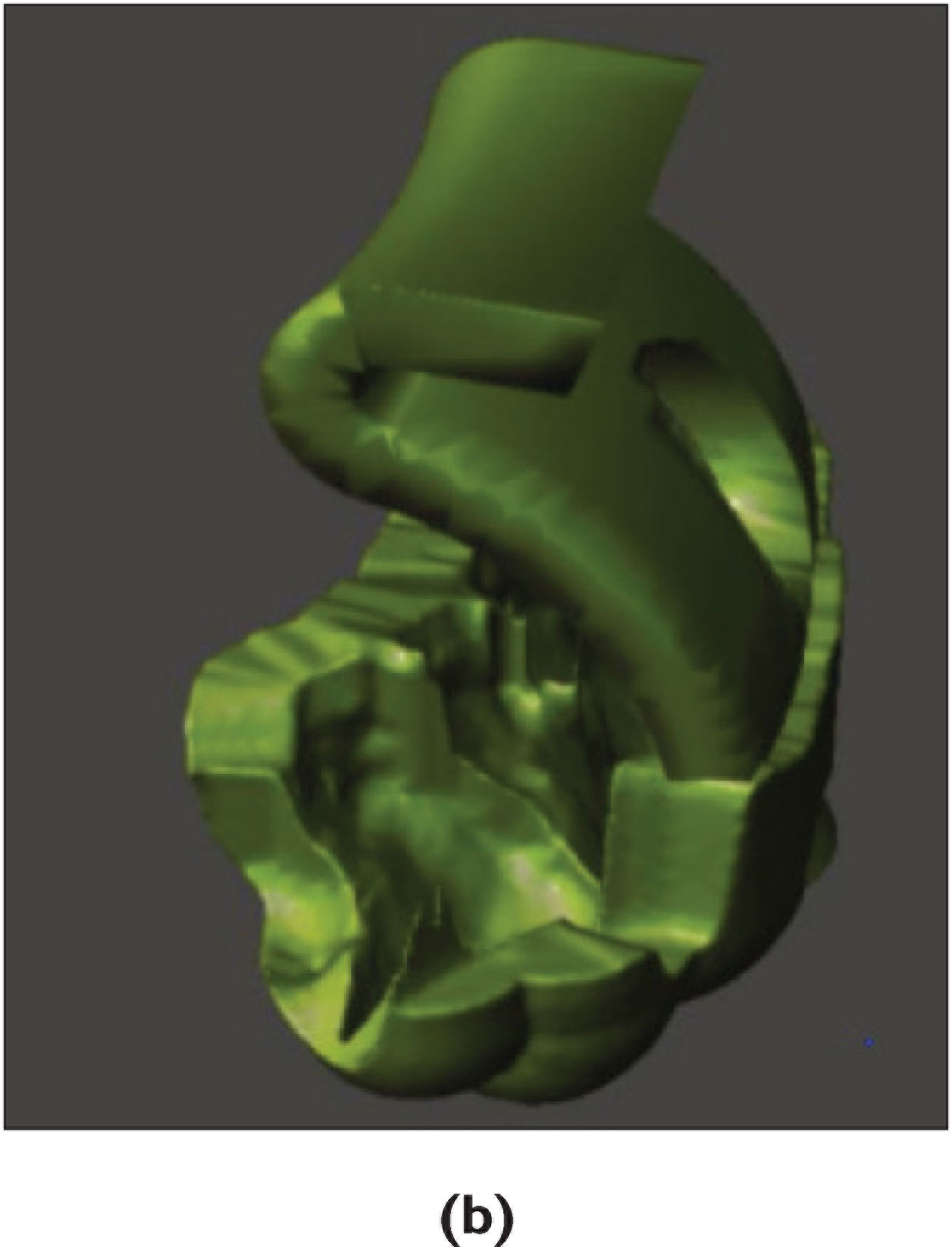
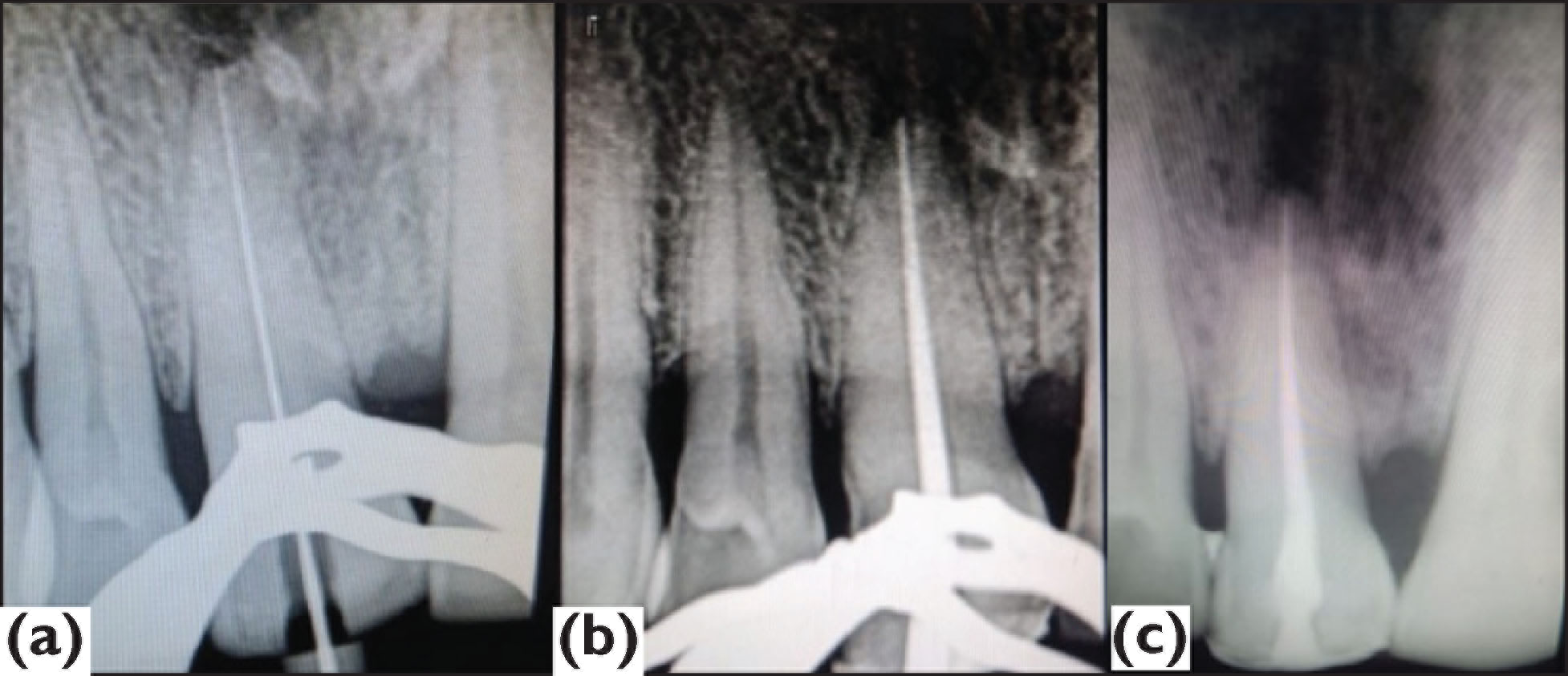
Applying a 3D software technique, a virtual template was fabricated by making an intraoral impression (Figure 3). Then, the patient was anesthetized and a conservative access cavity was prepared through the template until the dentin was exposed through guided endodontics drill till the apical third of the root. Through an incisal approach (Figure 4), the preparation was extended apically showing a minimally invasive access cavity, which was followed by a conventional root canal treatment (Figure 5) and passive irrigation was performed with 3 mL of 5% sodium hypochlorite and instrumented with a reciprocating file (R25, VDW. Munich, Germany), followed by intracanal medicament application and temporary filling (CavitTM, 3 M ESPE). After two weeks, the tooth was found to be asymptomatic and nontender to percussion. Obturation was performed using gutta-percha (Dentsply Tulsa, OK, USA) and AH Plus sealer (Dentsply, De Trey, Konstanz, Germany) (Figure 5c). Then, the access cavity was cleaned and closed with composite resin (IvoclarVivadent, Amherst, NY, USA) (Figure 6). Later on, the patient was reviewed after 3 months (Figure 7) which showed signs of healing.
(a) Customized Design of Template-Anterior View and (b) Customized Design of Template-Lateral View
Incisal Approach of Access Cavity

Conventional Root Canal Treatment. (a) Working Length, (b) Mastercone, and (c) Obturation
Post-Operative View

Three Months Followup

Discussion
Calcific metamorphosis of teeth is the most common sequela of dental trauma and dental caries.5,6 The stage of root development and the severity of trauma dictate the extent of calcification. Calcific obliteration of the tooth can lead to iatrogenic errors such as perforation, instrument separation, and compromised sound tooth structure during endodontic therapy. To avoid these errors, a thorough knowledge of root canal morphology and accurate diagnostic aids are mandatory.
Endodontic intervention of these teeth is quite debatable. Few studies have suggested that the management criteria include signs and symptoms along with the appearance of periapical rarefaction, which is radiographically evident. 7 Various methods were used for gaining proper access to the coronal calcification of the canal by using dental operating microscope, loupes, ultrasonic tips, and chelating agents. Recently, Krastl et al. 4 suggested a new method for gaining easy access to the coronal aspect of the tooth in the case of CM and periapical pathology by using a guided endodontic template.
Earlier the clinicians commonly used radiographic images for the initial assessment of the root canal morphology and its pathology. However, these images provided only two-dimensional information without any crosssectional details of the tooth. CBCT is a revolutionary imaging modality in the recent era of research, furnishing a 3D view and fine details through the thin sliced sections of axial, sagittal, and coronal planes of the involved tooth. In this case report, the patient was sent for CBCT imaging to accurately obtain the extent of the calcification, which helped in designing the template.
Based on the rapid prototyping technique, 8 an intraoral impression was made followed by scanning, and then it was uploaded into the virtual implant planning software. To prevent the deviation of the drill from its trajectory, a virtual template and guided sleeve (3.0 mm external diameter, 1.4 mm internal diameter, and 8 mm length) were customized by a 3D printer (Formlabs, USA). The guided endodontic sleeve was incorporated into the template to guide the drill during access cavity. After template try-in, endodontic treatment was performed. The postoperative radiograph shows the complete negotiation of the canal with the sound tooth structure.
Although this technique is very time-consuming and expensive, it may be justified as it helps in accurate diagnosis and thus reduces the occurrence of iatrogenic errors resulting in the increased tooth retention. There is a chance of technical failure if the traditional approach was used as that may lead to the extraction of the tooth, which necessitates the patient to rely on the expensive implant procedure. 9
The present clinical outcome reveals that the guided endodontic technique is proven to prepare minimal access cavity with predictable treatment outcome in teeth with CM. 10
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Patient Consent
Patient was explained before enrolling the participation. Informed written consent was taken for same.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.