
Abstract
Aim:
The aim of this study is to evaluate the relationship between children’s tooth decay risk score and a dental examination and parent reports of oral health practices.
Materials and Methods:
A cross-sectional correlational study utilizing data from an oral health assessment was performed by undergraduate nursing students and parents completed the permission forms.
Results:
Four hundred and fifty-six children received an oral health assessment. None of the percentages were found to be at high risk for tooth de cay and 21% were referred for further evaluation and dental treatment. Twenty-seven % of parents reported that their child was not being seen by a dentist and 49% reported that they had not established recommended tooth brushing practices in early childhood. In this analysis, the physical examination measures accounted for a significant amount of risk: R2 = 0.55, F(5,317) = 7.62, P < .00. The parent report measures offered little predictive power beyond the examination: R2 = 0.029, F(7,310) = 3.01, P = .00.
Conclusions:
These findings identify a need for a broader perspective to inform oral risk assessment and interventions to address oral health disparities. A social determinant of health framework would improve nursing students’ competency to identify children in need of early intervention. Oral health promotion at the family and community level would improve the preventive oral health practices.
Introduction
Dental caries are one of the most common chronic illnesses of childhood and the largest prevalence occurs in poor, socially disadvantaged minority groups. 1 Dental caries are not only a burden on the child and family but also on health economics. The United States spent $298 billion on dental treatment in 2010. 2 Interventions such as water fluoridation, tooth brushing with fluoride toothpaste, fluoride varnish, and dental sealants have been shown to be effective in preventing caries and are even more cost-effective in areas where risk factors are high. The role of parents is critical in facilitating and promoting these oral health behaviors in children. This study aimed to evaluate the relationship among parent-reported children’s oral health status, an oral health assessment conducted by undergraduate nursing students, and a tooth decay risk score.
Although programs such as school-based dental programs and policies that increased insurance coverage have resulted in increased access to dental service and a decline in the prevalence of dental caries in the pediatric population in the United States, it is still one of the most common chronic diseases among children. During 2011–2014, 13.7% of children aged 2 to 8 years had untreated dental caries in their primary teeth and the proportion increased with age: 10.9% among children aged 2 to 5 years and 17.4% among children aged 6 to 8 years. A larger proportion of Hispanic (19.4%) and non-Hispanic black children (19.3%) had untreated dental caries in primary teeth compared to non-Hispanic white (9.5%) children. 3 In the 2011–2014 period, children and adolescents in families with incomes less than 100% of federal poverty guideline (FPG) were more likely to have caries than children and adolescents in families with incomes greater than or equal to 200% of FPG. 3
Left untreated, dental decay can result in pain, infection, impaired chewing and poor nutrition, issues with speech and missed time from school, and poor academic performance.4,5 In addition, absenteeism from school for children results in missed workdays for parents and caregivers. 6 Consequently, oral health is a priority focus area in Healthy People 2020, with the goal to improve oral health by focusing on prevention and increasing access to dental care services. 6
Numerous modifiable risk factors for dental caries exist. Children with caries consume between meal juice and sugary snacks more often than children who are caries free. 7 The risk increases when children fall asleep with a bottle filled with sweet fluids because salivary flow is reduced during sleep. 7 Maternal behaviors significantly associated with early childhood caries (ECC) include frequent consumption of unhealthy food, infrequent dental visits, poor oral hygiene, and smoking. 8 A study investigating household smoking in 76,920 children concluded that exposure to tobacco smoke at 3 years of age was associated with a twofold increase in the risk of childhood caries. 9
Several preventative actions are protective against tooth decay. The American Academy of Pediatrics (AAP) recommends that children begin regular dental visits at 1 year of age. 10 In a study of over 42,500 children, researchers found that beginning dental visits before the age of 4 years allow for the opportunity to intervene and lead to less restorative treatments, such as crowns or extractions, than beginning dental visits after 4 years of age. 11 Dental insurance status, regardless of the type, correlates to an increase in the use of dental services, as well as a decrease in the number of unmet dental needs. 12
Fluoride is one of the main factors responsible for the decreased prevalence and severity of dental caries in the United States. However, too much fluoride while teeth are developing can cause pitting and discoloration of the tooth enamel (dental fluorosis). It is recommended that children’s teeth be brushed twice a day as soon as the teeth erupt with plain water. 13 After the age of 2 years, teeth should be brushed with a smear the size of a grain of rice of fluoridated toothpaste. After the age of 3 years, a pea-sized amount can be used. 14 In a survey of tooth brushing practices, 80% of children aged 3 to 15 years began tooth brushing after the age of 1 year, approximately one third brushed once a day, and nearly 40% of children aged 3 to 6 years used too much toothpaste. 14 These findings indicate that parents/caregivers need education regarding recommendations for tooth brushing and the amount of fluoride toothpaste to use.
Fluoride varnish is a professionally applied concentrate of fluoride. A systematic review reports that topically applied fluoride varnish may reduce caries by 37%. 15 In 2011, the Arkansas legislature passed Act 90 allowing Arkansas physicians, nurses, and other licensed health care professionals in addition to dentists, dental hygienists, and dental assistants to apply and be reimbursed for fluoride varnish. 16
Many research studies have confirmed the benefits and safety of community water fluoridation. According to the Centers for Disease Control (CDC), community water fluoridation is responsible for decreasing 25% of caries in adults and children. 17 For over 70 years, communities in the United States have benefited from community water fluoridation, considered as one of the public health’s greatest achievements. Currently, three in four Americans who drink from public water supplies obtain enough fluoride to prevent tooth decay. According to the CDC, bottled water may contain fluoride, depending upon the source of the water, but it may not be enough to prevent tooth decay. 17 Geographic, racial, ethnic, and environmental influences contribute to preferences for bottled water. Consumers are more likely to believe that bottled water is safer or tastes better if they have been exposed to unsafe water or live in areas with water quality standards variations. Blacks and Hispanics are more likely to drink bottled water due to increased risk beliefs and greater exposure to unsafe water. 18
One study aimed to investigate the levels of fluoride in tap and bottled water in Arizona counties with a high prevalence of dental caries. Bottled water consumption is common in this area due to concerns regarding tap water quality. 19 Fluoride detection levels were significantly greater in tap water than bottled water, but still below the level for optimal dental health (0.7–1.2 mg l1). Concentration of fluoride in the bottled water samples was below the quantitative detection limit of 0.4 mg l1. Researcher concludes that low-income children in this region would benefit from regular access to fluoride varnish treatments and/or use of fluoridated mouthwash. 19
Dental sealants applied in childhood can help prevent about 90% of posterior caries for 1 year and about 50% for 5 years after placement. 4 In a survey of dental sealant awareness, 50% of adults in general and 55% of parents knew about the purpose of dental sealants. Adult knowledge was higher among women, non-Hispanic whites, and those with more than a high-school education. 20 These findings suggest that oral health promotion programs designed to reach the low-income and racial/minority parents could reduce disparities in sealant knowledge and untreated dental caries.
Reducing socioeconomic barriers remains an important strategy to decrease the prevalence of childhood dental caries. A systematic review of evidence about preventive strategies for children and adolescents with immigrant or low socioeconomic backgrounds found that an effective prevention technique included supervising tooth brushing in schools and targeting nutrition and oral health education of mothers. 20
ECC is associated with a negative impact on oral health quality of life of the children and their parents. An important aspect of oral health related quality of life is the feeling of guilt in parents. In a study to assess whether parents feel guilty for their children’s oral health problems, results indicate that guilt in parents was significantly associated with ECC and the thought that the problem could have been avoided. 21 These findings suggest that feelings of guilt can be reduced or avoided if parents have accurate knowledge of their child’s oral health status, know the potential consequences, and take the proper action to prevent caries and their progression.
Setijanto et al. used the theory of planned behavior to describe mothers teaching tooth brushing to their preschool children. 22 Attitudes and perceived behavioral control, the perception of the ability to perform an action given risks or constraints, were the most significant factors in improving the intentions of mothers towards teaching tooth brushing practices. Knowledge was positively associated with attitude and perceived behavioral control. 22
Collaboration between primary care providers and nurses and dental services creates opportunities to initiate preventive oral care in children. With training, nurses can perform oral health screening and risk assessment, fluoride varnish applications, and timely referrals to dentists. A study examining dental personnel referrals by primary care nurses indicated that referrals were appropriate but that over half of the children at risk of developing caries were not referred, suggesting that nurses need more competence to identify children in need of early oral health prevention. 23 A separate study determined that current approaches, with predominantly dental care providers educating low-income parents on prevention interventions, are insufficient. 24 Integrating science-based oral health preventive care into nursing undergraduate programs could improve the oral health literacy of nurses and their confidence in providing oral health care.
Materials and Methods
The purpose of this study was to evaluate the relationship among parent-reported children’s oral health status, an oral health assessment conducted at a school-based dental program, and a tooth decay risk score. As part of a service learning activity incorporated into a child health course, undergraduate nursing students examine preschool children for oral hygiene and apply fluoride varnish. The program was implemented in preschools in Northwest Arkansas where a high percentage of children qualify for free and reduced school meals. Senior BSN students complete an online module on Caries Risk Assessment, Fluoride Varnish and Counseling that is part of the Smiles for Life Curriculum. User competencies are measured through posttests at course completion. Students are required to score 80% or higher to receive the course certificate and participate in the program. Informed consents were taken from the participants after explanation of purpose of study.
Design and Sample
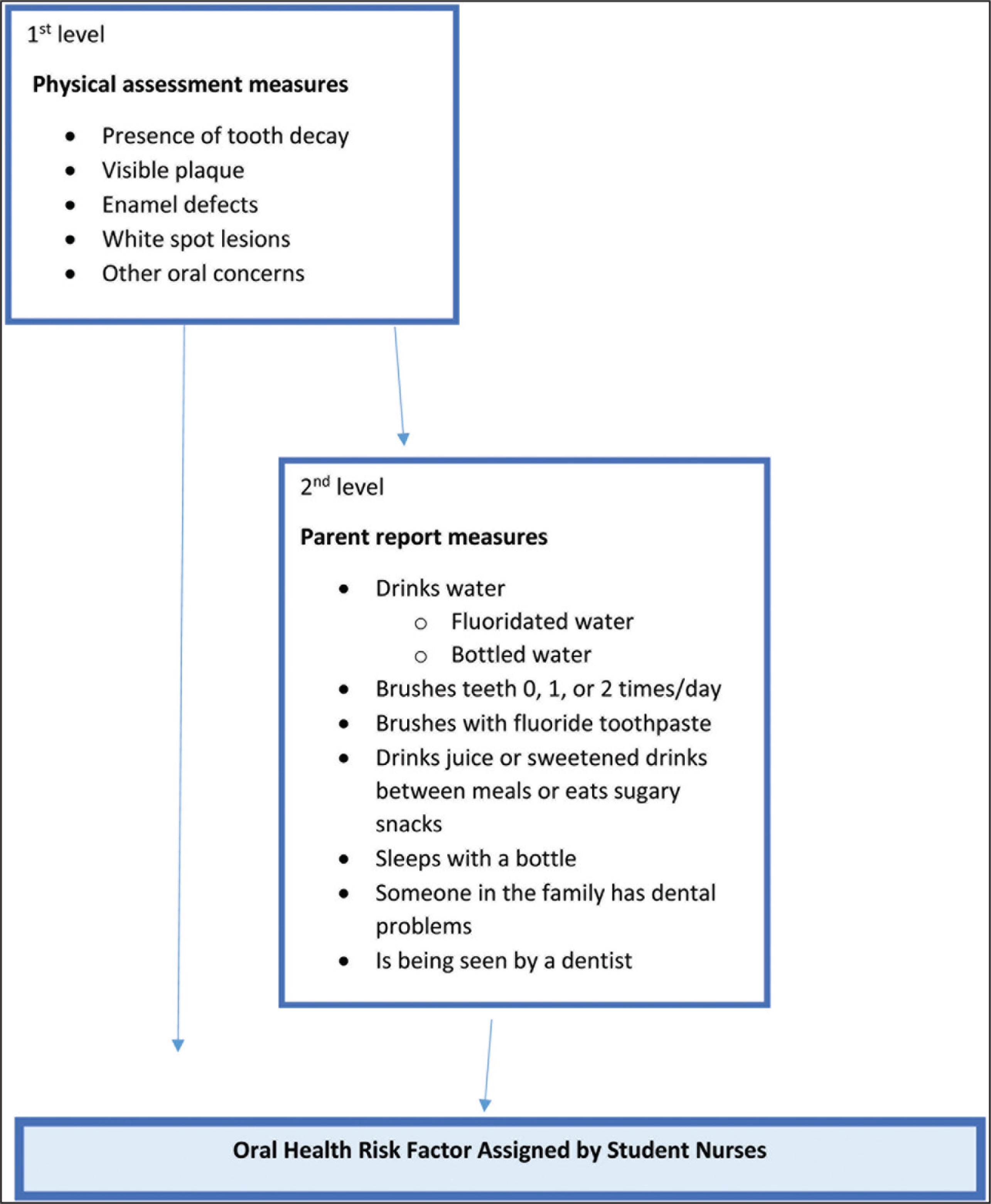
After obtaining institutional review board approval, data for the study was obtained from a parent-completed permission form with yes or no questions regarding tooth-brushing frequency, sugar intake, familial dental problems, and whether the child is being seen by a dentist. A second data set was obtained from an assessment completed by the student nurses and includes the presence of tooth decay and/or fillings, visible plaque, enamel defects, white spot lesions, swelling, complaints of pain, and whether the child was referred to a dentist for urgent care. Based on the data, student nurses assign a tooth decay risk score.
Measures
Dental Caries
The dental assessment performed to determine the presence or absence of dental caries followed methods and criteria established by the training program offered by the Arkansas Department of Health Office of Oral Health that is part of the Smiles for Life oral health curriculum.
Child Oral Health Behavior
The permission form sent home to parents/guardians included the following questions: My child brushes teeth twice a day, my child brushes teeth once a day, or my child does not usually brush their teeth; When your child drinks water, is it usually tap water from the sink or fridge door (Yes, No usually drinks tap water, or No my child does not usually drink water); Do you brush your child’s teeth at least once a day using toothpaste with fluoride? (Yes or No); Does your child drink fluoridated water? (Yes or No); Does your child drink juice or sweetened drinks between meals or eat sugary snacks? (Yes or No); Does your child sleep with a bottle filled with milk or drinks other than water? (Yes or No); Have you or anyone in your family had dental problems? (Yes or No); Is your child being seen by a dentist? (Yes or No).
Risk Assessment Score
Based on their assessment, student nurses assigned a tooth decay risk score of 1, 2, or 3 representing low, moderate, or high risk.
Data Analysis
A bivariate analysis with a Chi-square value was applied to compare the presence of tooth decay with each independent variable reported by the parent and a P value < 0.05 was considered statistically significant. A multiple regression analysis was conducted to predict the overall tooth decay risk from the student nurse who performed oral assessment. The multivariate regression model followed a hierarchal approach with determinants characterized into two levels: first level—physical assessment measures and second level—parent report variables. The conceptual framework depicted in Figure 1 was used for the multivariate analysis. Analyses were performed using SPSS software, version 25 (IBM SPSS Statistics).
Conceptual Hierarchal Framework for Oral Health Risk: Multivariate Data Analysis
Results
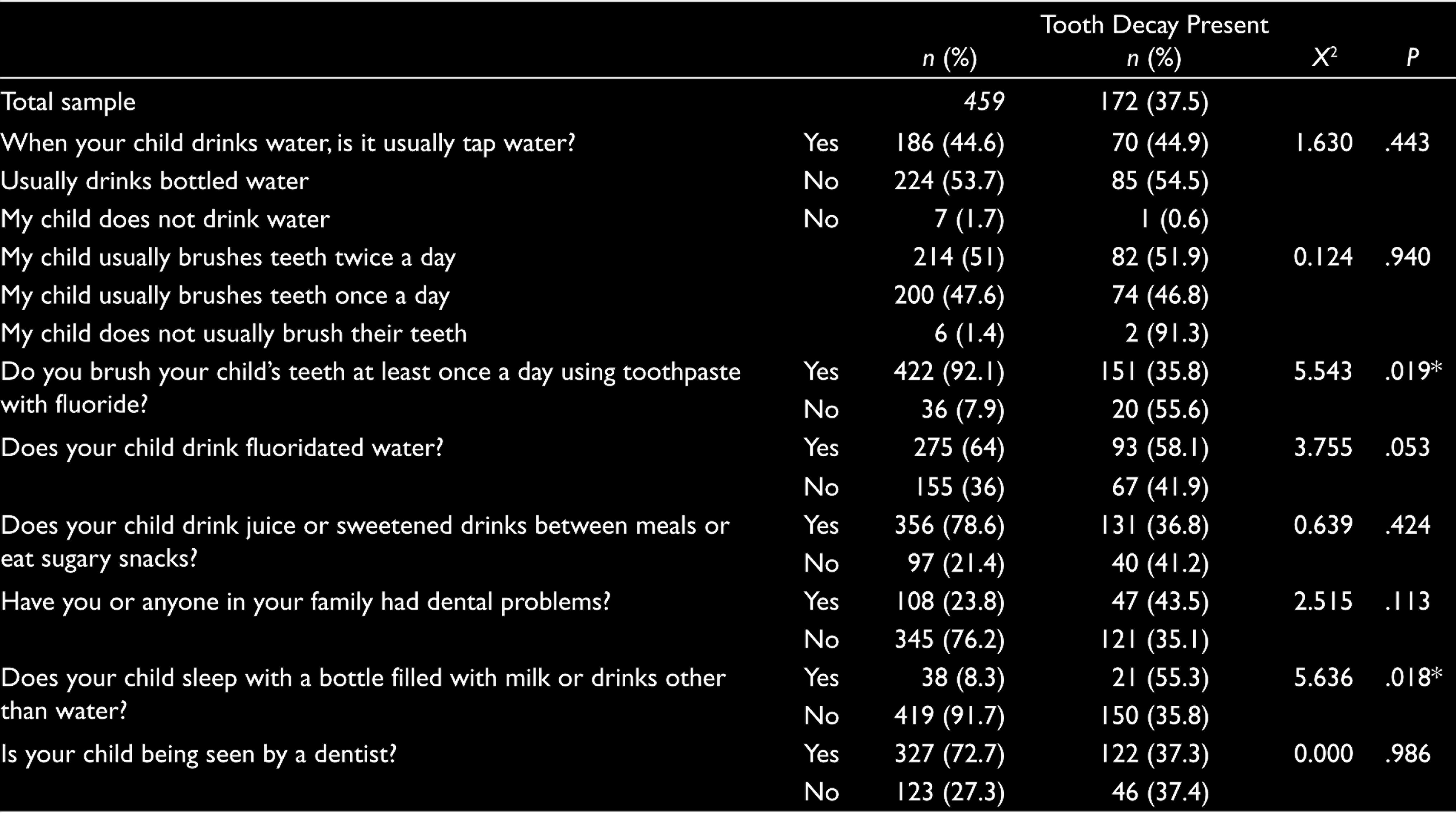
Around 92% of the parents reported brushing their child’s teeth at least once a day using toothpaste with fluoride; 60% reported that their child drinks fluoridated water; 77% reported that their child drinks juice or sweetened drinks between meals or eats sugary snacks; and 8% reported that their child sleeps with a bottle filled with milk or drinks other than water. Around 71% reported that their child was being seen by a dentist.
There was a statistically significant difference in the presence of tooth decay between children whose teeth were brushed at least once a day using toothpaste with fluoride and those whose were not and between children whose parents reported that they slept with a bottle filled with milk or drinks other than water and those who did not (Table 1).
Chi-square Results
A multiple regression analysis was conducted to predict the overall tooth decay risk from the student nurse performed oral assessment. Overall, 9% of the children were assessed to be at high risk for tooth decay, 26% at moderate risk, and 66% at low risk. Results of this analysis indicate that the physical assessment measures accounted for a significant amount of the risk variability, R2 = 0.55, F(5, 317) = 76.2, P < .00. A second analysis was conducted to evaluate whether the parent report measures predicted tooth decay risk over and above the assessment, R2 change = 0.029, F(7, 310) = 3.010, P = .00. These results suggest the parent’s reports, although significant, offer little additional predictive power beyond that contributed by the screening when student nurses assigned a risk score.
Discussion
Results of this study indicate that while children and their parents or guardians are engaging in appropriate preventive oral health practices, implementation of recommendations is not optimal. About half of the parents reported brushing their children’s teeth less than twice a day, the majority reported that their children consumed sugary food and drinks, and 40% reported that their child did not drink fluoridated water. Results also indicate that the nursing students based assignment of risk status and need for referral on clinical findings and that biological and social risk factors reported by parents/caregivers were not as useful in predicting tooth decay risk. Referral of 21% of children to dental services indicates under-referral given that 27% of the parents reported that their child was not being seen by a dentist and 49% had not established recommended tooth brushing practices in early childhood.
These findings confirm the need for a social determinant of health (SDOH) perspective to better inform oral risk assessment and interventions to address oral health disparities. 25 Fisher-Owens et al. proposed a broader framework that incorporates predictors at the child, family, and community level along with biologic and dietary influences when researching oral health in children. 26 At the child level, physical and demographic attributes such as low birthweight, initial feeding practices such as breastfeeding, and early childhood experiences that affect subsequent well-being and coping skills influence health outcomes. At the family level, family composition, immigration status, socioeconomic status, and family health practices can have positive or negative effects on oral care. Community level influences include neighborhood safety, the presence of oral health promotion campaigns, the dental care system’s degree of diversity and participation in Medicaid, and the availability of primary care. 26
Our study had limitations. The study sample was a convenience sample and the results may not be generalizable. The data was obtained from parent permission forms that were not intended for health surveillance. Measures are based on parents’ self-reports and are susceptible to social desirability response bias. Because the parent sample size is small, parental reports should be interpreted with caution.
This study provides foundation for further curricular development. Next steps include emphasizing an SDOH framework such as the one proposed by Fisher-Owens et al. to describe factors leading to oral health disparities in the nursing curriculum. Plans are to continue the dental service learning project with a more comprehensive caries risk assessment (CRA) tool that includes biological and social ECC risk factors. Although no validated CRA tool exists, the most commonly used tool is available from the AAP and is included in the Smiles for Life curriculum. 27 This tool will also be used by students to develop a prevention plan that can be shared with parents. Faculty is also developing a method to evaluate the extent to which the service learning assignment meets course outcomes. Course evaluations and reflective journals will be used to evaluate student’s awareness of community needs, ability to work with diverse populations, and development of effective strategies to promote oral health in young children.
Oral health screening of children with early detection of risk and referral to dental services can be effectively carried out by nurses and nursing students. Preschool and elementary school age children regularly participate in vision and hearing screening. Adding an oral health screening with fluoride varnish application can increase access to preventive dental care. 28 Applying an SDOH perspective to education about oral health could improve nursing students’ competency to identify children in need of early intervention.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by a grant from the Delta Dental Foundation.