
Abstract
Objective:
To identify African-American seniors’ perceptions of the barriers and facilitators to their dental care.
Materials and Methods:
In this cross-sectional qualitative study, we conducted in-depth interviews with 16 community-based, self-identified African-American seniors from March 2017 to August 2017 in Oregon. We coded data in ATLAS.ti and used thematic analysis to identify emergent themes within the social ecological framework and a cross-case comparative analysis to explore variation by participant characteristics.
Results:
Regardless of dental insurance status, cost and perceived urgency of treatment were the primary drivers of participant’s ability and interest in seeking dental care. Participants identified four solutions to improve oral health care in African-American seniors: affordable/free care and vouchers for dental work, better oral health education at a younger age, onsite community dental services, and navigators who can educate patients about insurance and dental providers who see low-income patients.
Conclusions:
Oral health decisions by African-American seniors were primarily driven by cost and perceived urgency irrespective of insurance coverage. Affordable dental care, early intervention, on-site services, and navigation may help to address key barriers and reduce oral health disparities faced by African-Americans.
Introduction
The number of American seniors (65 years and older) is expected to nearly double from 43.1 million in 2012 to 83.7 million in 2050, contributing to more than a fifth of the nation’s population. 1 Among this older population, African-Americans represent the greatest number and proportion of minority elders, and their numbers are expected to rise dramatically. 2 It is estimated that by 2020, when many of the baby boomers become eligible for retirement, the population of elderly African-Americans will have increased 121.2% since 1990 population levels, almost twice as much as the projected 64.7% increase among older White Americans. 3
Although the oral health of Americans has improved tremendously over the past 30 years, African-Americans experience numerous challenges accessing dental care which have a great impact on their oral health. 4 While seniors overall are at risk to various oral health ailments, 5 African-American seniors experience numerous other health disparities compared to their white counterparts. For example, African-American seniors are at a higher risk of developing oral health pathologies, including periodontitis, 6 tooth loss, 7 and caries. 7
The oral health status of African-Americans can be viewed through a social-ecological lens and may be influenced by cultural norms, residential segregation, discrimination, and racism. 8 In a recent study, researchers identified various determinants influencing oral health disparities among African-American men, including insurance coverage, treatment costs, and access to care. 9 While age may be one factor that influences oral health in African-American seniors, other factors include socioeconomic status, 10 cost barriers, 10 and oral care training among caregivers. 11 When compared to dental provider perceptions, African-American seniors are significantly more likely to perceive their own dental conditions as non-problematic. 12 Yet, they have the greatest unmet dental needs and have the lowest dental care utilization compared to other ethnic groups. 13 This may be in part due to the notion that African-American senior perceptions of their oral health influence their dental care seeking behavior. 14
Currently, a plethora of oral health educational materials provide information targeted towards multi-ethnic and older adult populations, 15 however, few resources are targeted towards African-American seniors. There are very limited studies that test the effectiveness of existing oral health educational materials developed for African-American seniors. 16 Despite the recent evidence on the underlying pathways for oral health disparities among African-American men, 17 several knowledge gaps remain in relation to African-American women, who may have different barriers to their oral health care. 18 Furthermore, limited studies involve a holistic understanding or use a qualitative approach to explore the various causes of these oral health disparities among African-Americans. Those studies that do exist involve children 19 and adults20,21 or examine only one aspect, i.e., dental care access problem among African-American men.
Therefore, the overall objective of this study was to identify African-American seniors’ perceptions of the barriers and facilitators to their dental care. With the qualitative design of our study, it provides more exhaustive view on oral health barriers and facilitators exclusively in African-American seniors from consumers’ perspective. The long-term goal is to inform development of community-driven culturally appropriate interventions to reduce oral health disparities in African-American seniors.
Materials and Methods
In this cross-sectional qualitative study, the multidisciplinary study team conducted in-depth interviews with self-identified African-American men and women over the age of 65. The study used the grounded theory method with two basic principles: (a) questioning rather than measuring and (b) generating hypotheses using theoretical coding. 22
Sample Selection
Participants were recruited using multiple methods, including distributing recruitment fliers at community health fairs, churches, senior centers, community centers, primary care clinics, dental offices, and senior residential facilities in the Portland metro area. Eligible participants were African-American, 65 years or older at the time of the interview, capable of making cognitive decisions, and residents of Oregon. The study team also used a snowball sampling technique, 23 which asked interview participants to recommend other African-American seniors who met study inclusion criteria. Interested participants completed a brief intake survey with questions about insurance status, annual income, and education level. Participants were asked to subjectively select their social status in the community using the MacArthur Subjective Social Status Scale 24 and to complete the Mini-Cog test, a brief test of cognition. 25 Participants that met inclusion criteria were invited to take part in a one-on-one, one-hour semistructured interview at a central community location or at the researcher’s office.
Data Collection
From March to August 2017, a research assistant trained in qualitative methods (SH) obtained informed consent and conducted interviews using a semistructured interview guide. The interview guide was first pilot-tested and refined with the sample of African-American seniors at the 24th Annual Event of African-American Wellness Village organized by African-American Health Coalition in Portland, OR. The interview guide included a definition of oral health and asked questions about participant’s oral health history, personal history, current oral health, and where they sought dental care. Interviews were performed at a mutually agreed site by the interviewer and interviewee in and around Portland, OR. Each interview was audio recorded (average length 35 min), professionally transcribed, de-identified, and transferred to ATLAS.ti (Version 7.5.18) for data analysis and retrieval. Participants received a $25 gift card once the interview was completed. We enrolled 16 African-American seniors, out of which 10 participants (63%) were recruited using snowball sampling.
Data Analysis
We conducted interviews and analyses concurrently, monitoring for data saturation, the point at which no new findings emerge. 26 Analysis began after three months of data collection and assisted the study team in determining if saturation had been met. We used the six phases of thematic analysis to identify emergent themes: familiarizing with data; generating initial codes; searching for, reviewing, then defining, and naming themes; and producing a scholarly report. 27 The research team read early transcripts and defined a preliminary coding scheme. Transcripts were coded independently or by groups of two study team members. Over the course of multiple analysis meetings, the full study team met to discuss emergent themes and to resolve discrepancies through consensus. 28 During these meetings we organized emerging themes according to levels of the social–ecological framework: individual, relationship, community, and societal factors. 29 We then iteratively refined themes and produced a summary report.
Results
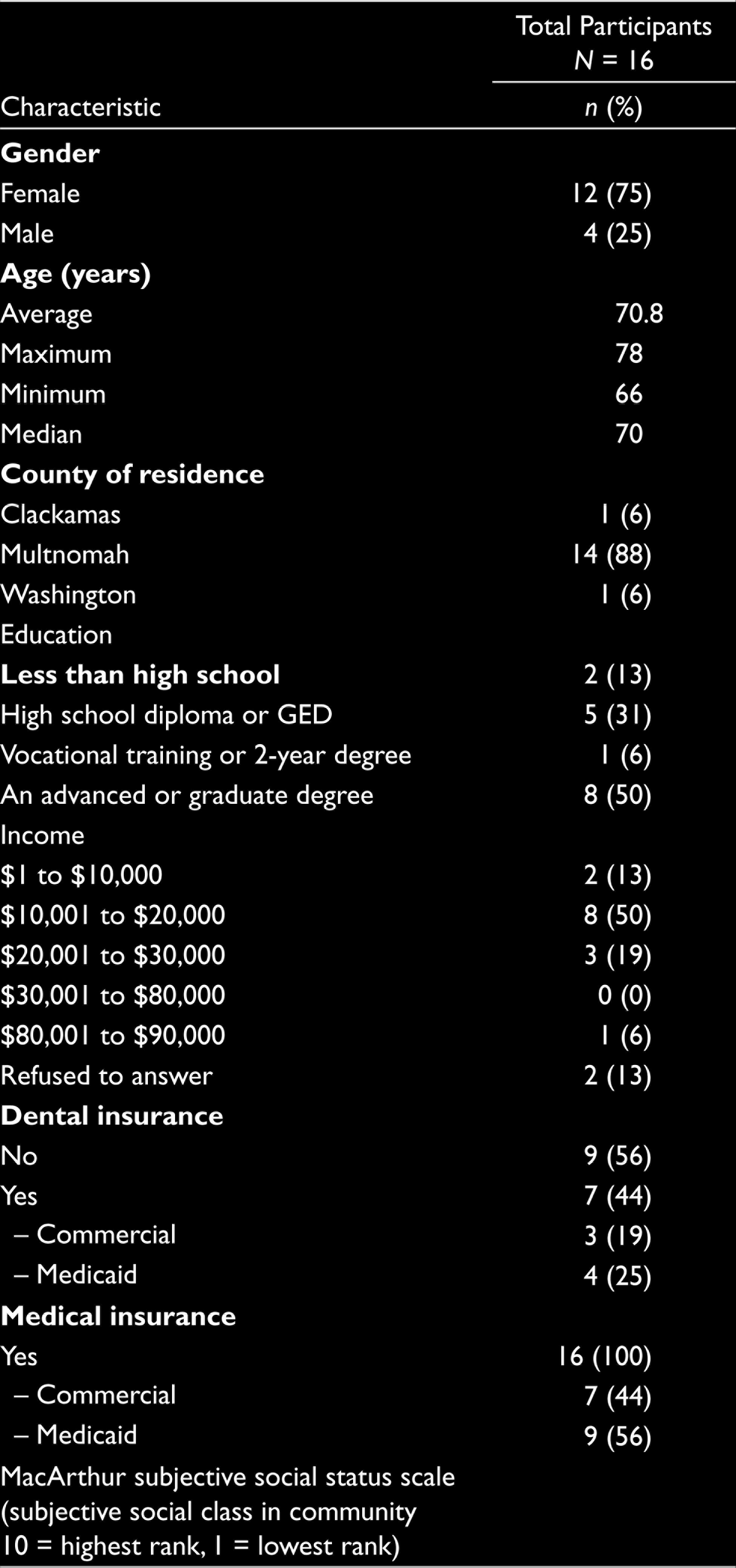
Demographic characteristics of the 16 participants are summarized in Table 1. Mean participant age was 70.8 years (range: 66–78); 75% (n = 12) were females. All participants had health insurance through Medicare (n = 16, 100%; dental insurance is generally not included with Medicare and, therefore, it is an additional product that must be purchased and managed by the recipient). Nine participants (56%) had no dental insurance; the seven participants with dental insurance had it through Medicaid (n = 4, 25%) or through commercial plans (n = 3, 19%). Mean annual income was $32,000 across the participants; eight participants (50%) made $10,000 to $20,000 per year.
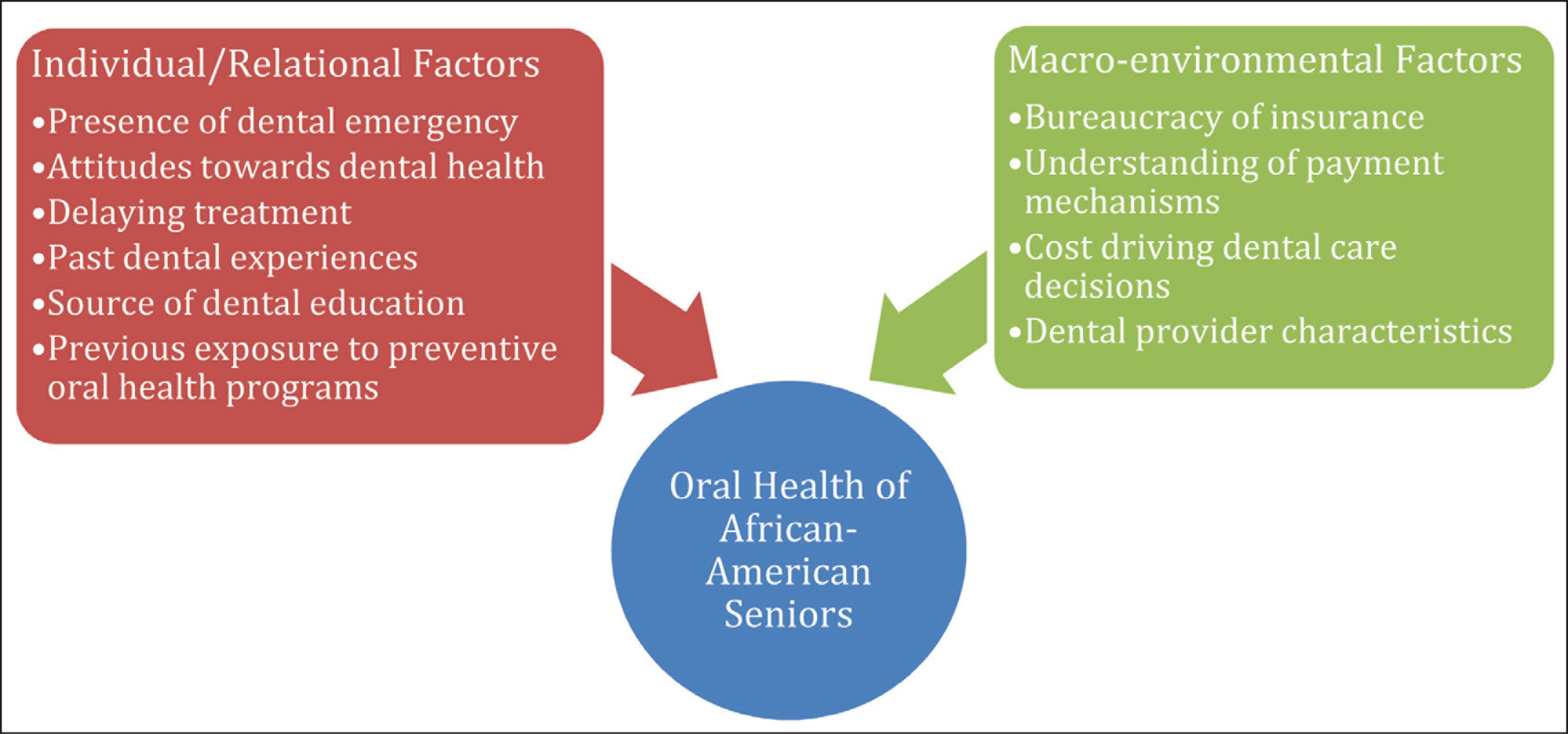
Around 10 themes that shaped dental care seeking behavior and obtaining dental care for African-American seniors emerged within two broad clusters related to (a) individual and relational factors and (b) community and societal (macro-environmental) factors. These themes are summarized in Figure 1 and have been described in detail below.
Individual and Relational Factors
Participants described learning their dental care routines through various avenues. Mothers were often credited with teaching participants about regular dental care at home, home remedies for oral pain, and when to seek dental care.
I had a horrible experience with a toothache. … My mother introduced me to a technique about fingernail polish. What it is, it just coats the tooth. So, I stopped going to the dentist. I’d just go numb …. Numb myself up real good…. (P11)
Participants also fondly recalled school programs, especially assemblies, where they received information on fluoridation and brushing. Dental professionals also taught the participants as children about proper home care, including teeth brushing and flossing:
The [hygienist] told me, … if you brush your teeth, brush your teeth with a toothbrush going like this [up and down] and make sure you floss really good. (P16)
Participant Characteristics (N = 16)
Factors Across the Social Ecological Spectrum Affecting Oral Health of African-American Seniors
Many participants reported that when they were children, the dentist was “expensive” and visits were not regular occurrences. Childhood visits to the dentist were often for dental emergencies (e.g., abscess, tooth ache, and broken teeth), rather than for preventive care. These influences in childhood shaped participant’s attitudes and oral health behaviors as adults. Many participants commented that regular brushing was enough of a preventive measure, rather than annual or bi-annual dental cleanings as recommended by national programs. Those that sought preventive care set a priority on their oral health. Other prevailing attitudes included the belief that the loss of one’s teeth, and even, in some cases, serious dental disease was inevitable. One participant dealt with this perceived reality by getting all her teeth extracted:
… it’s been real important that I take care of my teeth…. It’s really been a high priority for me because these teeth have got to last. (P1) I don’t want to keep running back and forth … [to the dentist]. So, I had [my teeth] pulled. I didn’t have no abscess or nothing. I just wasn’t going to be bothered with trying to save 11 teeth on the bottom. … so, I just had them pulled. (P9)
While many participants indicated that they did not pay attention to their oral health until there was a problem, others delayed treatment before finally going to the dentist for esthetic reasons. One participant reflected on the parental influence on their care-seeking behavior:
My mom had a mouth full of gold. And my father had a mouth full of gold. My grandmother had a mouth full of gold so, you know, they would, they were some of my heroes so I’ve, you know, I liked how it looked on them, and so I’ve gotten some. (P15)
Participants sought oral health care due to pain and problems chewing with or without dentures. Although the majority of participants did not visit the emergency room for dental issues, one participant reported visiting the emergency room 10 times for dental-related problems. This seemed to be a stop-gap measure taken to address pain during nonbusiness hours, before visiting a dentist to address the oral health issue.
They gave you some pain medication to last you through the [weekend], ... they’d see if I had a hole-And stuff like that at the emergency room. And see why I was paining so bad and my gums were maybe infected they would give me antibiotic. So, I could start on the antibiotic before the dentist ... got to it. (P13)
Community and Societal (Macroenvironmental) Factors
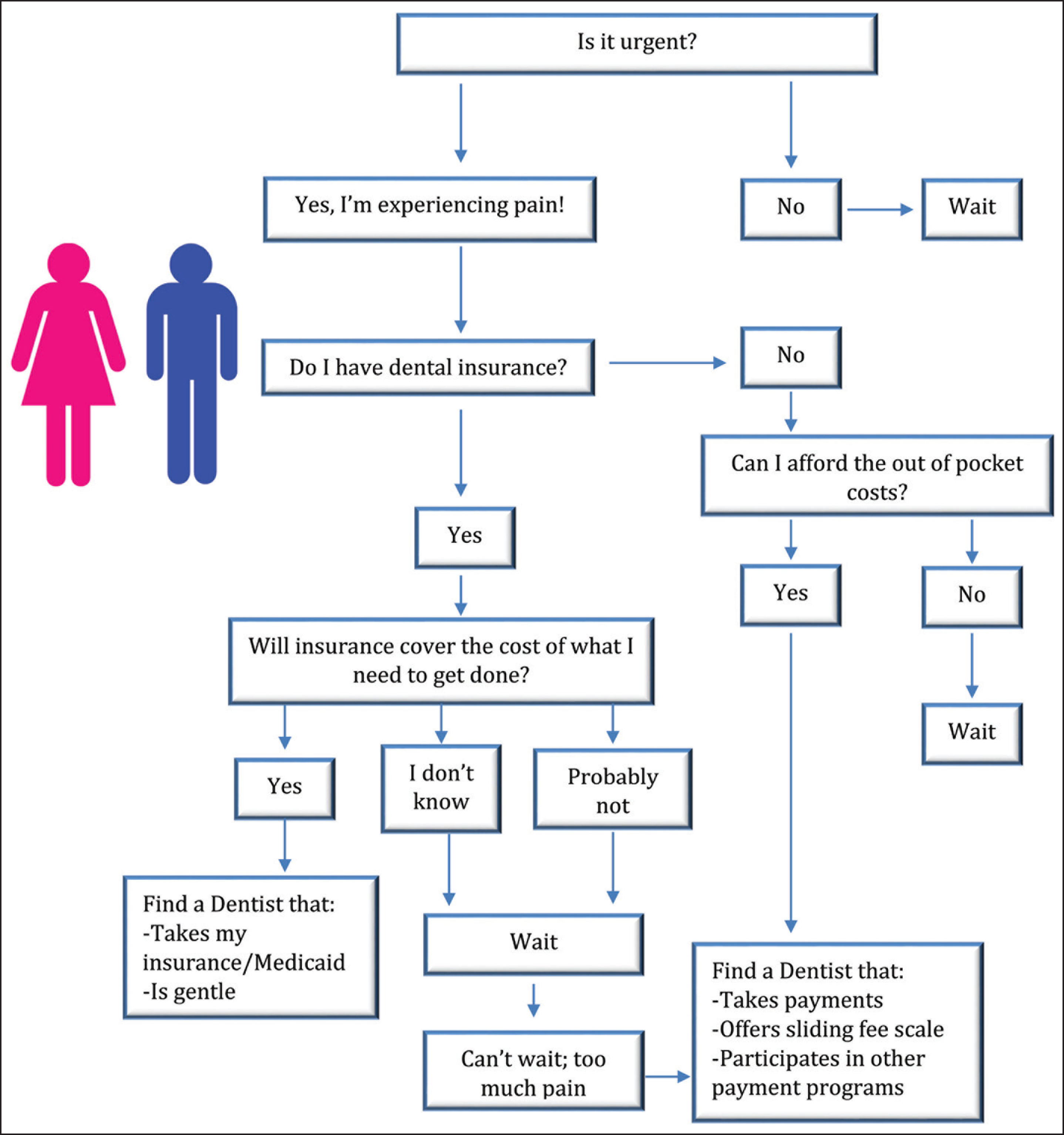
Community-level and broader-scale social factors that influenced the cost of treatment were macroenvironmental factors that played a key role in oral health behaviors of African-American seniors. As displayed in Figure 2, these macroenvironmental factors interacted with individual attitudes such that the prevailing indicator of whether someone would visit a dentist was determined by the intersection of affordability and necessity. Participants often had to consider if they could afford the out-of-pocket costs, whether their dental problem was an immediate issue, and whether dental care was more important than other essential expenses, such as a utility.
Well, it would be fine if you can afford it and if you can find a dentist that would take your coverage.… I’m paying $40 a month that really, I can’t afford … seniors are on a fixed income. We can’t afford this extra money, out-of-pocket money. (P3)
Intersection of Affordability and Necessity for Dental Care in African-American Seniors
Some participants could afford to pay out of pocket for preventive maintenance, such as cleanings. However, once other services, such as radiographs, restorations, or crowns, were required, they sought dental providers who could offer these services at a lower cost, take Medicaid or payment on installments, or offer a sliding fee scale. Participants that did not have insurance coverage would delay treatment until they found a mode to pay for these fundamental procedures.
A lot of things I want to do and I can’t do it because I live on a fixed income so I just don’t do it. You just wait, wait, until you get the money to do it. (P4)
I’m able to get to my dentist, it’s just being able to pay him. (P1)
Participants who had dental insurance (both Medicaid and Commercial) found difficulty managing and tracking payments between the dental office for services and the insurance company. These activities added to the frustration of having to pay out of pocket for services not covered by the insurance plan. The major barriers to seeking care among those with insurance were the monthly cost to carry the insurance policy, the out-of-pocket cost, and the cost to meet the deductible. Regardless of insurance coverage, all participants indicated that cost was the main driver determining where, when, and if dental care services were sought.
While some participants who had access to dental insurance during their working years used it regularly, others were just as likely to not use it. Those that did take advantage of employer-sponsored dental insurance did so in order to complete all their treatment while they were still covered. Participants were more inclined to utilize dental services if the insurance was employer paid and treatment was affordable. Interestingly, these participants also believed that dental work is an elective service rather than a necessary, continuing service.
When I retired I decided that I wasn’t going to be able to have dental insurance, I told that to my dentist … He said, “Okay, let’s do everything that you might likely need to have done while [your employer] is paying.” (P1)
The attitudes and characteristics of the dentist were imperative to the participant’s trust and comfort with their provider. All subjects indicated that the most important characteristic they would like to see in a dentist is empathy and gentleness. Although some participants would be more comfortable going to African-American dentists, they prioritized a dentist’s competency and trust. It was also important for the dentist to be knowledgeable and confident. All but one subject indicated that the dentist’s race and ethnicity did not determine whether they would patronize a dental practice.
A person that has empathy because they know everybody can’t take needles and pullings and all that. So, somebody, a dentist, that would be a comfort, to have empathy enough to talk to the person to let them know what they’re gonna do, what they might experience, and what they’ll do to help them make it more comfortable. (P10)
I wasn’t necessarily looking for a dentist because they were African American. I’m just looking for a good dentist. (P1)
Participant Solutions to Improve Dental Health Care
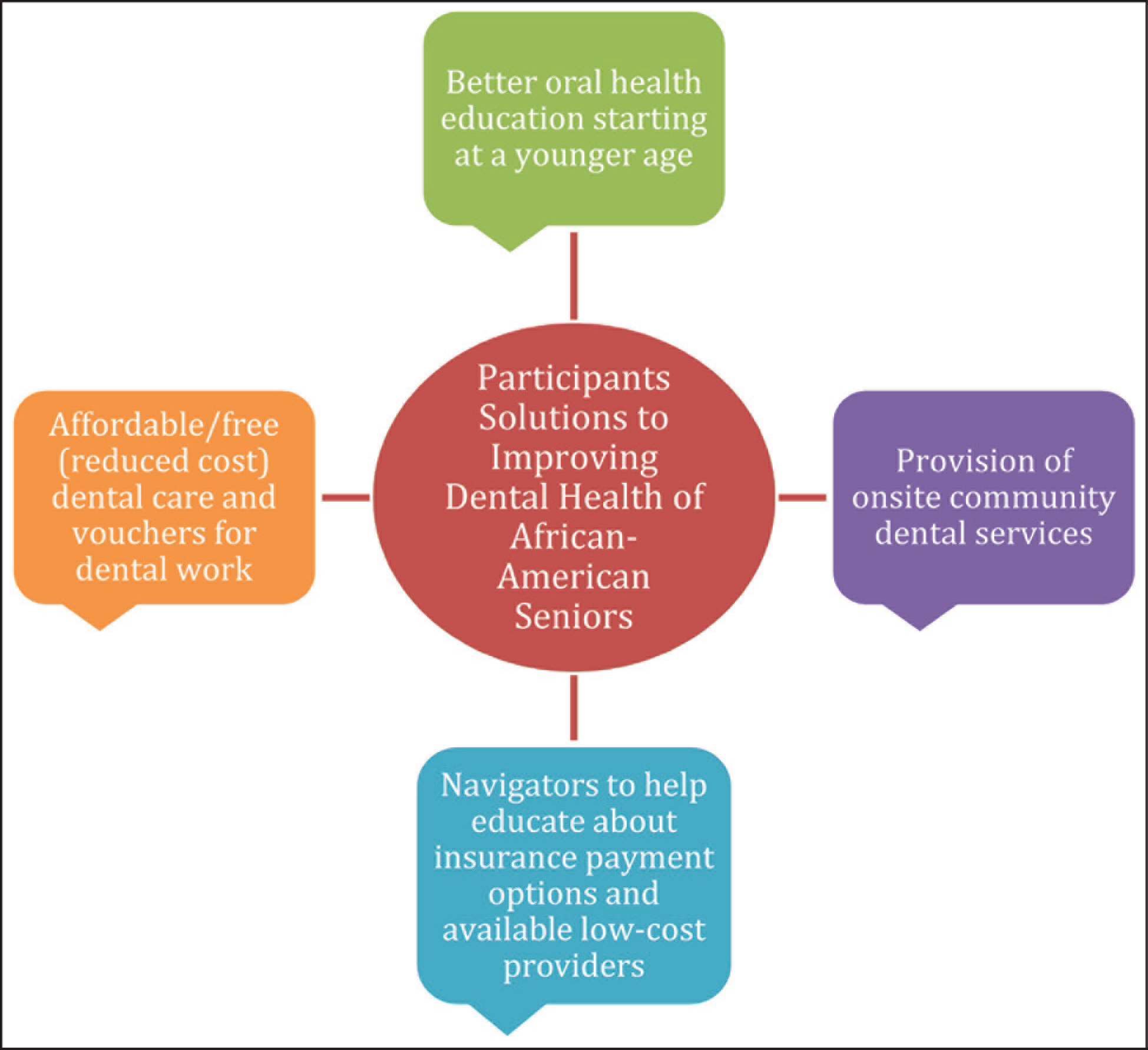
Figure 3 summarizes the four main focus areas participants suggested to improve the oral health of African-American seniors. One subject suggested that basic dental services should be free or very inexpensive. Most participants felt that dentists were widely available, but it was difficult to come by dentists who offered services at reduced rates or took Medicaid. One participant recommended dental treatment costs be included as a tax break and reduced in accordance to other essential bills.
Participant Solutions to Improving Dental Health of African-American Seniors
I would say also to have more of a bigger chunk of tax write off for your dentistry as in like medical.… I think, and maybe have maybe voucher for dentistry, for your dental care, for those who can’t afford to pay that right now... I think the voucher should as the cost of living goes up, the voucher should give you dental care…. should go up at the same time, at the same percentage. (P8)
Many participants felt the need for better oral health education at their current age as well as a younger age. They suggested incorporating more dental education in schools through use of pamphlets for kids and their parents. One patient reported education would help them set a higher priority to their oral health.
Participants discussed the benefit of having dental professionals go to senior centers to provide them services, to educate them, and to guide them to the proper treatments. Participants would also like to see someone in a “navigator” type role to help seniors find low-cost dental providers, to understand the ins and outs of dental insurance, and to provide a list of dentists who accept alternative payment methods.
… if I don’t have someone to explain things to me and to show it to me then ... then I don’t know what’s available for me and … So, it would be nice to know if there was somebody looking out for you, to let you know this is something that you can do. (P3)
Discussion
This study gave rise to multiple notable findings regarding the underlying factors to oral health care seeking behaviors among African-American seniors. Specifically, our study determined cost as a major barrier in seeking dental care, regardless of whether the participant was covered by insurance. Our study found that in addition to insurance coverage and cost of care, African-American seniors reported that navigating through insurance policies and payment plans, the oral hygiene education they received in childhood, provider characteristics, and perceived dental urgency were factors in their barriers to dental care. Moreover, these various socioecological factors seemed to influence their recommended solutions for improving the dental health of African-American seniors.
These findings confirm those determined by Manksi et al, who found that African-Americans with dental insurance coverage and high incomes still had lower rates of dental care utilization than their White counterparts. In a recent study by Thompson et al, 10 researchers found that those who reported worse oral health also reported being more likely to avoid the dentist due to financial barriers and were more likely to decline recommended treatment. This may help to explain our study participants’ behavior to not seek care from a dental provider, despite having employee-sponsored insurance.
As demonstrated by Akintobi et al 9 and Schrimshaw et al, 21 the major themes identified in our study, such as insurance coverage and treatment costs, strongly influence participant decisions to seek dental care. While Akintobi et al identified transportation and not knowing where to go for dental care as significant issues to dental care utilization among African-American men, the African-American seniors in our study, majority of who were women, reported that the cost of treatment was the primary barrier. Education, like cost, influenced multiple themes across the individual and macroenvironmental clusters, which led to confusion and frustration surrounding dental insurance policies and navigation. In addition, dental education influenced participant decision to set a lower priority to oral health.
Our findings suggest similar solutions to reducing oral health disparities among African-Americans as Hoffman et al. 17 Study participants confirmed that improving knowledge and attitudes through dental education at an earlier age, will improve behaviors and attitudes toward their oral health as adults. However, patient care seeking behavior does not solely depend on insurance coverage or dental education. Our findings demonstrate that provider’s race may not have as strong as an influence on provider–patient relationships of African-American patients as previously thought. 30 Rather, our participants preferred to seek care from dentists who were empathetic, competent, and trustworthy. These are characteristics that can be encouraged in dental students and active providers to strengthen their provider–patient relationships, as well as serve as models for future dentists to improve their practice of dentistry.
There are some limitations to the present study. First, our study engaged a small number of African-American seniors in one state, which limits the generalizability of results. To address these concerns, we used robust standards for qualitative research, such as by monitoring for data saturation and engaging a purposive sample, to ensure diverse perspectives were representative. Second, as a convenience sampling technique, the snowball sampling method may have resulted in a sample population, who are members of the same social communities and who have similar values, beliefs, and socioeconomic status. This could have led to an agreement among responses. Although we used this sampling approach, we were able to include seniors that represented a diverse spectrum of social and economic communities.
Conclusion
As data are currently lacking on oral health status of African-American senior population within Oregon, our study identified specific problems related to individual and social factors that influence oral health care behaviors. We found that oral health decisions by African-American seniors were primarily driven by cost and perceived urgency irrespective of insurance coverage. These findings may lead to critical initial steps in eradicating barriers and strengthening facilitators to African-American seniors’ dental care. As more dental providers become willing to provide free dental educational and care services, we may see a greater overall improvement to oral health and oral health perceptions among African-American seniors. The solutions to reducing oral health disparities proposed by the participants, reduced costs of care, better oral health education, on-site community dental services, and navigator roles may serve as a model for dental providers, researchers, and other stakeholders to establish the most effective preventive interventions for this high-risk subgroup as well as other vulnerable and underserved populations. Future research activity should enhance these study findings through community-based interventions, educational events, and patient engagement organizations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
We would like to thank Medical Research Foundation (GSODO0085A) for funding this project as well as the participants of this study.
Semistructured Interview Guide for interviewing African-American Seniors
The questions below are the general topic areas we will explored with interview participants. These questions will were modified in light of what was learned during the interview and to fit the expertise of the interviewee.
Thank you for participating in this interview. We are talking with you today because we are interested in finding out about your experience getting dental care. We are interested in learning more about what prevents you from getting dental care, and what helps you get dental care, and if you have any recommendations for how to improve dental care in your community.
Before we get started, I’d like to take a few minutes to review the study consent form. (distribute and review consent form, get signatures). Do you have any questions about the study before we begin?
As mentioned in the consent form, we’d like to record this conversation. Is it OK to turn the recorder on? (if yes start audio recording and get verbal consent on the audio recording).
Potential Prompts:
What does it mean to you have bad dental health? What does it mean to have good dental health?
In our study, we’re thinking of dental (or oral) health as an overall picture of the quality of health in your mouth. This includes your teeth, gums, but also, the palate, the soft tissue lining of the mouth and throat, the tongue, salivary glands, chewing muscles and upper and lower jaws. 1 …. Thinking about that, I’m going to ask you some questions about your dental health.
Potential Prompts:
Why? Are you in charge of helping anyone else with their dental health? If yes, how has this impacted your own dental health?
Potential Prompts:
How did you learn to take care of your dental health?
How has what you do for your dental health changed over time?
Potential Prompts:
How long have you had these problems?
What are you doing to address them?
Potential Prompts:
Positively; negatively? Probe for each condition they talk about.
Potential Prompts:
Potential locations of interest (ask about each if needed): Dentist, Primary Care Provider, Emergency Room, someplace else? What leads you to seek care at these locations (e.g., Price? Location? Characteristics of the provider?)
You told me about the place(s) where you get care; I would like to explore more about where you currently get dental care; I’m interested in learning a little more about the(each) setting(s), how you feel about the provider, and what would make your experiences better.
To what extent do you have access to his/her dental practice?
Is his/her practice free standing or a group practice?
Is it near bus line?
Is it near mall?
How old is his/her dental practice at the current location?
Is it with latest technology?
Now, I’d like to understand what might help improve your dental care or make access to dental care easier for you.
Potential Prompts:
Consider asking about the role of fear/past experience, cost, racism, access, provider characteristics (however, let the participant drive this question – what do they bring up? Probe for details.) Is this because there are no African American dentists available?
Potential Prompts:
Consider asking about the role of fear/past experience, cost, racism, access, provider characteristics (however, let the participant drive this question – what do they bring up? probe for details.) Is this because there are no African American dentists available?
President Obama signed the Patient Protection and Affordable Care Act (ACA) on March 23, 2010. The law was intended to lower the cost of health care and coverage for all Americans and to give more rights to help insured patients.
Potential Prompts:
Did you change your dental coverage due to ACA?
Did that lower your dental care treatment spending?
Potential Prompts:
When you think of your family and close friends, what might help your family or friends improve their dental health? What specific changes might help African American seniors improve their dental health?
Thank you for your time and input on this topic. We would like to provide you with a gift card in appreciation of your time (complete documentation and get signature for the receipt of gift card).