
Abstract
Aim:
Due to the common nature of oral and dental problems, awareness needs to be improved, expanded, and maintained. The aim of this study was to determine the oral and dental health knowledge levels of students, many of who would be teachers of the future, in this health field, and to help them work toward the elimination of the identified deficiencies.
Materials and Methods:
This cross-sectional descriptive study involved 475 students from the Erzurum Ataturk University dentistry, medicine, pharmaceutical sciences, nursing, and education faculties. Data were collected through a questionnaire by random stratified technique, investigating participants’ demographic characteristics and oral health knowledge levels.
Results:
We observed that 77.3% of students correctly answered 15 or more out of 31 questions addressing levels of knowledge of oral and dental health. This figure was 100% for students in the dentistry faculty and 56.3% for those in the education faculty. The difference between faculties in terms of students correctly answering 15 or more questions was statistically significant (P < .001). A statistically significant difference was also determined between the faculties in terms of students’ sense of competence in oral and dental subjects (P < .001).
Conclusion:
In the light of the data obtained, since prospective health care professionals and teachers both play an important role in raising public awareness, we recommend that a basic oral health course be introduced into the curricula of the relevant faculties.
Introduction
Dental caries and periodontal diseases are among the major public health concerns in Turkey and worldwide. 1 Since recent studies have revealed the impact of oral and dental health on overall health, many countries have started to grasp the importance of preventative dentistry and appropriate training programs for creating a healthy community. A rapid decrease in the prevalence of dental caries has been reported in some developed countries, such as Finland, Norway, and Germany. This decline has been attributed to national socioeconomic improvements, the wide use of fluoride toothpastes, changes in sugar consumption habits, widespread dental services, and an increase in public awareness of personal hygiene.2,3 In an endeavor to promote global oral health, the World Health Organization (WHO) has also emphasized through its Global Oral Health Program (ORH) that oral and dental health represents a significant part of general health and quality of life.4,5
In contrast to many global improvements and successes, oral and dental health issues are still being reported as common problems in developed and middle-income countries. Epidemiological studies have revealed that the distribution of oral diseases is influenced by sociocultural and environmental factors.6,7
The treatment costs of oral and dental disorders in developed countries are high. Treatment is also unaffordable for most people in middle- and low-income countries.8,9 Through its Global Oral Health Program, the WHO supports research promoting more economical preventative dental services. 10
Studies have proved that community knowledge levels in Turkey concerning oral health are inadequate. Additionally, due to the large number of active patients to each dentist, dental practitioners are unable to resolve this situation singlehandedly.11-13
In its 2014-revised guideline, the American Academy of Pediatric Dentistry stressed that nondental physicians and other health care providers should play a more active role in carries-risk assessment. 14 The Global School Health Initiative launched by the WHO in 1995 within the scope of preventative and therapeutic strategies also aims to boost oral and dental health services through teachers and schools. 15
It is, therefore, strongly and widely recommended that professionals involved in health and educational services, such as physicians, nurses, community pharmacists, and teachers, should support dentists in the provision of oral and dental health training.
Although individual patients can access health care providers, such as doctors, nurses, and community pharmacists, more easily in rural Turkey, the inadequate dentist-to-patient ratio in these regions can cause a number of challenges in raising public awareness toward the importance of oral health. 16
However, elementary school teachers instruct not only in core curriculum subjects but also in overall and oral hygiene, and healthy nutrition in rural areas of Turkey. 17
The aim of our study is to compare the knowledge levels of prospective elementary school teachers, physicians, nurses, and community pharmacists concerning oral and dental health with those of prospective dentists, and to suggest means by which such information can be integrated into the curriculum.
Materials and Methods
Study Design and Data Collection
The target population for our cross-sectional descriptive study, conducted at Ataturk University, Erzurum, in academic year 2016 to 2017, included 200 senior students from the Medical Faculty, 141 from the Dental Faculty, 80 from the Pharmaceutical Sciences Faculty, 108 from the Education Faculty (Department of Primary Education), and 273 from the Health Sciences Faculty. All students were included in the study with the random stratified technique. Around 100 students from the Medical Faculty, 92 from the Dental Faculty, 52 from the Pharmaceutical Sciences Faculty, 112 from the Health Sciences Faculty, and 119 from the Faculty of Education (Department of Primary Education) agreed to participate in the study. The total number of students participating in the study was 475.
Study Method
The questionnaire was prepared by the researchers by searching the literature.11,13,17 The survey questionnaire was composed of two parts. The first part contained 12 questions designed to elicit sociodemographic data, and the second part consisted of 31 questions inquiring into subjects’ knowledge of and attitudes to oral and dental health.
The reliability of the survey was determined through a field test conducted among 20 interns trained in health sciences in January 2016, who were subsequently excluded from the main study. Unusual or confusing questions were amended or redesigned. All researchers were trained by researchers from the Faculty of Dentistry. The knowledge level of all researchers was equalized. The final version was then administered to volunteer participants after briefings by five research assistants from the Faculty of Medicine, Health Sciences Department, and after oral informed consent had also been obtained.
The questions produced by the authors based on a scan of the previous literature, and the responses obtained, are shown in Table 1.
Analysis of Responses Given by the Participants.


Statistical Analysis
Data were analyzed on Statistical Package for the Social Sciences (SPSS version 20.0, IBM Corp., Armonk, NY, USA) for Windows. Descriptive statistics were expressed as percentile ranks, mean, and standard deviation. Statistical analyses were performed using the chi-square test, and P values < .05 were regarded as statistically significant.
Results
Women comprised 62.3% of the participating students and men 37.7%, with a mean age of 23.39 ± 1.49 years. The mean number of members of participants’ families was 5.40 ± 1.86, and the mean number of children per family was 3.38 ± 1.61.
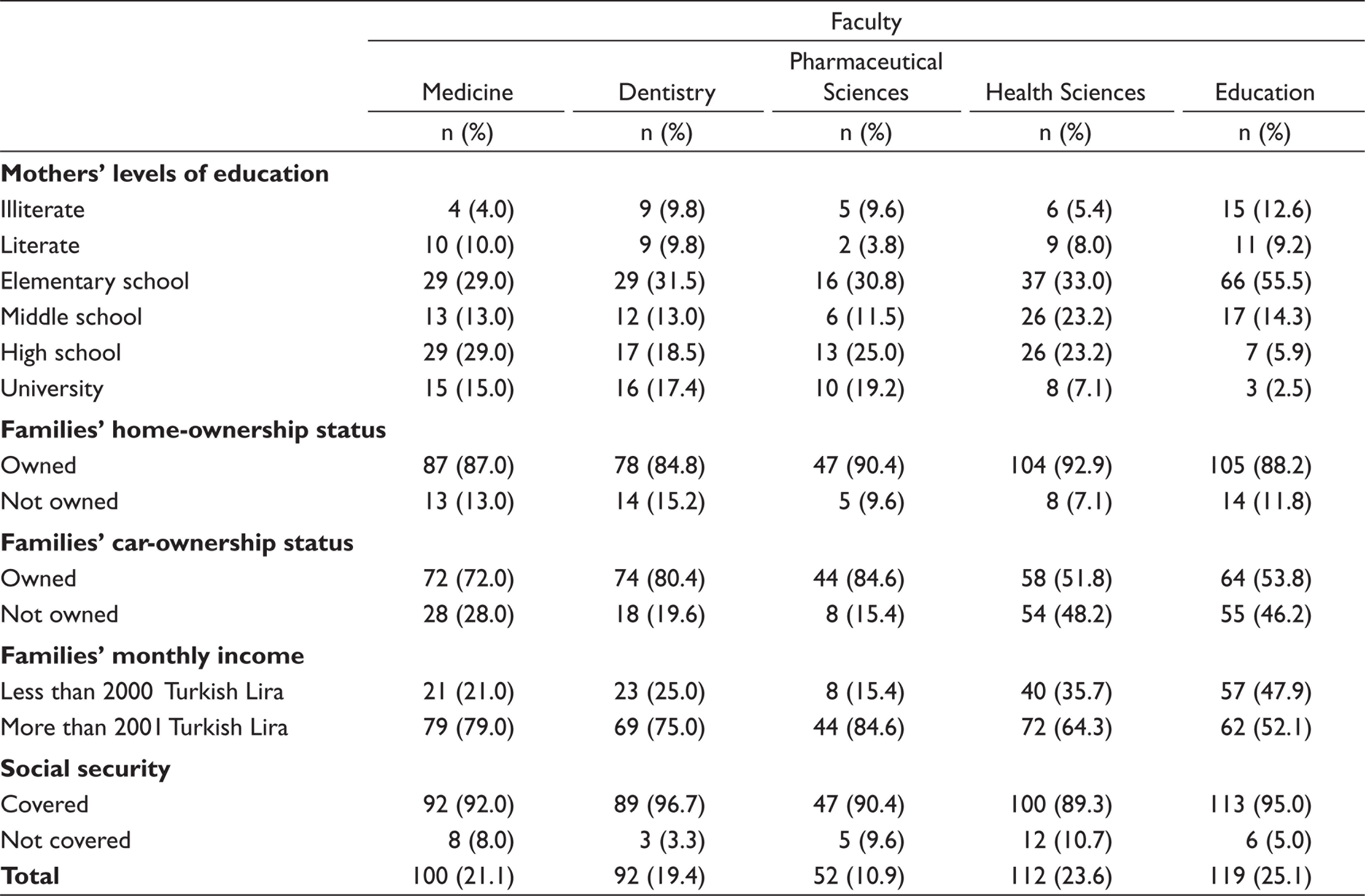
Distribution of the 475 students by faculties was 25% Education Faculty, 23.6% Health Sciences Faculty, 21.1% Medical Faculty, 19.4% Dental Faculty, and 10.9% Pharmaceutical Sciences Faculty. Students’ sociodemographic characteristics are shown in Table 2.
Participating Students’ Sociodemographic Characteristics by Faculties.
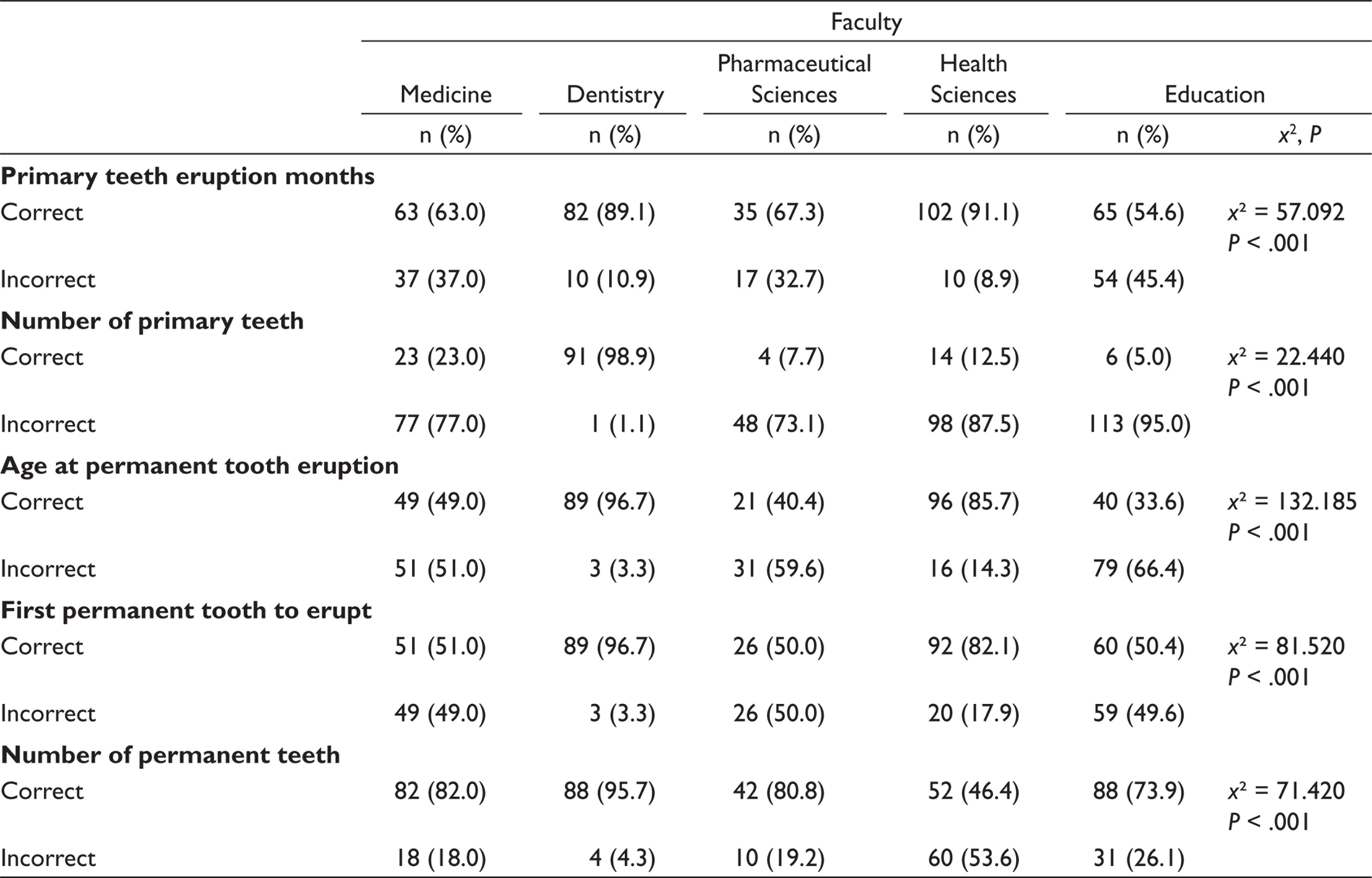
We asked the students a number of questions that aimed at measuring their level of knowledge of and attitudes toward oral and dental health. Questions intended to assess students’ overall knowledge concerning tooth numbers and eruption times, and the answers received are given in Table 3. Statistical analyses revealed significant differences between the faculties (P < .01).
Respondents’ Levels of Knowledge About Tooth Numbers and Eruption Times.
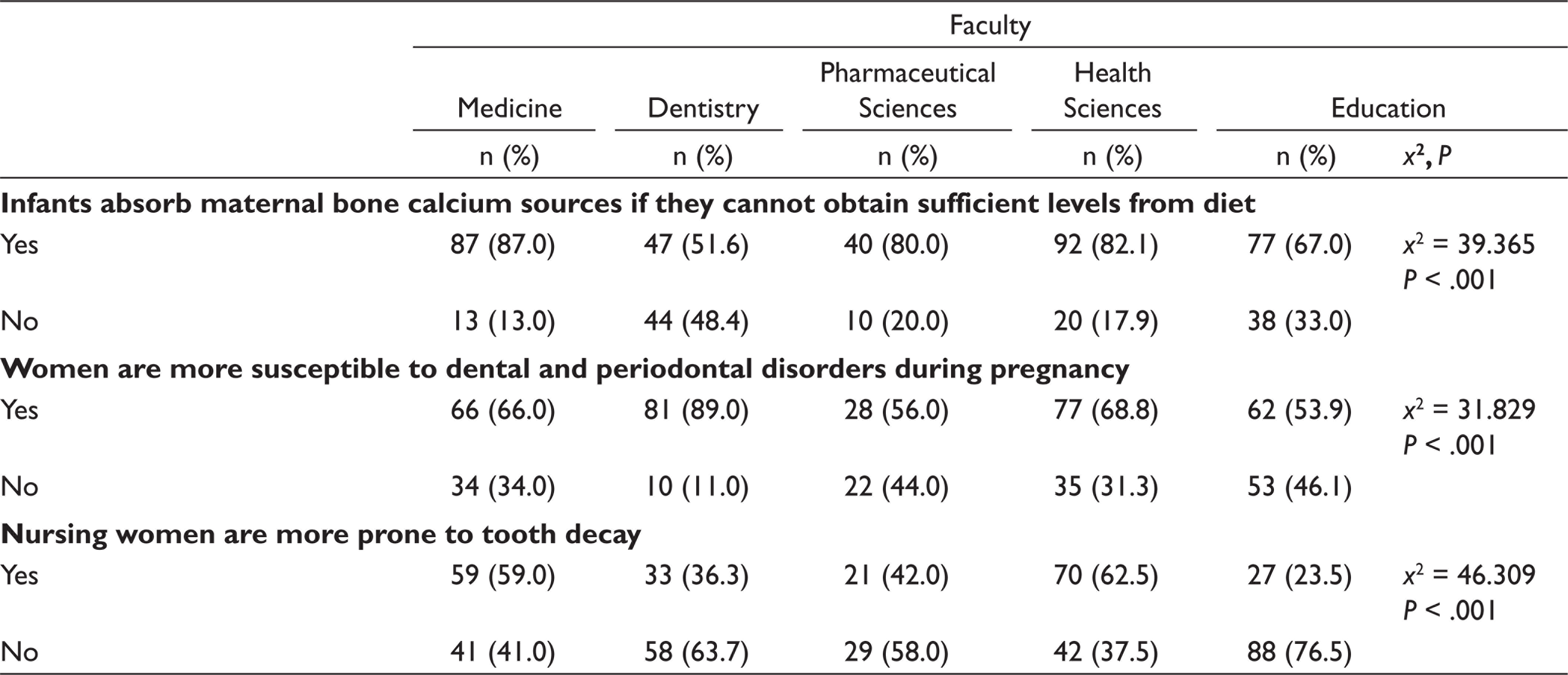
Respondents’ levels of knowledge of oral and dental health during pregnancy and nursing are presented in Table 4. Statistical analysis again revealed a significant difference between the faculties (P < .01).
Respondents’ Levels of Knowledge About Oral and Dental Health During Pregnancy and Nursing.
The percentages of students in the faculties of medicine, dentistry, pharmaceutical sciences, education, and health sciences correctly answering “fluoride” to “the caries-preventive mineral” were 51.0%, 60.9%, 57.7%, 47.3%, and 16.8%, respectively. A statistically significant difference was again observed between the faculties (P < .01).
The percentages of students reporting regularly visiting a dentist every 6 months were 25.0% in the Dental Faculty, 12.0% in the Medical Faculty, 17.3% in the Pharmaceutical Sciences Faculty, 13.4% in the Education Faculty, and 3.6% in the Health Sciences Faculty. In addition, 10.7% of students reported never having visited a dentist, while 72.6% of the dental service users reported doing so only after problems had arisen. Moreover, 2.7% of students stated that they never brushed their teeth, although 62.3% of the remaining students reported brushing their teeth at least twice a day. Statistically significant differences were determined between the groups (P ˂ .05).
The idea that “oral and dental hygiene habits for infants and toddlers should begin as soon as their first primary teeth erupt” was correctly confirmed by 72.8% of students in the Dental Faculty, 51.9% in the Pharmaceutical Sciences Faculty, 43.0% in the Medical Faculty, 42.0% in the Education Faculty, and 16.1% in the Health Sciences Faculty. The difference between the faculties was statistically significant (P < .01).
The proposition “tooth brushing training should start in children at the age of 4 to 5 years” was correctly confirmed by 59.0% of students in the Medical Faculty, 63.0% in the Dental Faculty, 46.2% in the Pharmaceutical Sciences Faculty, 47.9% in the Education Faculty, and 16.1% in the Health Sciences Faculty. The difference between the faculties was again statistically significant (P < .01).
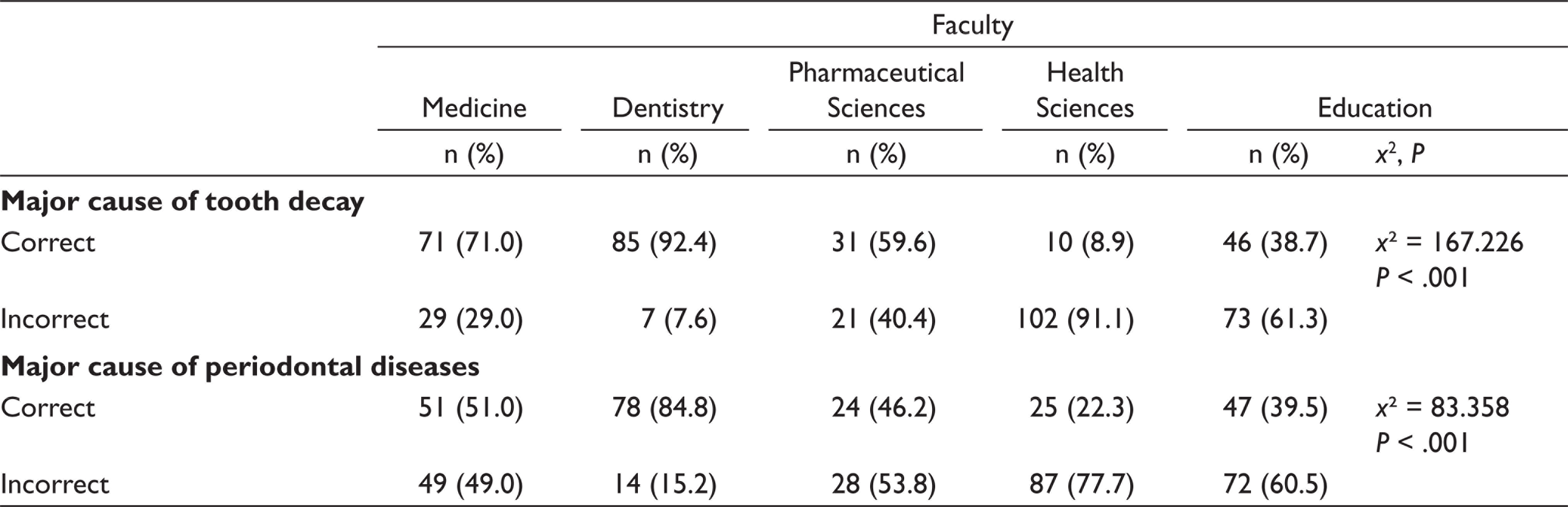
Distributions of students’ knowledge levels regarding the principal causes of dental cavities and periodontal diseases are shown in Table 5 (P < .01).
Participating Students’ Levels of Knowledge Regarding the Major Causes of Dental Cavities and Periodontal Diseases.
We determined that 48.8% of students considered themselves proficient in oral and dental health issues, and statistically significant differences were observed between the faculties (P < .01).
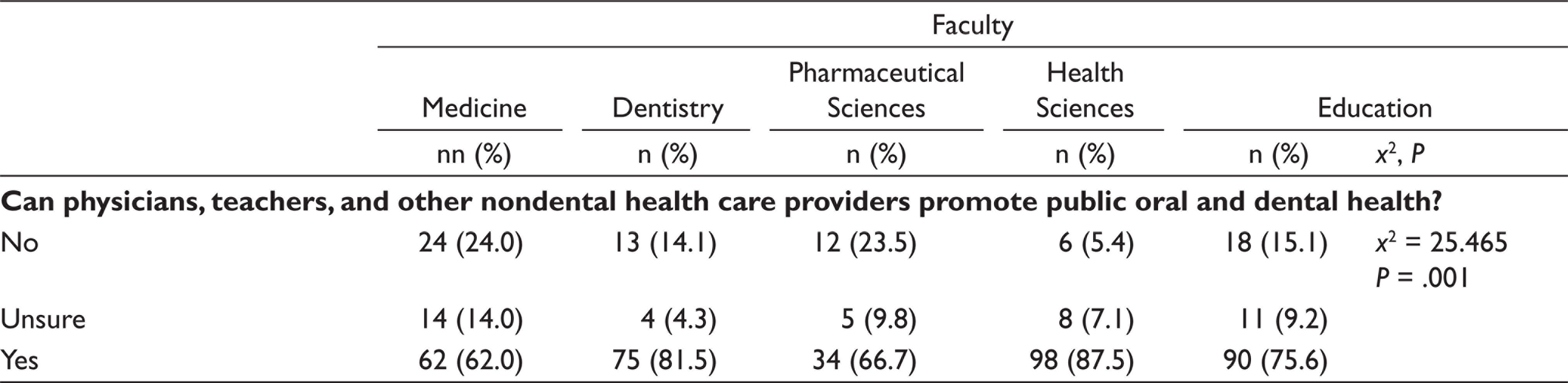
The percentages of students stating that the physicians, teachers, and nondental health care providers can make significant considerable contributions to improving public oral and dental health were 87.5% in the Health Sciences Faculty and 62.0% in the Medical Faculty. The difference between the faculties was statistically significant (P < .01; Table 6).
Respondents’ Assessments Concerning Whether Physicians, Teachers, and Other Nondental Health Care Providers Can Help Promote the Public Oral and Dental Health.
The mean percentage of students correctly answering 15 or more of the 31 questions in the questionnaire investigating the levels of knowledge of oral and dental health was 77.3%. Further analysis revealed figures of 100% for students in the Dental Faculty, 81.0% for the Medical Faculty, 78.8% for the Pharmaceutical Sciences Faculty, 76.8% for the Health Sciences Faculty, and 56.3% for the Education Faculty. The difference between the faculties was statistically significant (P ˂ .01).
Discussion
Preserving and improving oral and dental health, the primary goal of dentistry, can be facilitated through economic and social development, and reforms in education. Of these three key factors, education is the most important in terms of correcting incorrect public habits and attitudes. Ensuring oral hygiene and maintaining good oral health in adults can be achieved through proper oral hygiene habits established in childhood.
Health care providers and educators play an undeniable role in public health training. Due to the numbers of dental practitioners being lower than those of other nondental health care providers, insufficient numbers of dentists being available in rural areas, and patients often visiting the dentist’s office only in the case of dental pain or infection, dental practitioners are unable to cope singlehandedly with the issues involved in raising public awareness. 18
Data released by the Turkish Ministry of Health in 2016 revealed that 51,837 doctors, 7756 dentists, 83,795 nurses, and 22,344 midwives were working in the public sector. 16 These data confirmed that dental practitioners could be supported by other nondental health care providers. In its data for 2016, the Turkish Dental Association reported a total of 27,230 dentists across Turkey, of whom 15,412 were working in private practices and 1786 were not working at all. The patient-to-dentist ratio was 2853. Although this number might seem sufficient, dentists tend to operate more in large cities, while their numbers in smaller towns and cities are lower, ranging between 2 and 7. Dentist-to-patient ratios are insufficient in smaller cities. In 2014, for example, there was 1 practicing dentist to 1927 residents in Istanbul and to 1487 in Ankara. These figures rose to 1 dentist to 9007 residents in Agri, 4800 in Ardahan, 5056 in Aksaray, and 6188 in Kahramanmaras, all relatively smaller cities. 19
Due to the insufficient number of dentists per capita across Turkey, practicing dentists generally provide therapeutic dentistry services only, which results in limited public awareness of oral and dental health and also hinders the improvement of preventive dental services.
Low levels of public awareness of oral and dental health lead to patients visiting dentists only in case of specific emergency situations. However, a countrywide survey performed in 2004 revealed that 4.9% of the 35 to 44 age group had never visited a dentist, that 88.2% of individuals who had previously visited a dentist had presented with specific symptoms, and that only 1.1% of participants attended regular dental checkups in Turkey. 17
In the light of the above, physicians, community pharmacists, nurses, and teachers can all play key roles in establishing oral hygiene habits in the community because they have close contacts and communications with its members.
Individual awareness, a very important factor for a healthy future population, can only be acquired during childhood. 20 Childhood is the optimum period for establishing oral hygiene habits. Children first adopt their parents as role models, usually followed by teachers when they reach primary school age.
Studies have reported that children aged 6 to 11 years are particularly influenced by the language and attitudes of their parents, teachers, and physicians and start to mimic them. 3 This places enormous responsibilities on teachers, who perform such important roles in society.
Although some basic information concerning oral and dental health and teeth in general is included in social studies and science courses in the Turkish elementary education curriculum, this is not effective in terms establishing proper oral and dental hygiene habits. The levels of correct responses to propositions concerning basic oral and dental health by senior education faculty students, the teachers of the future, in our study varied between 5% and 73%.
One study assessing the roles and impact of teachers in promoting oral and dental health recommended that dental health training be incorporated into middle-school curricula and that adequate training be given to teachers to promote their vigorous engagement in oral health development activities. 21
It has also been suggested that schools can provide an optimum atmosphere for developing policies such as stimulating dental and oral health. 22 The provision of oral and dental training programs in schools helps children develop their personal skills, teaches good oral health, and encourages positive attitudes and healthy behaviors. It is of crucial importance for improving oral health problems that oral and dental health issues be incorporated into the education curriculum.
Several studies have reported that oral and dental health education programs can halt or slow the progress of dental caries. 23 In their study examining the impact of training programs implemented in regions of low-socioeconomic status and high rates of dental caries, Kowash et al confirmed the importance of education by determining a decrease in early childhood caries at the end of 3 years. 24
Early childhood caries develops in infancy. Unfortunately, parents do not take their children to the dentist in this period, even though they periodically visit pediatricians, family care physicians, and nurses for growth-development monitoring and vaccinations. Instructing parents on what they should do during tooth eruption and how to brush their babies’ teeth is, therefore, of the utmost importance.
A study compared the effect of motivational interviewing counseling visits with mothers with the effect of traditional health education, and determined lower rates of new caries in children of those mothers at the end of 2 years. 25 Our study findings revealed low levels of knowledge among prospective physicians and nurses. Interviews between primary health workers and families are of key importance, and importance must be attached to oral and dental health during their undergraduate training.
Studies have noted that community pharmacists are the most accessible health professionals to the public, 26 and they are also consulted more than physicians. 27
Al-Saleh et al reported that although community pharmacists are frequently asked for oral health care advice, most receive inadequate oral health training. 28 Taiwo and Panas reported that community pharmacists can be effectively employed to raise public awareness of oral health care. 29
No previous research in Turkey has assessed community pharmacists’ knowledge levels or contributions to public awareness. In the present study, we determined that prospective pharmacists also had low levels of knowledge of oral and dental health. However, we also think that if equipped with sufficient knowledge concerning oral and dental health, they can be effectively employed in raising public awareness. Pharmaceutical science students should, therefore, also take additional courses on oral and dental health during training.
Our study data show that prospective doctors, nurses, community pharmacists, and teachers have important roles to play in the improvement public oral and dental health. They also stated that their knowledge levels on this issue were inadequate, and that they regarded themselves as only 38% to 40% competent. However, if equipped with sufficient knowledge, they could contribute to raising public awareness of oral and dental health at a rate of 66% to 87%.
Limitations
The fact that our study was conducted among our university students facilitated the data-collection process. However, we were unable to contact those students who were absent from class on the day of data collection. There should be more students and multicenter studies across the country. Then, the data should be compared and the developments in oral and dental health should be recorded. The integration of these issues into the educational curricula should be ensured.
Conclusion
Classes on oral and dental health should be added to the pregraduation training of professional groups capable of playing a key role in the improvement of oral and dental health.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the resident physicians of the Department of Public Health, Atatürk University, for their assistance with the data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.