
Abstract
The proper knowledge of the root canal system anatomy is crucial to perform successful endodontic treatments. Maxillary lateral incisors usually have a single root. However, aberrant canal configurations of this tooth have been reported in the literature. The clinician should be aware of the difficulties arising from this more complex root canal anatomy and should be able to manage them. A rare case of a maxillary lateral incisor with three root canals is presented in this article; the challenge of diagnosis and treatment in similar situations is also discussed.
Introduction
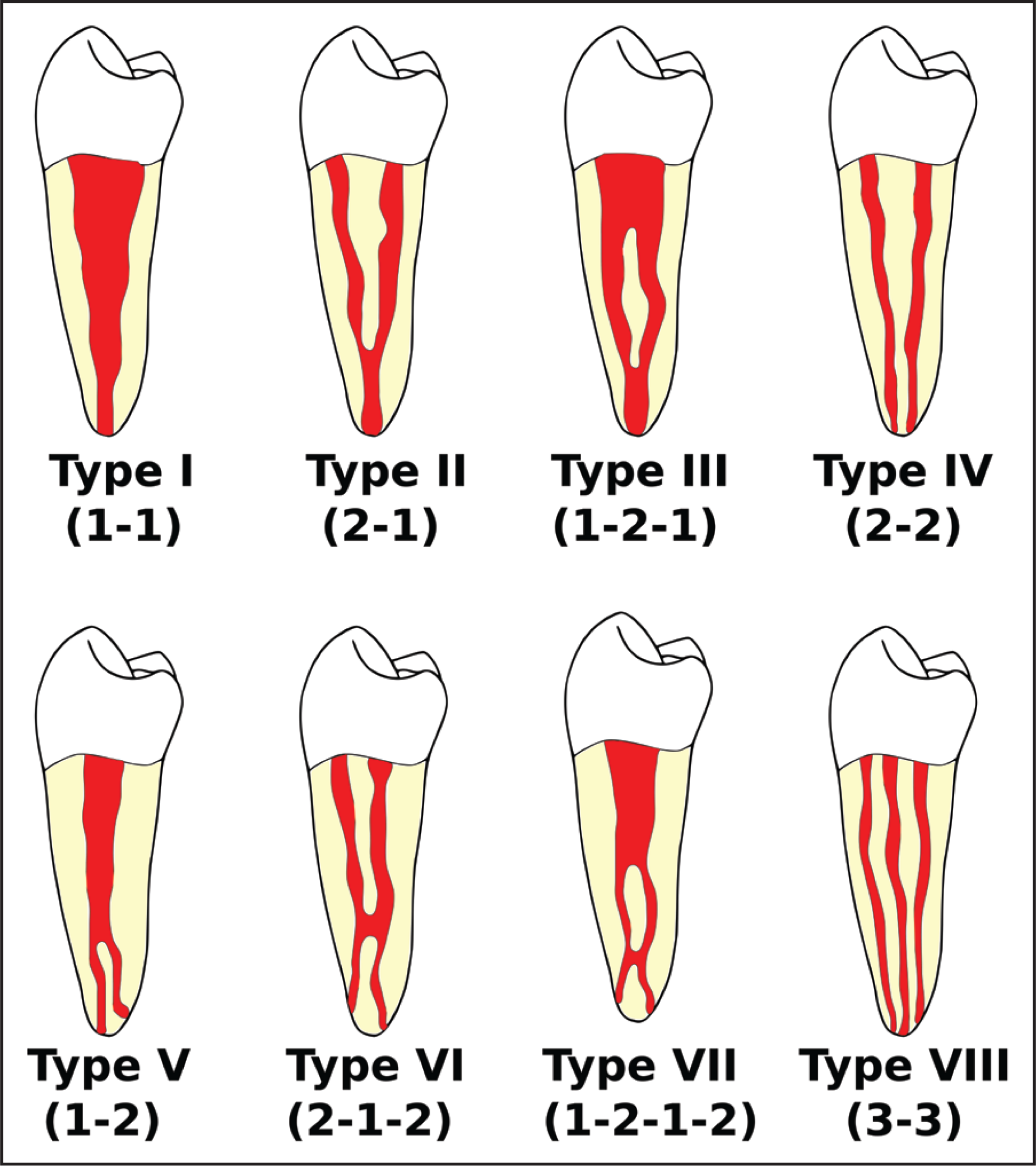
Maxillary lateral incisors usually have a single root with an apical curvature and a relatively straight, tapering canal. According to Vertucci’s configuration, which classified endodontic morphology within a single root canal into 8 different types on the basis of the number of canals from the orifice to the apex, maxillary lateral incisors generally belong to type I (Figure 1). 1 Although root canal morphology cone beam computed tomography (CBCT) evaluations confirm these findings especially in a Caucasian population, 2 aberrant canal configurations of these teeth have been reported in the literature,3-5 thus demonstrating that the endodontic anatomy of these teeth should not be taken for granted. A deeper literature analysis reveals indeed that morphology variations of maxillary lateral incisors occur with a frequency of about 10% 6 which even increases up to 22% in a Turkish population. 7 Excluding development aberrations of the tooth, root morphology of lateral incisors with more than one canal may fall into Vertucci’s type II6-8 or type IV 9 configurations; cases of lateral incisors with two separated roots have also been described. 10 Endodontic treatment failure mainly depends on the inability to clean and disinfect all root canal anatomy11,12: bacteria left in apical ramifications, lateral, or even missed canals could cause endodontic infection, and therefore induce or support apical periodontitis.13,14 In order to prevent missing anatomy, care is recommended in the diagnostic process and in the initial phases of the root canal treatment.
Diagrammatic Representation of Vertucci’s Root Canal Configurations
Case Presentation
A 29-year-old female reported to the dental office with a chief complaint of pain on the upper left lateral incisor (tooth 22). The patient reported a history of pain, swelling, and recurrent abscesses on the mentioned tooth. The patient also mentioned that the tooth had previously been subjected to a root canal treatment in order to cover it with a crown for aesthetic purposes; albeit normal in shape, in fact, the tooth had a strong palatal inclination. The clinical observation revealed tenderness to percussion; however, there were no signs of inflammation and no sinus tract was evident. Probing depth and tooth mobility were normal. The tooth was unresponsive to vitality test and electrical stimulation, while the adjacent (excluding the tooth 23, already subjected to root canal treatment) and contralateral teeth exhibited physiological responses. Preoperative radiographs showed a single root of abnormal size, with a mesio-distal width larger than usual; a previous endodontic treatment and large periapical radiolucency were evident (Figure 2). The diagnosis of previously treated tooth with symptomatic apical periodontitis was made. 15
Preoperative radiograph (taken after the old crown removal) showing an unusual root morphology; a previous root canal treatment is evident, as well as a wide periapical lesion.

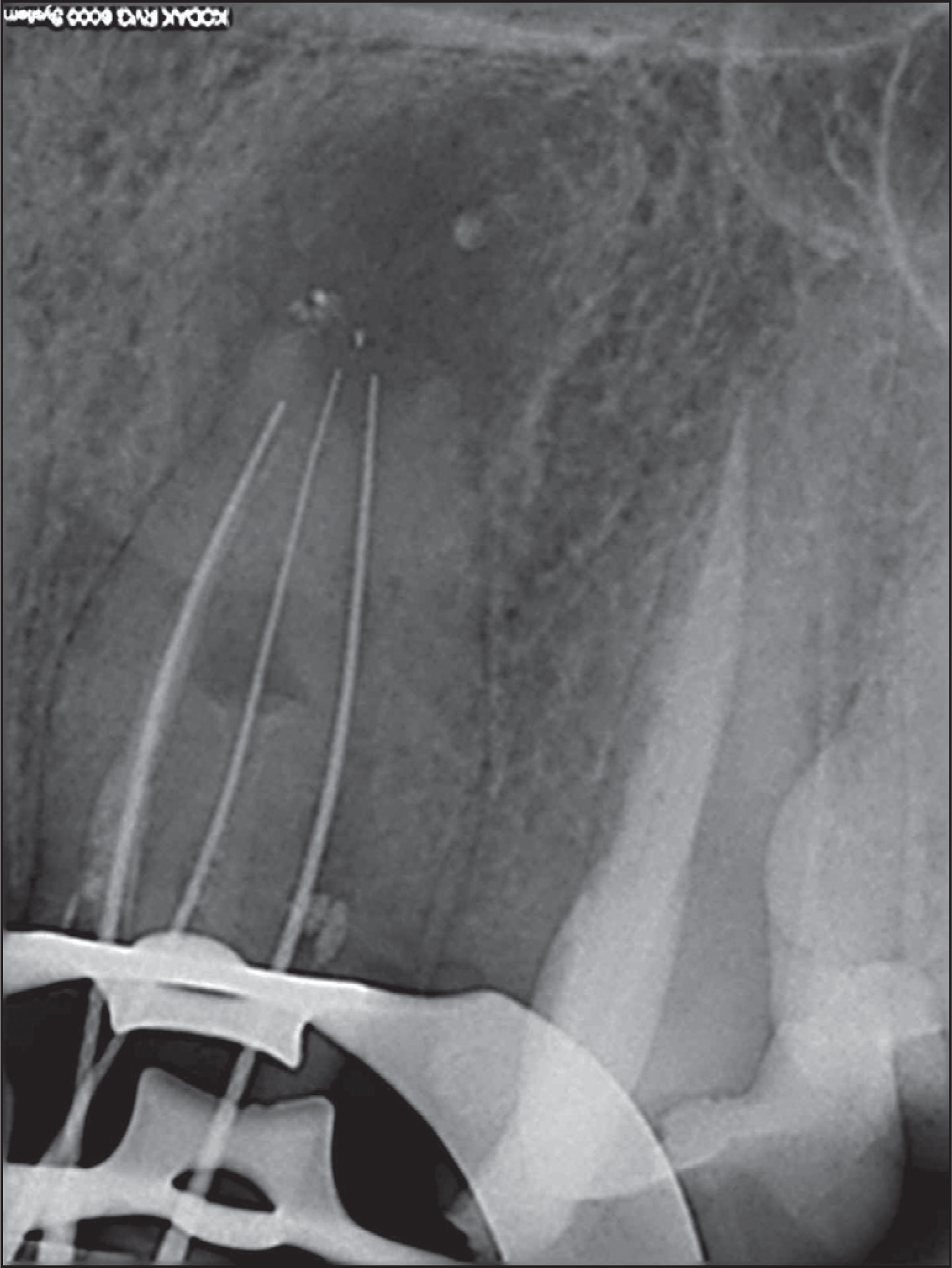
The patient accepted the proposed treatment plan that included an orthograde endodontic re-treatment, followed by the restoration of the tooth with a glass-fiber post, a composite core, and a lithium-disilicate crown. Local anesthesia was obtained with the administration of articaine hydrochloride acid (HCl) 4% with epinephrine 1:200,000 (Septanest; Septodont, Saint-Maru-des-Fosses, France). After removing the old crown, the tooth was isolated under rubber dam and the cavity access was modified with a round bur in order to find the orifices of the other presumed canals; the central and distal canals were immediately identified with an endodontic explorer, while the mesial one was hidden by a small sessile mass of inflamed gingival tissue which was eliminated with a surgical blade 15C. The three canals were explored with a steel K-File 8; the working length was established with a K-file 10 and an electronic apex locator (ProPex II Apex Locator; Dentsply Maillefer, Ballaigues, Switzerland) and then confirmed radiographically (Figure 3). Subsequently, all the canals were prepared manually to a size 40 K-file, according to a crown-down technique and alternating each instrument with a profuse irrigation of a 5% sodium hypochlorite solution (NICLOR 5-dentale; OGNA Laboratori Farmaceutici, Muggiò, Italy) and a 17% EDTA solution (E.D.T.A. 17%; OGNA Laboratori Farmaceutici, Muggiò, Italy). Finally, after drying the canals with sterile paper points, they were obtured with gutta-percha points and root canal sealer paste (Apexit Plus; Ivoclar Vivadent, Schaan, Liechtenstein), according to a cold lateral condensation technique (Figure 4A). The entire procedure required two appointments at a week of distance; during this time, the canals were medicated with calcium hydroxide (ENDOIDROX; OGNA Laboratori Farmaceutici, Muggiò, Italy) and provisionally sealed with Cavit (3M Deutschland GmbH, Neuss, Germany); the patient reported no symptoms between the 2 appointments.
Radiographic Working Length Determination With Vertucci’s Type III Root Canal Configuration
Postoperative Radiographs at the End of Treatment (A), After 12 Months (B), and After 24 Months (C)
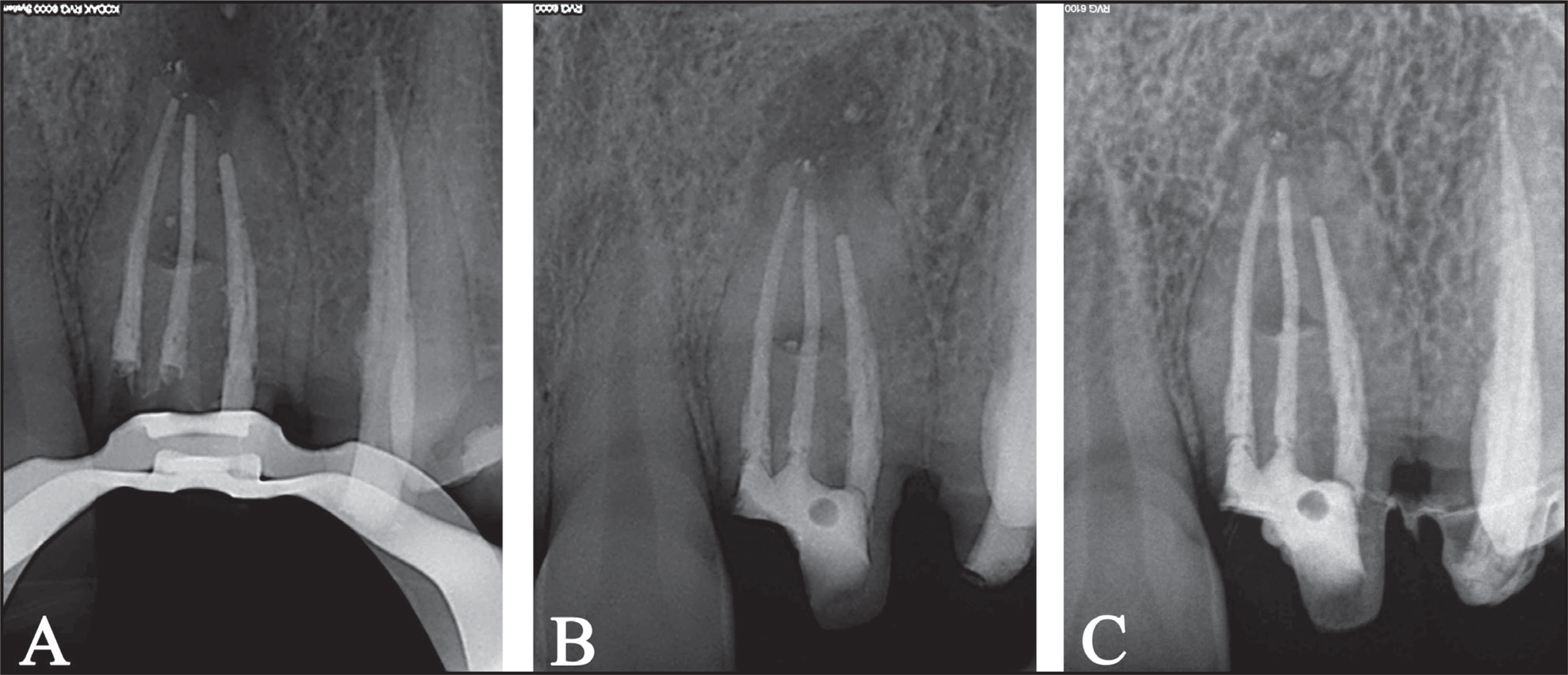
A 2-year follow-up was carried out with no clinical symptoms of failure; radiographic follow-ups at 12 (Figure 4B) and 24 months (Figure 4C) showed the progressive healing of the periapical radiolucency.
Discussion
A successful root canal treatment relies on the ability of the clinician to control the endodontic infection through the eradication of the responsible bacteria. 16 With this purpose, every canal must be found, debrided, disinfected, shaped, and then obturated in a tridimensional way. 17 Even though literature on this topic is scarce, it is commonly thought that missed or inadequately treated canals may cause failure, since they act as reservoirs for microorganisms which may lead to a persistent microbiological infection associated with periapical rarefaction. 18 A retrospective cohort study conducted in a North American population showed that teeth with a missed canal were 4.38 times more likely to be associated with apical periodontitis 19 ; a more recent paper found the risk to be even higher in a Brazilian population. 20 Untreated canals are so determining that a clinical research identified the presence of a missed canal as the primary cause of endodontic failure in molars and the second one for all types of teeth. 21
In order to prevent missing anatomy, clinicians must pay particular attention to the initial phases of any root canal treatment, especially to the radiographic examination and the preparation of the access cavity. Within certain limits, preoperative radiographs suggest the presence of abnormal roots and/or canals, hence the importance of taking a minimum of 2 diagnostic radiographs using shift cone angle technique. 22 Postoperative radiographs are also useful since obturing material non-centered within the root may be a sign of a missing canal 23 ; in the sub-mentioned case, for example, the previously treated and sealed canal was totally shifted towards the mesial side of the root, thus leading to the hypothesis that there were other canals left untreated by the previous dentist (Figure 2). However, if any additional information is needed after a comprehensive clinical examination and an appropriate conventional radiographs assessment, a request for a CBCT scan with a limited field of view should be considered. 24
Regarding the access cavity, a correct approach represents the crucial step to individuate all root canals and should be based not only on the knowledge of the endodontic anatomy but also on the information provided by the preoperative radiographs. An adequate access cavity preparation should grant the removal of the chamber roof and of everything else that may block the instruments way to the orifices of the canals, such as sclerotic dentin, dystrophic calcifications, old restorations or, as in the case reported, inflamed gingival tissue. This is more easily obtained using both rotating burs and ultrasonic (US) tips, especially designed for endodontics. US tips, which do not rotate, combine high-cutting efficiency with optimal visual access and better control, thus enhancing safety in areas with high-perforation risk.25-27 This is especially true when US endodontic tips are used with the aid of a dental operating microscope which offers better lighting and improved vision of the operative field. 28
Conclusions
Deviations in maxillary lateral incisors endodontic morphology are not as rare as expected. Being aware of how missed anatomy may lead to failures, clinicians should be able to guess the existence of supernumerary canals in the diagnosis phase and consequently adjust the access cavity preparation in order to find all of them.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.