
Abstract
Aims and objectives:
The aim of this study was to assess the influence of periodontal status on quality of life (QoL) with the use of a short version of the Oral Health Impact Profile (OHIP-14) in patients with periodontal disease attending university in Riyadh, Saudi Arabia.
Materials and methods:
Adult patients diagnosed with periodontal disease and having minimum of 15 teeth or more present was included. Included patients were requested to fill a questionnaire form and undergo a comprehensive clinical periodontal examination. The influence of oral health on patients’ QoL was assessed using the Arabic version of OHIP-14.
Results:
A total of 25 adults aged between 23 and 80 years with a mean age of 49 years completed the questionnaire. The impact of periodontal disease on patient’s QoL was statistically significant in 2 domains, namely physical pain (P = .004) and psychological disability (P = .001). The severity of periodontal disease did not show a negative impact on functional limitation. In general, the total OHIP-14 scores were statistically significant with the number of teeth with pocket depths of 5 mm (P = .001) and 7 mm (P = .011).
Conclusions:
Periodontal destruction has a negative impact on QoL. The use of this index as well as other patient-centered outcome measures has significant implications in periodontology, including treatment planning and evaluation of treatment results.
Introduction
Chronic periodontal disease is a common inflammatory oral disease, which is reported to affect 30.1% to 50.8% of adult population in Saudi Arabia aged between 25 and 55 years. 1 For several years, the significance and demand of periodontal maintenance have mostly been credited to the high percentage of disease in most demographics. In recent periods, the significance of periodontal care has emphasized on its association with altered systemic conditions including diabetes mellitus, obesity, cardiovas-cular diseases, and respiratory disorders.2-6 Other recognized risk factors for periodontal disease that have been investigated in recent times include cigarette smoking, vaping electronic cigarettes, and psychological stress.7-9
The extent of periodontal inflammation is estimated by evaluating clinical periodontal variables including bleeding on probing (BOP), periodontal probing depth (PPD), and clinical attachment loss (CAL). 10 Because of its chronic and asymptomatic nature, patients are generally unaware of their periodontal status and they therefore undervalue any therapeutic approach. However, these symptoms are pertinent from patients’ standpoint and often have substantial negative influence on their daily quality of life (QoL). 11 There is insufficient evidence about this aspect because such aspects are not generally reported in research studies and warrants further investigation.
Extensive debate has appeared on the application of conventional clinical indicators in periodontal treatment. Hujoel and co-workers 12 stated that such clinical indicators are no more than just surrogate endpoints, but such factors are also clinician centered. Recent studies13,14 have investigated a wide perspective in the form of satisfaction factors that are also known as patient-centered outcomes.
Precise scales to evaluate oral health-related quality of life (OHRQoL) have been developed. Most of the measurements describe aspects of symptoms, for instance, comfort, pain, speech, chewing, appearance, psychological aspects, and social aspects including social life, work, and finances. 15 The concise version of the Oral Health Impact Profile (OHIP-14) consists of 14 items obtained from the original 49-item OHIP, and it seems to have sound rationality and reliability characteristics in measuring the OHRQoL.16,17
Numerous investigations have explored the impact of QoL on periodontal disease. For instance, Needleman and colleagues 18 assessed the influence of oral health on QoL in consulted patients with periodontal disease from United Kingdom and concluded that periodontal health impacts on life quality. Another study by Ng and Leung, 19 explored in Chinese cohort, reported a significant association between OHRQoL and periodontal health. Another study conducted 20 in Brazil reported that the deteriorated periodontal tissues have a negative impact on the masticatory performance and QoL, as shown by the scores of the Brazilian version of the OHIP-14. In addition, the association between the severity of periodontal inflammation and QoL was measured in Jordanian patients and a positive association was found between them. 21
To the authors’ knowledge, there have been no studies that have assessed the impact of OHRQoL on patients suffering from periodontal disease in Saudi Arabia. There-fore, the aim of the present study was to evaluate the impact of periodontal health status on QoL using the short version of OHIP-14 in periodontal disease patients attending university setting in Riyadh, Saudi Arabia.
Materials and Methods
This study was officially approved by the College of Dentistry Research Center of King Saud University (Research Project No. E-17-2745). A convenient sample of 25 adult patients referred to the periodontal specialist clinics at the College of Dentistry, King Saud University, were selected. Adult patients aged 18 years or older diagnosed with periodontal disease and having minimum of 15 or more teeth were included in the present study. The exclusion criteria were as follows: edentulous patients, psychological or mentally handicapped patients, antibiotic coverage, presence of a removable denture, and the presence of a symptomatic oral lesion.
Included patients were requested to fill a questionnaire form and undergo a comprehensive clinical periodontal examination. The questionnaire included information regarding patient’s demographic status such as age, gender, marital status, level of education, social history, reporting any chronic medical condition, use of medication, smoking history, oral hygiene status, previous dental appointments, and periodontal treatment in the past 6 months.
The impact of oral health on patients’ QoL was assessed using the Arabic version of OHIP-14. The Arabic version of the index was validated in a previous study in Jordan. 21 The questionnaire was self-administered containing 14 questions to record 7 dimensions: physical pain, functional limitation, psychological discomfort, psychological disability, physical disability, social disability, and handicap. Responses to each question were recorded using a 5-point Likert scale that included: 0, never; 1, hardly ever; 2, occasionally; 3, fairly often; and 4, very often. The answers of “often” and “always” had an impact and responses of “sometimes,” “rarely,” and “never” had no impact on patients’ QoL. 19 An impact on each of the 7 dimensions of the OHIP-14 was calculated by adding up all the answers to the 2 questions that represent each of these dimensions. The total scores for OHIP-14 were gained by adding all answers for each subject, which ranged from 0 to 56 points.
Clinical examination was performed by 1 trained and calibrated periodontal examiner. Clinical periodontal parameters including PPD, CAL, and BOP were assessed at 6 points on each tooth. Plaque scores were recorded as dichotomous reading, present or absent at 4 sites per tooth. In addition, the number of teeth with PPD ≥3, ≥5, and ≥ 7 mm, and those with CAL ≥3, ≥4, and ≥5 mm were also measured for each patient. Measurements of all teeth except third molars were recorded.
Statistical Analysis
SPSS, version 16, was used for data processing and analysis. Characteristics of variables were described using frequency distribution, mean, and standard deviation. The independent t-test was used to assess the association between the categorical variables. The Pearson correlation analysis was used to find the correlation between the degree of periodontal disease severity and the differences in the OHIP-14 scores. Alpha level <5% were deemed statistically significant.
Results
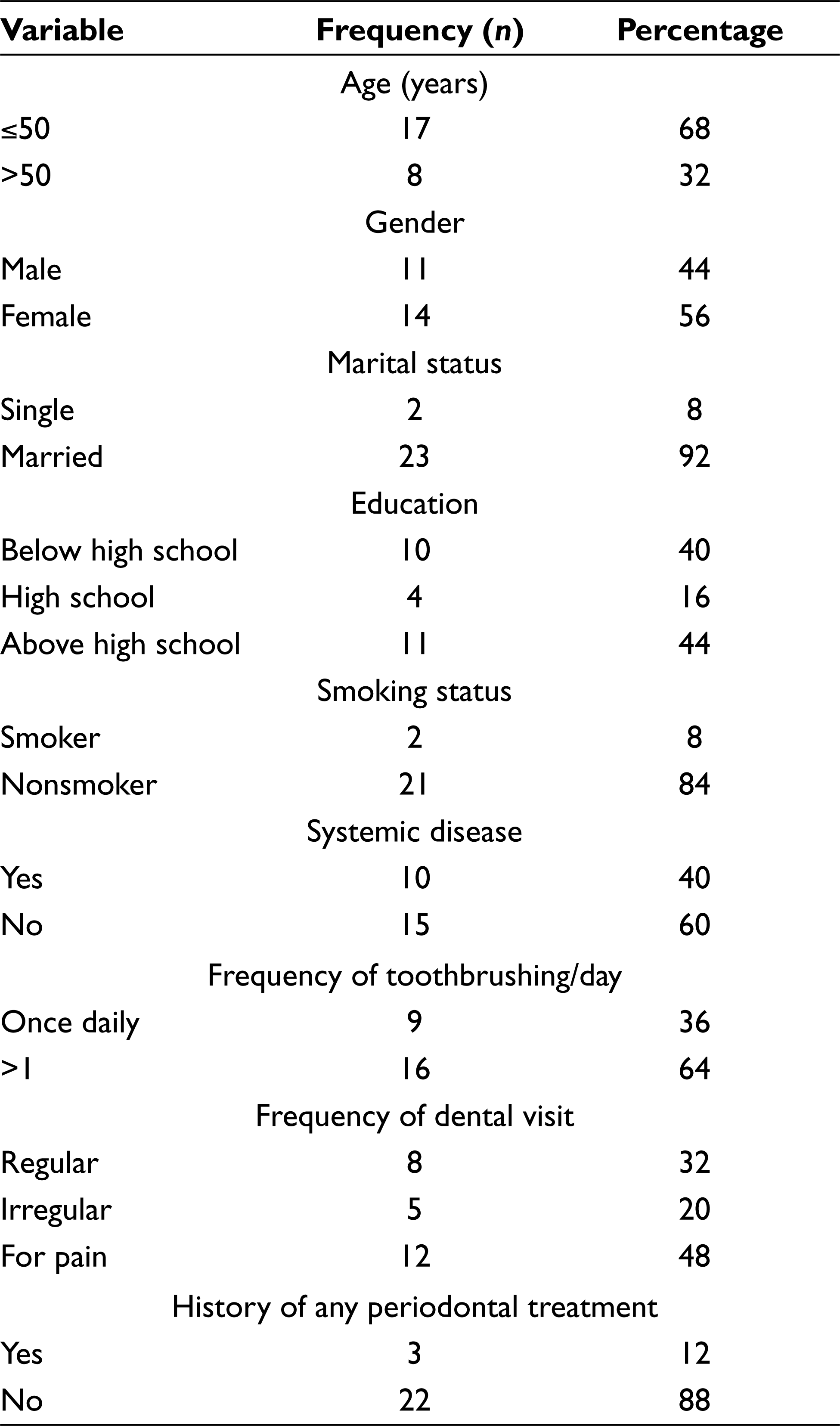
A total of 25 adults (11 males and 14 females) aged between 23 and 80 years with a mean age of 49 years completed the questionnaire. Patients’ socio-demographic, clinical, and other pertinent data are reported in Table 1. Almost equal percentage of participants had the education level either below (40%) or above (44%) high school. A total of 84% of participants were nonsmokers and 60% reported no history of any systemic disease. Greater than once daily tooth brushing was reported by almost 64% of the included participants. Around half of the participants (48%) sought dental treatment for pain. No history of previous periodontal treatment was reported by 80% of the participants.
Sociodemographic, Clinical, and Other General Characteristics of Participants
Oral hygiene measures and periodontal variables of the included patients categorized by age are reported in Table 2. Although the plaque index, BOP, mean PPD, and mean CAL were slightly higher in participants aged >50 years than ≤50 years group, none of the clinical periodontal parameters showed statistically significant difference between the 2 groups.
Oral Hygiene and Periodontal Status of Participants by Age
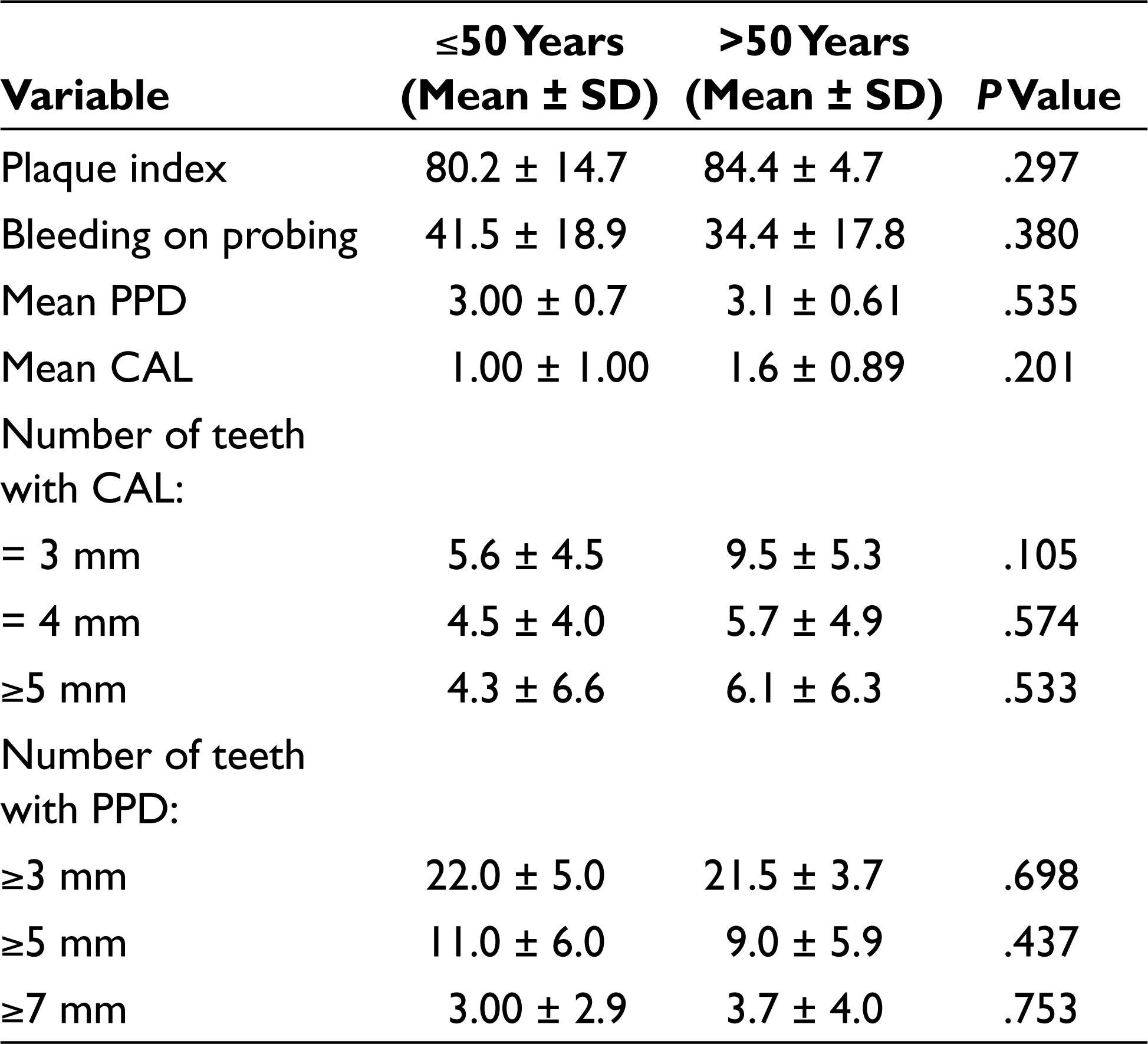
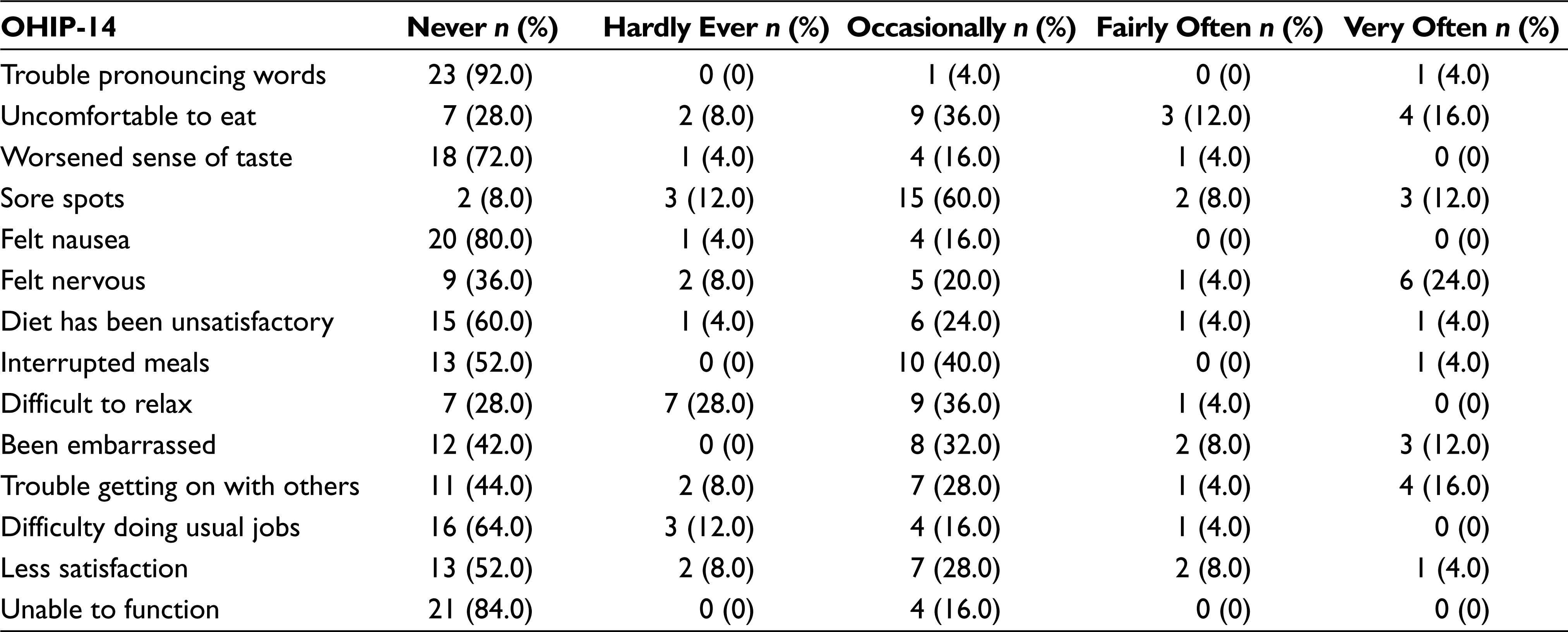
Table 3 shows the distribution of responses to the OHIP-14 items for all participants. Occasional uneasiness to eat food was reported by 36% of participants. A striking 60% of participants also reported occasional sore spots inside the mouth. Total 24% of the patients reported that they felt nervous and their diet being unsatisfactory very often. Nearly 40% and 36% of patients reported occasional interrupted meals and difficult to relax, respectively, whereas 32% and 28% reported occasional embarrassment and trouble socializing, respectively.
Distribution of OHIP-14 Individual Items Response
It was found that the impact of periodontal disease on the patient’s QoL was statistically significant in 2 domains, namely physical pain (P = .004) and psychological disability (P = .001) (Table 4). The severity of periodontal disease in this current study did not show a negative impact on functional limitation. In general, the total OHIP-14 scores were positively related to the remaining number of teeth with PPD 5 mm or deeper (P = .001), as well as the number of teeth with pocket depths of 7 mm or deeper (P = .011) (Table 4).
Pearson Correlation of OHIP-14 Subscales with CAL/PPD
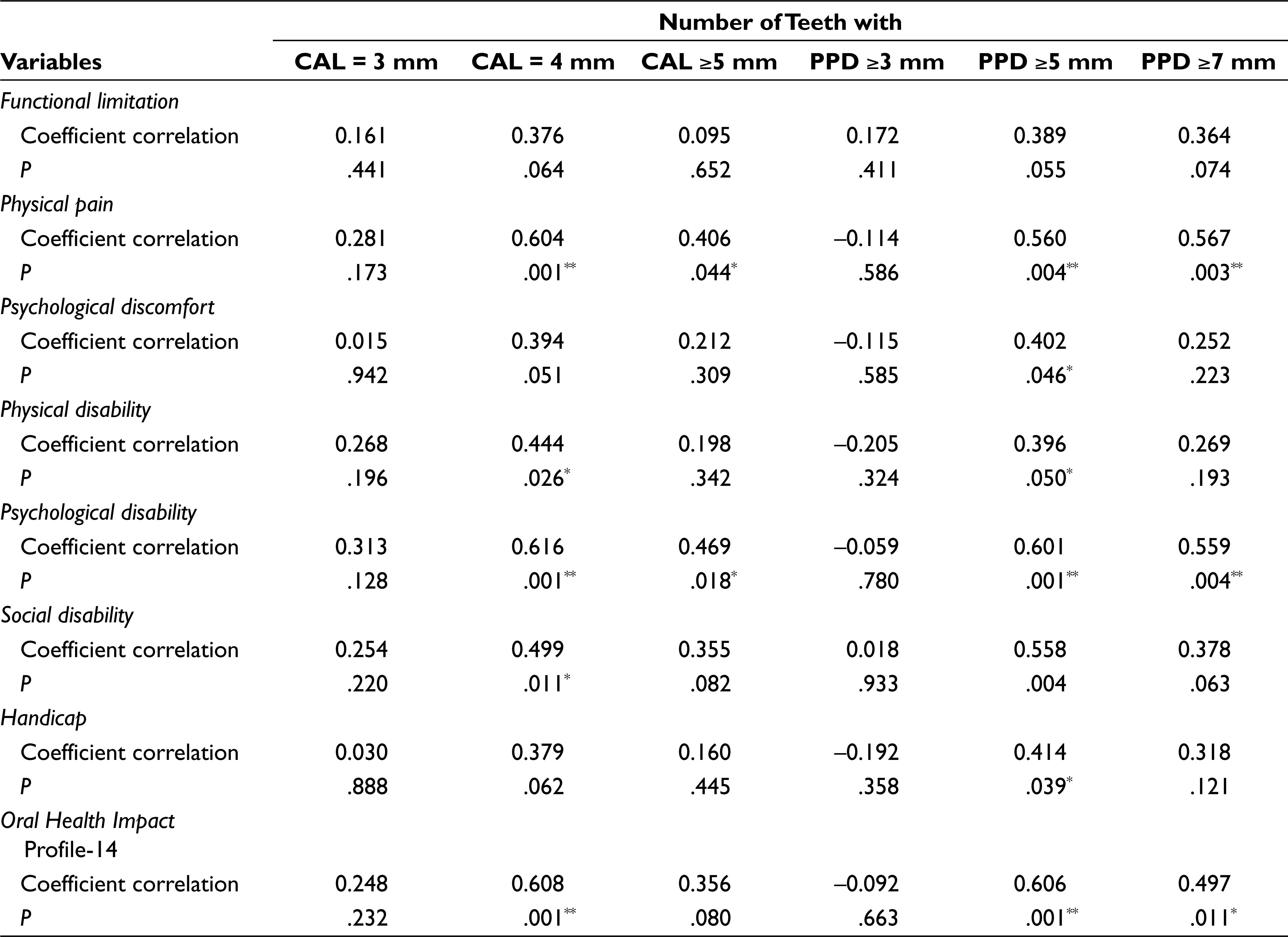
**Significant at <.01
Discussion
The present study was based on the hypothesis that periodontal status significantly affects OHRQoL. It was found that the influence of the periodontal condition on patient’s QoL was significantly affected by psychological disability and physical pain. However, the extent of periodontal inflammation in this current study did not show a negative impact on functional limitation. In general, the total OHIP-14 scores were statistically significantly associated with the remaining number of teeth with PPD 5 and 7 mm.
QoL is highly recognized as an acceptable and appropriate scale that is considered as an important indicator of treatment need in epidemiological research and practice. Health-related QoL procedures including both objective and subjective evaluations are useful for estimating efforts to prevent chronic conditions and appraising their efficiency. 22 Evaluating the hazards of impaired oral health from the patient’s view has appeared as an important research area. 23 This has led to an increase in the use of patient-centered oral health status measures, primarily attempting to measure the impact of oral health on QoL. The Arabic version of the OHIP-14 was used in this study to assess such effect, and it had been shown in a previous study in Jordan to be valid and reliable. 21
A number of clinical studies have utilized OHIP-14 to estimate the influence of periodontal disease on the QoL.16,24 In a study by Borges et al, the Brazilian OHIP-14 index was used to measure the OHRQoL on 24 patients with varying degrees of periodontal conditions. 20 It was concluded that there was a statistically significant correlation between the OHIP-14Br total score and the degree of loss of the periodontal tissue.
In the present study, it was found that the impact of periodontal disease on the patient’s QoL was statistically significant in 2 domains, physical pain and psychological disability. The significant correlation between disease severity and physical pain is in agreement with that reported by other studies.19-21 The severity of periodontal disease in this current study was not significantly correlated with functional limitation. This is in contrast to the results reported by Ng and Leung 19 and da Silva Araujo et al, 24 which showed that periodontal disease had a statistically significant effect on functional limitation. In general, the total OHIP-14 scores were significantly related to the number of teeth with pocket depths of 5 mm or deeper. The same correlation was also found with the number of wteeth with the clinical attachment loss of 4 mm, which is in agreement with that reported by Bernabé and Marcenes. 25
Like any other research study, this study also has some limitations that should be taken into account. The present study consisted of small sample size. This can be attributed to time restrictions and difficulties finding patients that fit the inclusion and exclusion criteria of the study. This study, however, to our best knowledge, appears to be the first study to estimate the influence of periodontal disease on the QoL using the Arabic version of the OHIP-14 index in Saudi Arabia. We highly recommend conducting a similar study on a larger sample size to measure the influence of periodontal conditions on QoL on a larger scale and obtain better generalizable results. Furthermore, future investigation is also warranted to evaluate whether the measure of OHRQoL as a patient-centered outcome is sus-ceptible to variations in periodontal health over a period and also to assess at the level of the individual. The instrument used showed discriminative validity in recognizing participants with self-reported symptoms associated with periodontal diseases and those with a clinical sign of established periodontal destruction.
Conclusions
Within the limitation of our study, it can be concluded that by using the Arabic version of the OHIP-14 index, periodontal disease had a negative influence on QoL. These findings suggest that the use of this index, as well as other patient-centered outcome measures, has significant implications in periodontology, including treatment planning and evaluation of treatment results.
Footnotes
Acknowledgements
We would like to thank Dr Rola Al Habashneh for providing us with the Arabic short-form version of the OHIP-14 questionnaire.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.