
Abstract
Background:
Oral health touches every aspect of our lives and still it is been taken for granted. The access and affordability to oral health care services are very limited and expensive especially in developing countries.
Objectives:
The article highlights the importance of global oral health and how it can tackle the growing noncommunicable diseases (NCDs) epidemic. Dental caries remains a significant problem even among the developed nations affecting 60% to 70 % of the children. Oral cancers, Qat chewing, craniofacial anomalies, and dental trauma contribute significantly to the global burden of diseases. Despite the magnitude of oral illness, there is neglect in global oral health, resulting in lack of combined action and support within the arena.
Conclusions:
Oral conditions share many common risk factors with NCDs and are also affected by similar social determinants. The Political Declaration of the High-level Meeting on the prevention and control of NCDs recognizes that oral diseases pose a significant burden for many countries and these diseases also share common risk factors of NCDs and can benefit from the multisectoral and multipronged approaches to NCDs. To address the existing inequities and inequalities in oral health care services globally, it is vital to ensure coverage for the poor and disadvantaged populations.
Recommendations:
There is a great need to develop some measurable oral health goals for global comparison in order to track, reduce oral disease burden, and to promote good oral health thereby advancing global public health.
Introduction
Oral health is a significant problem in the world and also a public health issue which is neglected. Although there are significant improvements in oral health condition of the people in several countries, global problem related to oral health and its related condition still persist. Oral disease condition like dental caries, periodontal problems, tooth loss, orodental trauma, oropharyngeal cancers, gum and supporting structure of the tooth-related condition are some of the major public health problems worldwide, and poor oral health imposes an enormous impact on general health and quality of life. Across the countries and regions, there is great diversity of oral disease patterns and its related developmental trends which reflect the distinct risk profiles and institution of oral health programs.
According to WHO, 1 dental caries continues to be major oral pathological state in most of the industrial countries, affecting almost 60% to 90% of children of school going age and the major proportions of adult population. A majority of adult periodontitis cases are contributed by smoking alone, and the prevalence of oral cancer is very high among men as the 8th most common cancer of the world. The recent statistics 2 indicate the incidence of oral cancer in men ranges from 1 to 10 per 100 000 persons in many countries and, especially, it ranks amongst the three major cancers in South Central Asia. Oral cancer accounted for almost 300 000 new cases and around 145 000 deaths in 2012. It also contributed 702 000 prevalent cases over a period of 5 years and is ranked as the 11th most common cancer in the world. A study conducted by Sankarnarayanan et al. concluded that low- and middle-income countries (LMICs) contribute to two-thirds of the global incidence of oral cancer of which half of those cases are in South Asia. 3 Other addictions like chewing Qat which is a leafy narcotic substance common in East-African countries and Arab region leads to serious oral health effects namely, lesions of oral mucosa, discoloration of teeth, dryness of mouth, and poor oral hygiene. The other challenges of public health include the management of cranio-facial anomalies, for example, cleft lip and palate which has an average incidence of 1 per 500-700 births. The increasing trends of dental traumatic injuries, 16% to 40% among 6-year old and 4% to 33% among 12- to 14-year old, are quite alarming globally and need great attention. WHO recognizes and emphasized oral health as an integral part of general health. As defined by World Dental Federation, Oral health 4 “is multi-faceted and includes the power to talk, smile, smell, taste, touch, chew, swallow and convey a variety of emotions through facial expressions confidently and without pain, discomfort and disease of the craniofacial complex.”
Global Burden of Oral Diseases
Currently, the oral disease cases are high in Americans than that in Africans. But in the light of change in lifestyle patterns, incidence of decay tends to extend in developing countries, due to inadequate exposure to fluorides and excess intake of sugar. Globally, in many developing countries, access to oral health care services is very limited due to various constraints, and affordability to acquire oral care is very expensive especially in developing countries where dental care insurance is not available. 5
Oral health conditions have not been improved in the last 25 years. The cumulative burden of oral diseases alarmingly increased in numbers during 1990 and 2015, especially because of demographic changes which include aging population and growth of inhabitants. There is a huge burden of untreated oral conditions where the number rose from 2.5 billion in 1990 to 3.5 billion in 2015 which equals to 64% increase of Disability Adjusted Life years Lost (DALYs) globally. 6 Oral health condition and its related diseases are clearly more prevalent around the world, emphasizing the critical role of public health and posing a challenge to the policymakers.
The main rationale of this review is to emphasize that oral health and oral diseases should be considered with the same priority as done for noncommunicable diseases (NCDs). The article also aims to address the barriers in global oral health inequalities and highlight prevention aspects in oral health rather than just focusing on diagnosis and treatment.
Oral Health and Its Relation with NCDs
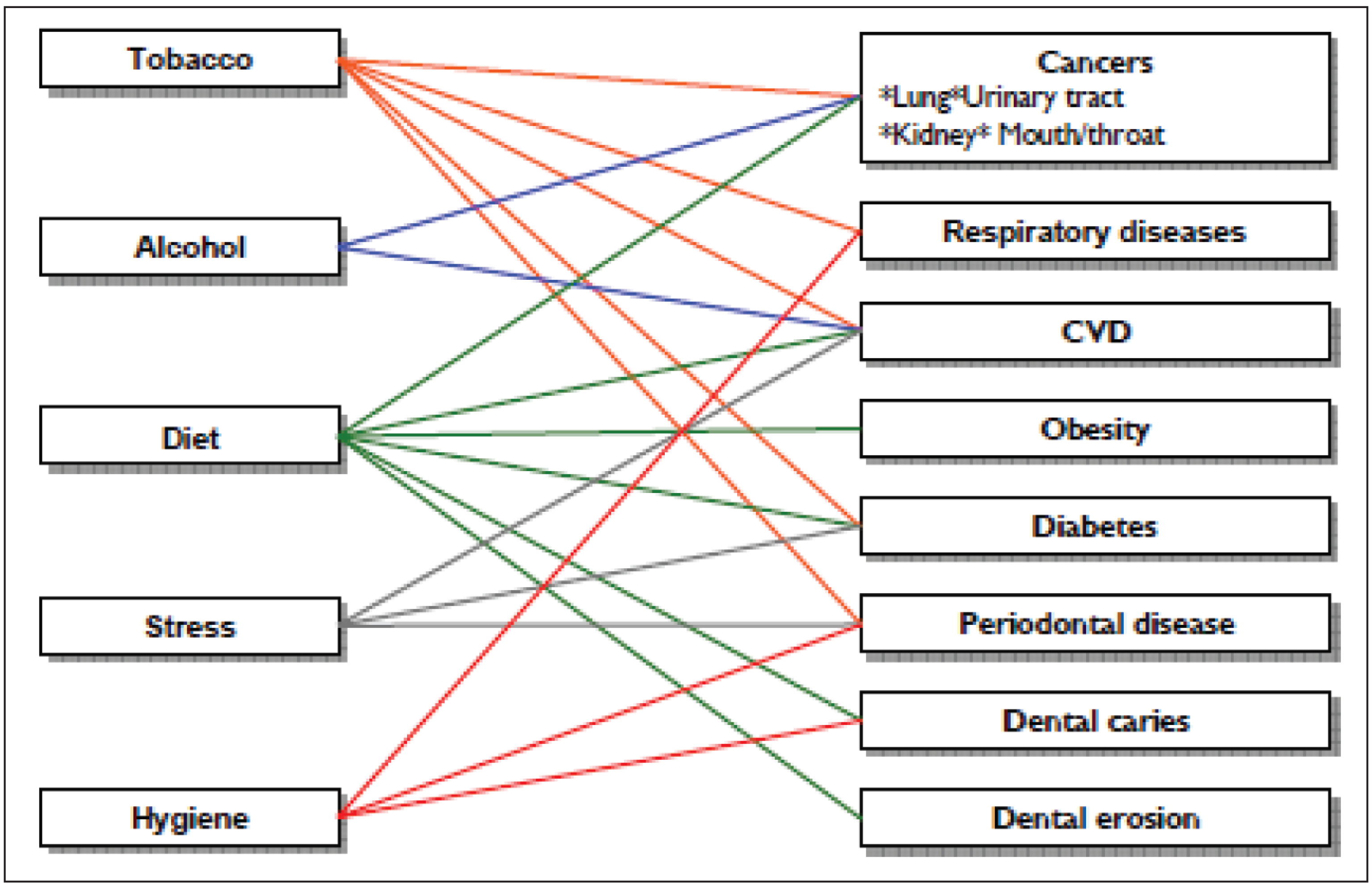
NCDs are defined as diseases of long duration, generally progressing slowly and are the prime cause for mortality and morbidity among the adults globally.5 The oral diseases and the four major NCDs namely, cardiovascular diseases (CVDs), diabetes mellitus (DM), cancers, and chronic pulmonary diseases share common risk factors which are preventable and related to lifestyle as shown in Figure 1. The most common risk factor is tobacco use which is estimated to account for 90% cancers in the oral cavity, associated with periodontal breakdown and premature tooth loss. Especially, the dietary habits pose a major risk for the development of NCDs and also influence the dental caries formation. Strong associations have been linked between NCDs and oral health in various literatures. 7 Numerous factors like tobacco use, alcoholism, unhealthy diet, particularly consuming high amount of sugar, physical inactivity, and improper oral hygiene practices are parallel to NCDs and oral diseases. 8 There are plethora of literatures showing that there is a strong association of periodontal diseases with CVD, DM, preterm low birth weight pregnancies, osteoporosis, chronic renal failures, rheumatoid arthritis. This association of oral disease with NCDs is due to the commonality of risk factors like systemic inflammatory factors and body metabolism. In Asian region, it has been reported that NCDs contribute for 56% of disease burden. 9 The widespread oral diseases may be among the foremost common NCDs and is a leading problem to development and accomplishment of health related UN-Sustainable Development Goals. Generally, in poor resource settings, there is a requirement to know the basic gaps in the understanding of oral diseases and NCDs.
Integration of Oral Health with the Framework of General Health
Oral health conditions are one of the most prevalent NCDs affecting around 4 billion people globally. Oral conditions share many common risk factors with NCDs and are also affected by similar social determinants. 10 Especially among the poorer socioeconomic strata, it was found that the socioeconomic impact on oral health and diseases is significant in most countries. Oral conditions are of complex in origin and do share significant number of modifiable risk factors (tobacco use, harmful alcohol consumption, unhealthy diets) along with the leading NCDs. 5
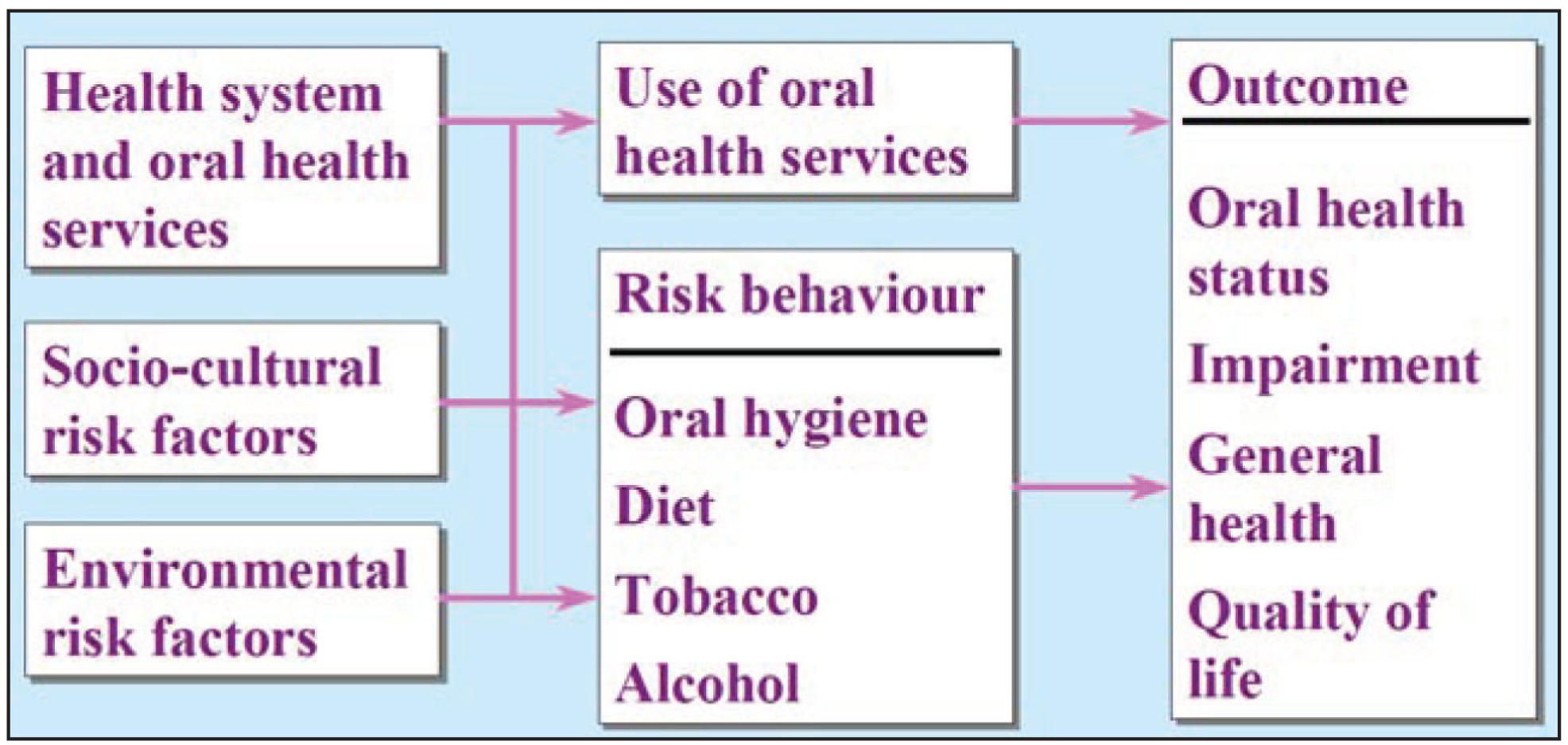
In addressing the burden of oral diseases, for the last few decades, the oral health programs were focusing on isolated and specific diseases despite the recommendations for integrated approach from WHO (Figure 2) and common risk approach developed by dental public health researchers. So many oral health programs still follow and implement the vertical approach with a focus to the isolated and specific conditions rather than an integrated approach. 12
The primary reason for disability worldwide is mainly due to the rising epidemic of NCDs.
The political declaration on NCDs and global action plan on prevention and control of NCDs from 2013 to 2020 defined the set of a collection of policy actions relating to the vibrant role of WHO in supporting member states, particularly developing countries, to complement the national efforts to address the challenges of NCDs through the multisectoral and multipronged approach. 13 Considering the current and rising burden of the oral conditions, there is a great need for the international oral health community to effectively coordinate and support the countries in implementing effective strategies and policies to promote good oral health. As key partners and stakeholders, there is an urgent need for the contribution by nonpublic sector, especially academia, policy analysis centers, intergovernmental organization, nongovernmental organizations to play a dominant role in this process to ensure sustainability. 5
The Political Declaration of the High-level Meeting of the General Assembly on the Prevention and Control of Non-communicable Diseases – United Nations General Assembly (September 2011), Recognize that renal, oral and eye diseases pose a major health burden for many countries and that these diseases share common risk factors and can benefit from common responses to non-communicable diseases. 14
As with general health, poor oral health contributes to social inequality, as disadvantaged communities have a greater burden of disease. Strategies to address oral health issues should therefore be undertaken in the framework of primary prevention and universal access to primary health care. 15 However, LMICs, especially India and several countries across the globe, fail to provide primary oral health care without any barriers. The recent statistics in India show that not even 20% of the rural primary health centers (PHCs) have a dentist available in the facility. The proposed plan of providing one dentist per PHC to cover 30 000 population is still a practicable goal to achieve. 16 Since oral health is an integral and essential part of general health and well-being, there is a great need to place oral health care in adjunct with general health and must be given importance the same way as has been given to general health especially to NCDs.
In this current scenario of expanding oral health care, one of the main challenges is to produce an eligible and trained dental health care planner. The other challenges are the lack of the oral health care surveillance system, lack of dentist in government local body meetings for decision–making, and making oral health affordable to all the public by providing dental insurance. Provision of some form of dental insurance significantly helps in managing the increasing costs of oral health care, and also encourages people to prioritize oral health and access the care without neglecting due to high costs and inaccessibility otherwise.
Oral Health Care Systems
The oral health care systems structure and function will vary markedly across different countries. The main purpose of the system is to improve the patient’s health. For a health care system to work effectively there should be good administration, equal proportion of health care workers to the population served, and facilities and well-equipped and advanced materials and instruments should be available for the treatment. 17
The oral health care system should function like the general health care system, were in it will focus on prevention, promotion, and disease control. Oral health care systems are influenced by the same factor as the general health care system, but are complicated due to the lack of importance given to oral health care services globally. The oral health services in both developed and developing countries primarily concentrate on diagnosis and treatment rather than the essential primary prevention and oral health promotion. Especially, South-Asian countries have a huge burden of oral conditions due to lack of provision of dentist in urban setup than in rural. Many of the countries worldwide are lacking in oral health policies thereby unable to design proper interventions and promotions for oral health.18,19 Data on disease prevalence are neither available nor disseminated due to the lack of economic resources and properly trained personnel. Most of the oral disease like dental caries, periodontal diseases, and gingivitis can be prevented by individuals by taking action for themselves and also for persons under their care to prevent disease and maintain health. 9
Opportunities exist to expand the oral disease interference and oral health promotion by providing information and practices to the general public through inculcating community programs in health care settings. The interventions in relation to oral diseases are not available and affordable due to escalating costs and limited resources leading to insufficient primary prevention of oral diseases which is being a challenge to many countries especially developing countries and also in countries where there is a transition in health care systems. 20 However, there is still disparity existing in oral health care services within regions and countries, where the oral health care is not fully integrated into national and community health programs. 21 We need to start thinking about the oral health in the same way as the wider community is beginning to think about NCDs. We should stop isolating oral health related diseases and ensure appropriate services available through existing health care systems.
Since health promotion and oral health prevention go beyond health care, improving quality of life, promotion, and prevention of oral diseases in the settings where people live, work, play, and learn are the most creative and cost-effective ways of enhancing and improving oral health. Interventions focusing on diagnosis and treatment of oral disease are high in cost especially in high-income countries, and sophisticated treatment is unavailable in LMICs leading to an increase in burden of oral diseases globally. However, these preventive and promotive oral health activities have been neglected in the public health system. 22
Global Oral Health Inequalities
Inequalities and its association with living conditions are the mainstreams in public health. This growing era of inequality based on gender, socio-economic status, and ethnic macro determinants are the major disparities on general health and overall well being. 23 The desire for healthy family, health society, and healthy country drives individuals and government alike. The government should pave way to provide equal opportunity for the people to access the health care services. Oral health inequity—inequitable access to oral health care services—has led to health inequity of the population.
There is only petite evidence on implementing the strategies to alleviate the inequalities in oral health globally. The health indicators are performing better in the more identical societies, and oral health status is deteriorated in society where there is inequity and also in disadvantaged groups. 17 Recently, we witnessed the development of new insights that are being developed into the contemporary patterns to address the oral health inequalities in both high- and middle-income countries. 24 Most of the dental strategies are aiming in reducing the diseases oriented to dental health by inculcating changes in the behaviors, which has unsurprisingly had a much less positive impact on oral health status. To maintain a good health status, policymakers should recognize these people who are in the disadvantaged groups (in social, political, and economic aspects) and provide access to health care services for a better living in the society.
When it comes to oral-health-related policy, the tendency has been to follow the approach suggested by the New Public Health movement, which involves adopting the Ottawa Charter for Health Promotion (WHO, 1986) and the total population approach. 25 There is an urgent need for strengthening of public health programs globally through effective oral disease prevention and health promotion. In addition, the common risk factor approaches should be used to integrate oral health into national health programs.
Based on Global Oral Health Inequalities: the Research Agenda’s (GOHIRA) recommendations on research barriers, 26 there are three major global inequalities that are obstacles in achieving a good oral health status namely, (a) gaps in knowledge, (b) isolating oral health from general health, and (c) inadequate evidence-based data.
As a whole, there is an increase in oral disease worldwide, but there is still inequality existing in oral health care services globally. Furthermore, the increased burden of oral conditions especially the dental caries and periodontal diseases among old age population is not being controlled effectively. This burden poses an urgent need to emphasize on oral health policy to enforce the already existing policies to improvise oral health and to reinforce the public health approach by addressing the common risk factors for oral health, and by mitigating inequality that is existing globally on oral health.
Conclusions
Oral diseases are one of the most prevalent diseases and yet they are neglected in several parts of the world. The oral health conditions have not been improved in the last 25 years and it has led to dramatic increase in untreated oral conditions across the globe. It is essential to strengthen the oral health policy and planning, in order to achieve the global oral health goals by the year 2020. The Port of Spain Declaration gave clear policy directions for an intersectoral approach which addresses many key risk factors ranging from tobacco, physical activity, healthy diet, health services, and surveillance. 27 There is a great need for collecting and updating data regarding oral health at national level to estimate the burden and monitor the progress. Integration of oral health with general health services would avoid duplication, and improving coverage through the collective actions is the key to tackle the growing epidemic of NCDs worldwide.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.