
Abstract
Background
Upper limb infections are common among patients with diabetes mellitus and their sequelae can be debilitating. They tend to present with severe infections but minimal symptoms probably due to neuropathy and vasculopathy among diabetics. The study aims to compare the demographic characteristics, clinical presentations and outcomes of upper limb infections between diabetic and non-diabetic patients.
Methods
All patients with upper limb infections who were admitted in a tertiary hospital from June 2017 to December 2020 were included in this study. Demographic data, clinical presentations, investigations and outcomes were obtained retrospectively from electronic medical record. There were 117 patients with diabetes mellitus and 127 with no diabetes mellitus. Comparisons were made between these two groups, and statistical analysis was done with SPSS.
Results
There were 244 patients included; 117 were diabetic and 127 were non-diabetic. Diabetic patients were more likely to present with emergent scenarios, especially necrotizing fasciitis and infective tenosynovitis (p < .05) with higher erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) readings (p < .05). Their microbiological cultures were less likely to be negative (p < .05). Diabetic patients also had poorer clinical outcomes with higher risk of amputation, re-operation and longer duration of hospital stay (p < .05).
Conclusion
Upper limb infections among diabetic patients should be treated aggressively. Early diagnosis and surgical intervention might decrease the morbidity and mortality in this group. Prevention of infections should be emphasized.
Introduction
Diabetes mellitus is one of the most common non-communicable diseases; the global prevalence among the adult population was 8.5% according to 2014 WHO global report on diabetes. 1 With its rising prevalence, it brings significant impact to the health care burden with direct increase in medical costs in managing the disease itself and its complications. It further affects the economy with loss of income associated with disabilities caused by the disease or its complications.2,3 Due to the state of immunodeficiency, diabetic patients are more susceptible to infections, including upper limb infections.4,5 Because of poor recovery, minor superficial infections may spread into deeper structures in upper limbs, causing massive tissue destructions or even sepsis.6,7
Although diabetic hand infections are less common than foot ulcers, the outcomes are often disappointing. 8 Diabetic patients tend to have more extensive infection, 9 longer time for recovery 10 and end up with amputation11,12 or death following sepsis. 7 Furthermore, the long-term morbidities that resulted from infection are more significant in diabetic patients. Inadequate or late treatment can result in severe stiffness, contracture and ultimately loss of hand function. 13 Thus, early diagnosis and urgent aggressive treatment should be given to diabetic patients who present with hand infections to prevent long-term morbidity and death.
There are many studies in literature reported on incidences and outcomes of hand infections. However, these were not comparison studies with non-diabetic patient population. The clinical presentations and managements of these two groups can be different. Thus, our study aimed to compare the demographic characteristics, clinical presentations and treatment outcomes between diabetic and non-diabetic patients who were admitted for upper limb infections.
Methods
All patients with upper limb infections who were admitted in the ward under Upper Limb and Reconstructive Microsurgery Unit, Department of Orthopaedic Surgery of a tertiary hospital from June 2017 to December 2020 were identified and included in our retrospective study. None of the patients had neurovascular deficit; thus, none were excluded. They were divided into two groups, patients with and without diabetes mellitus. Institutional medical research ethics committee approval was obtained (MREC: 2020714-8890).
Patient demographic characteristics, clinical presentation and microbiology results were obtained from the Electronic Medical Record (EMR). Demographic characteristics included were gender, age, body mass index (BMI), smoking status and comorbidities such as chronic kidney disease, hypertension, dyslipidaemia, gout and cardiovascular disease. Chronic kidney disease was defined as kidney damage or glomerular filtration rate (GFR) < 60 mL/min/1.73 m2 for 3 months or more, irrespective of cause. 14 Obesity was defined as body mass index of ≥ 27.5 kg/m2 according to Malaysian clinical practice guidelines on management of obesity published in 2004. 15
Clinical presentation variables that were recorded included side of upper limb affected, location of infection and diagnosis. Diagnosis was further categorized into emergent scenarios and non-urgent scenarios. Emergent scenarios that required urgent attention included necrotizing fasciitis, flexor tenosynovitis, deep hand infections (thenar, hypothenar and midpalmar abscess), septic arthritis and wet gangrene. Non-urgent scenarios included cellulitis, superficial abscess, animal bites, collar button abscess, fingertip infections (felon, paronychia), osteomyelitis and atypical infections.
For microbiological data, the number of organisms was recorded according to culture reports. Clinical outcome variables included readmission rate, sepsis rate, in-hospital mortality rate, the need of repeat surgery, the need of amputation and duration of hospital stay.
The data were summarized in tabular form, and statistical analyses were done using SPSS TM version 21 (SPSS Inc, Chicago, IL). For categorical data, chi-square test was used to calculate the p-value, and data were summarized in percentages. For continuous data, student t-test was used to calculate p-value for parametric data (age), and data were summarized in mean with standard deviation; Mann–Whitney U test was used to calculate the p-value for non-parametric data (number of comorbidities, white cell counts (WCC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and duration of hospital stay), and data were summarized in median with interquartile range for non-parametric data. A p-value of < .05 was considered as statistically significant.
Results
Demographic characteristics
Patient demographic and clinical characteristics.
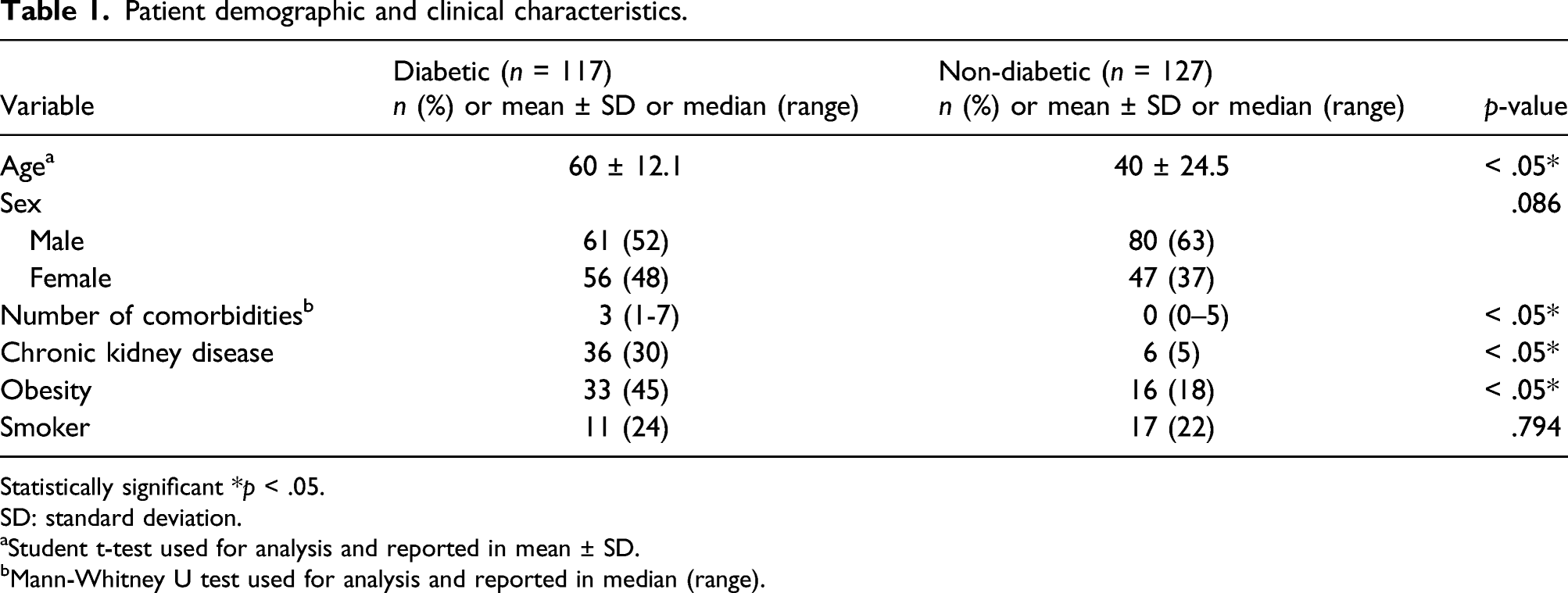
Statistically significant *p < .05.
SD: standard deviation.
aStudent t-test used for analysis and reported in mean ± SD.
bMann-Whitney U test used for analysis and reported in median (range).
Clinical presentations
Clinical presentations between diabetic and non-diabetic patients.

Statistically significant *p < .05.
CI: confidence interval.
aMann-Whitney U test used for analysis and reported in median (range).
Clinical outcomes
Clinical outcomes between diabetic and non-diabetic patients in ward.

Statistically significant *p < .05.
CI: confidence interval.
aMann-Whitney U test used for analysis and reported in median (range).
Discussion
We found that a higher percentage of diabetic patients with upper limb infections required hospital admission (48%) as opposed to non-diabetic patients; which is in contrast to previous studies which reported incidence of 5–25% only.10,17-19 Probably, this was due to the high prevalence of diabetes mellitus among Malaysian population; 3.9 million individuals reported in 2019. 20 Furthermore, we noticed that the random blood glucose level of diabetic patients upon admissions were not optimum, the mean dextrose value was 13.4 mmol/L with five other patients recorded as ‘HI’. This might reflect poorly controlled diabetes leading to complications of hand infections. A more reliable tool to measure long term glycaemic control is HbA1C, 21 but this data was not available in our EMR. Thus, HbA1c results were not included for analysis. The percentage of patients who were newly diagnosed with diabetes mellitus was 4% in our study compared to 25.7% and 31% reported in the literature.9,18
A study by Sharma et al. had shown that diabetic infections are more likely to present in proximal locations such as the forearm, 17 but there was no significant difference on site of infection between diabetic and non-diabetic patients in our study. We found that the diabetic patients were more likely to present with emergent scenarios especially necrotizing fasciitis and infective tenosynovitis. This could be due to the spread of infection to deeper tissues as diabetic patients remained asymptomatic at early stages due to neuropathy and poor healing potential due to angiopathy or vasculopathy. Surgeons should maintain a high index of suspicion that the infections could be more extensive in diabetic patients, 17 totally opposite to its benign appearance. Radiographs of the upper limb should be done to investigate for osteomyelitis 17 and urgent ultrasonography might delineate the extent of the lesions. Early and aggressive treatments of these severe infections might reduce the morbidity as well as mortality. Prompt diagnosis for necrotizing fasciitis is life-saving. 22 We also found that the ESR and CRP readings were significantly higher in diabetic patients, which can be attributed to the possible extensive nature of the upper limb infections at presentation.
The microorganisms in diabetic infections usually involve polymicrobial organisms from a wide range of pathogens including fungus.17,23 We noticed that this finding was consistent in our study, but the difference was not statistically significant compared to non-diabetic patients. However, in addition, we found that non-diabetic patients significantly showed ‘no growth’ in tissue culture and sensitivity test compared to diabetic patients
Generally, diabetic patients had worse clinical outcomes compared to non-diabetic patients. The amputation rates reported in literatures were 13.9%–39%.11,12,24,25 We found that amputations in upper limb infections were significantly higher in diabetic patients compared to non-diabetic patients (p < .05). The morbidity in these patients was significant as they suffer post-amputation pain and reduced quality of life. 26 Therefore, proper diabetic care and aggressive limb salvage treatments had to be sought for to prevent this end point. In addition, diabetic patients with upper limb infections required longer duration of stay in hospitals as they required multiple subsequent surgeries to achieve resolution of infection. The immunopathy in diabetes including neutrophil and monocyte dysfunction explained that diabetic patients needed longer time to eradicate infection. It also explained the higher incidence of re-operations and amputations. 4 Sharma et al. reported that poor in-patient glycaemic control resulted in the need for repeated drainages. 17 Furthermore, longer hospital stay was needed to manage the poor glycaemic control itself. Jalil et al. found that the length of hospitalization correlated with severity of infection. 6 We found the incidences of sepsis, mortality and readmissions were higher in diabetic patients but they were not statistically significant compared to non-diabetic patients.
There were limitations in this study. The data collected was retrospective and dependent on clinical notes. Some data were missing including status of smoking in 123 patients, and data were missing on obesity in 81 patients, WCC in three patients, and ESR and CRP in 128 and 86 patients, respectively. HbA1c readings and fasting blood glucose levels were not available in our EMR. Thus, the level of glycaemic control in diabetic patients could not be properly assessed. Besides that, this study was based on a single tertiary centre, and thus, the results may not reflect the whole population. This observational study was only a comparison between diabetic and non-diabetic patients who were admitted for upper limb infections. The fact that other co-morbid conditions, for example, chronic kidney disease could have resulted in or altered our clinical outcomes as well, as the diabetic and non-diabetic groups were not completely comparable. Risk factor analysis via multivariate logistic regression could not be done.
Conclusion
Upper limb infections can be severe among patients with poorly controlled diabetes mellitus. Early diagnosis and aggressive surgical intervention may decrease the morbidity as well as mortality. These groups of patients must be educated on the importance of prevention of infections.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.