
Abstract
Purpose
The direct anterior approach (DAA) for total hip arthroplasty (THA) can be performed with patients in either in the lateral decubitus or supine position. Prompted by the lack of studies addressing differences between the two positions, this investigation aimed to examine clinical and radiographic outcomes and compare the lateral decubitus versus the supine position for THA using the DAA.
Methods
Between January 1 and October 1, 2020, 90 patients who underwent primary unilateral THA using the DAA were recruited, with 54 (60%) undergoing THA in the supine position (SP group) and 36 (40%) in the lateral decubitus position (LP group). Technical information, clinical and radiographic outcomes, and patient-reported outcomes, including the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and Short-Form-12 (SF-12) were evaluated. All data were subjected to several statistical tests.
Results
There were no preoperative differences in baseline characteristics between the LP and SP groups, which were also similar in terms of operative duration, length of hospital stay, and blood loss. Radiographic assessment confirmed satisfactory positioning of the prosthesis in both groups. There were no significant differences in terms of CK-MB and hemoglobin levels, Harris Hip Score, WOMAC, UCLA, visual analog scale score, and SF-12. The incidence of complications in the LP group was lower than in the SP group.
Conclusion
Total hip arthroplasty performed via DAA in the LP and SP groups yielded excellent clinical outcomes, although the incidence of complications in the former was lower than in the latter.
Introduction
Total hip arthroplasty (THA) is regarded to be one of the most successful and reliable procedures for restoring function and reducing pain, consequently improving the quality of daily life for patients with end-stage hip joint disease. 1 However, the choice of appropriate surgical approach for THA remains controversial.2,3 Recently, the direct anterior approach (DAA) was recommended owing to less muscle damage, a lower rate of dislocation, and faster recovery.4-7
The DAA was conventionally performed with patients in the supine position using a Hana table or an ordinary operating table capable of folding during surgery. Nevertheless, DAA could also be performed with patients in the lateral decubitus position. Melman et al. described their first experience with DAA in the lateral decubitus position in 172 patients and reported promising clinical results. 8 Min Chen et al. also reported their experiences and early results of DAA in the lateral decubitus position, demonstrating that it may be a valuable alternative in the absence of a special operating table and yielded satisfactory clinical and radiographic outcomes. 9
However, there is an obvious absence of published studies addressing differences between the two positions, for which surgical positioning for THA may be more conducive to recovery, technically more demanding, associated with component malposition, or more complications. Therefore, the aims of this study were to examine the clinical and radiographic outcomes and distinguish between the DAA for THA in the lateral decubitus versus the supine position.
Materials and methods
A prospective, randomized clinical trial was designed at the authors’ hospital to compare clinical and radiographic outcomes between the DAA in the lateral decubitus (LP group) and the supine (SP group) positions for primary unilateral THA, with at least a 6-month follow-up. Patients with end-stage hip joint disease and indications for THA were recruited. Individuals with severe obesity (body mass index [BMI] > 40 kg/m2), those who underwent previous hip procedures with retained hardware, those with severe deformity of the femur, posterior acetabular deficiency, stiff hip, Crowe type III/IV developmental dysplasia of the hip, and patients intolerant to the operation, or could not be followed up were excluded. All eligible patients provided written informed consent before undergoing surgery. Both patients and investigators evaluating the clinical outcomes were blinded to the allocated treatment.
For each patient, a comprehensive physical examination was performed, and medical history was recorded, including demographic data. Surgical duration, perioperative blood loss, muscle injury, length of hospital stay, and intraoperative and postoperative complications were assessed. Standard anteroposterior radiographs of the pelvis and lateral radiographs of the femur were obtained for all patients preoperatively, immediately postoperatively, and at the latest follow-up to compare differences in component position (such as offset and cup abduction) and leg length discrepancy (LLD) between the two groups. Moreover, multispectral CT was performed to evaluate component position and alignment, especially for femoral and acetabular or cup anteversion.10,11 Additionally, the Harris Hip Score (HSS), the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), visual analog scale (VAS) score, the University of California at Los Angeles Shoulder Rating Scale (UCLA), and the Short-Form-12(SF-12) were obtained preoperatively, 2 and 4 weeks’ postoperatively, and the latest follow-up were used to assess the clinical results of the procedure.
All procedures were performed by a single high-volume orthopedic surgeon who did not participate in the follow-up. Clinical and radiographic outcomes were calculated by another well-trained orthopedic surgeon who was blinded to the study. In other words, both patients and researchers evaluating the clinical outcomes were blinded to the allocated treatment. Total hip arthroplasty was performed using the DAA with patients in the lateral decubitus or supine position using a standard surgical procedure.8,9,12
Surgical procedure
Patients underwent THA performed using the DAA in either the lateral decubitus or supine position. The DAA, or modified Hueter approach, to THA, based on the Smith–Peterson approach, has been described by many authors.13-16 Before initiation of this randomized clinical trial, the surgeon had performed > 100 THA procedures using the DAA either in the lateral decubitus position or supine position per year. The surgeon has many years of surgical experience using the DAA, operating on a mean of 150 hips per year using the DAA instead of the posterolateral approach. Patients who underwent THA in either the lateral decubitus or supine position were compared in terms of surgical duration, length of hospital stay, blood loss, muscle damage, prosthesis position, and complications.
Statistical analysis
Homogeneity of variance and data normality were tested before statistical analysis. Pearson’s chi-squared test was performed for normally distributed variables (sex and surgical site). An independent samples t-test was used for normally distributed variables(age, BMI, surgical duration and length of hospital stay). The Mann -Whitney U test was used for non-normally distributed variables(blood loss). Hemoglobin (Hb), CK-MB, HSS, WOMAC, SF-12, femoral anteversion, cup abduction, cup eversion, and offset values were tested using a GLM repeated measurement analysis. Visual analog scale and LLD were analyzed using generalized linear mixed model analysis. Analyses were performed at an alpha level of 0.05; differences with p < .05 were considered to be statistically significant. Data are expressed as mean ± standard deviation (SD). All statistical analyses were performed using SPSS version 20.0 (IBM Corporation, Armonk, NY, USA).
Results
Patient characteristics
Baseline characteristics.
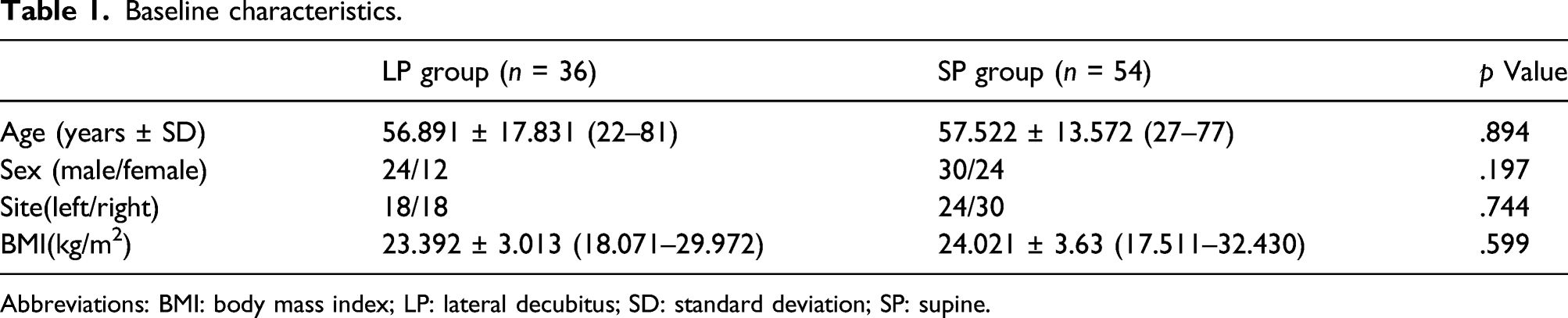
Abbreviations: BMI: body mass index; LP: lateral decubitus; SD: standard deviation; SP: supine.
Intro-Operative outcome
Intro-operative outcome.

Abbreviations: LP: lateral decubitus; SD: standard deviation; SP: supine.

Comparison of surgical duration between LP and SP group. The standard deviation is indicated by error bars, positive for LP group and negative for SP group.
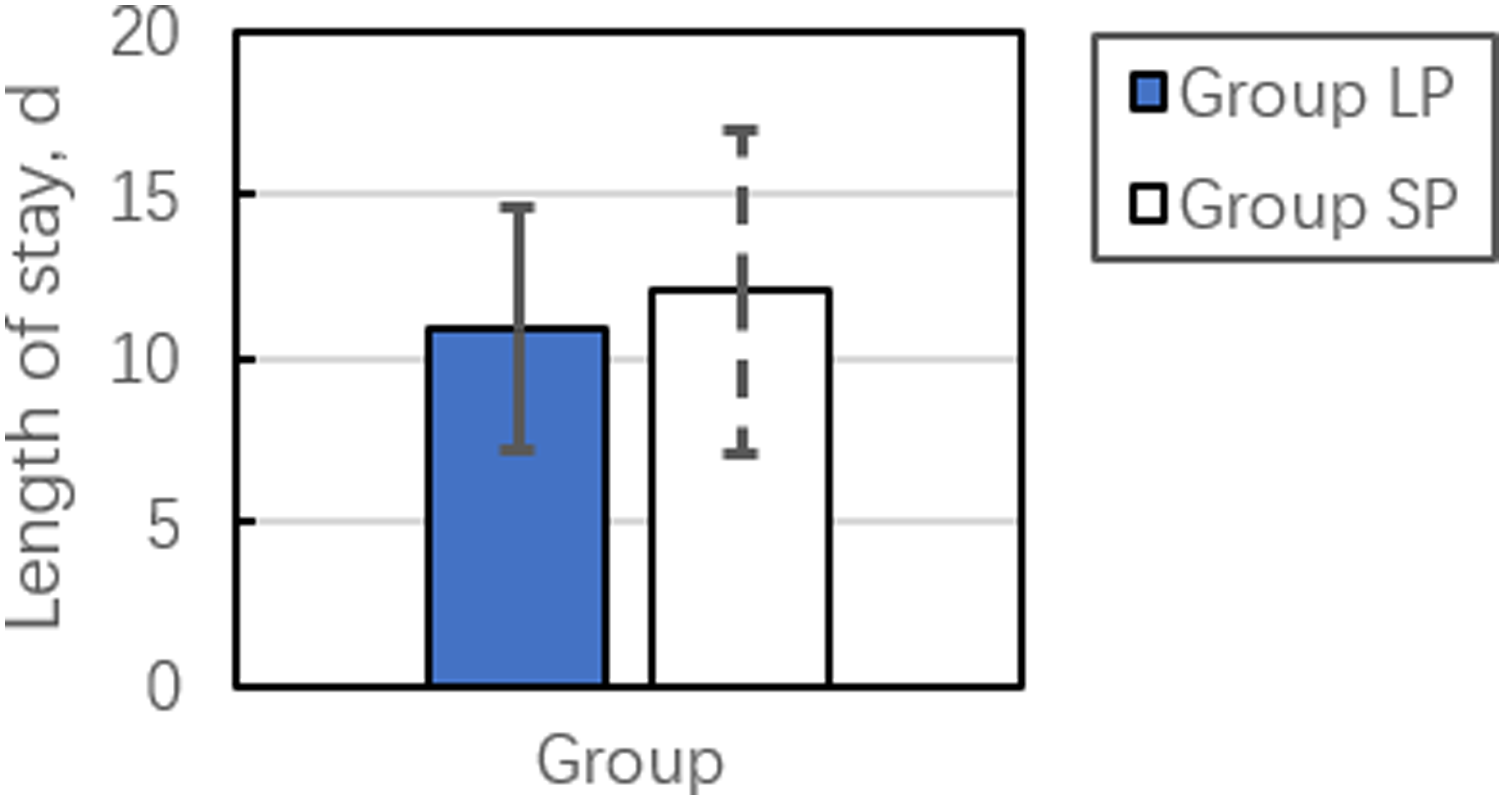
Comparison of length of hospital stay between LP and SP group. The standard deviation is indicated by error bars, positive for LP group and negative for SP group.
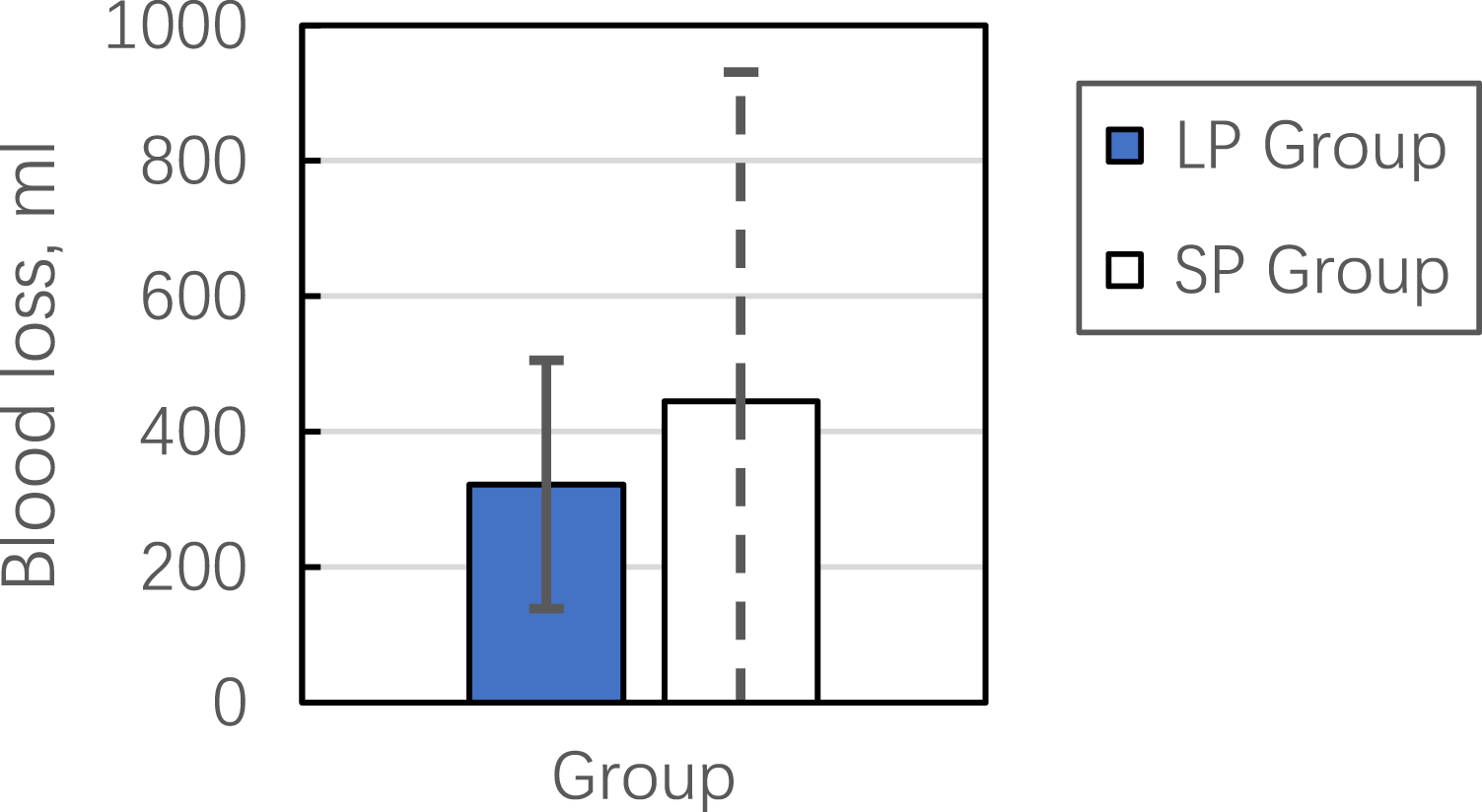
Comparison of blood loss between LP and SP group. The standard deviation is indicated by error bars, positive for LP group and negative for SP group.
CK-MB and Hb levels
The value of Hb and CK-MB.

Abbreviations: LP: lateral decubitus; SD: standard deviation; SP: supine.
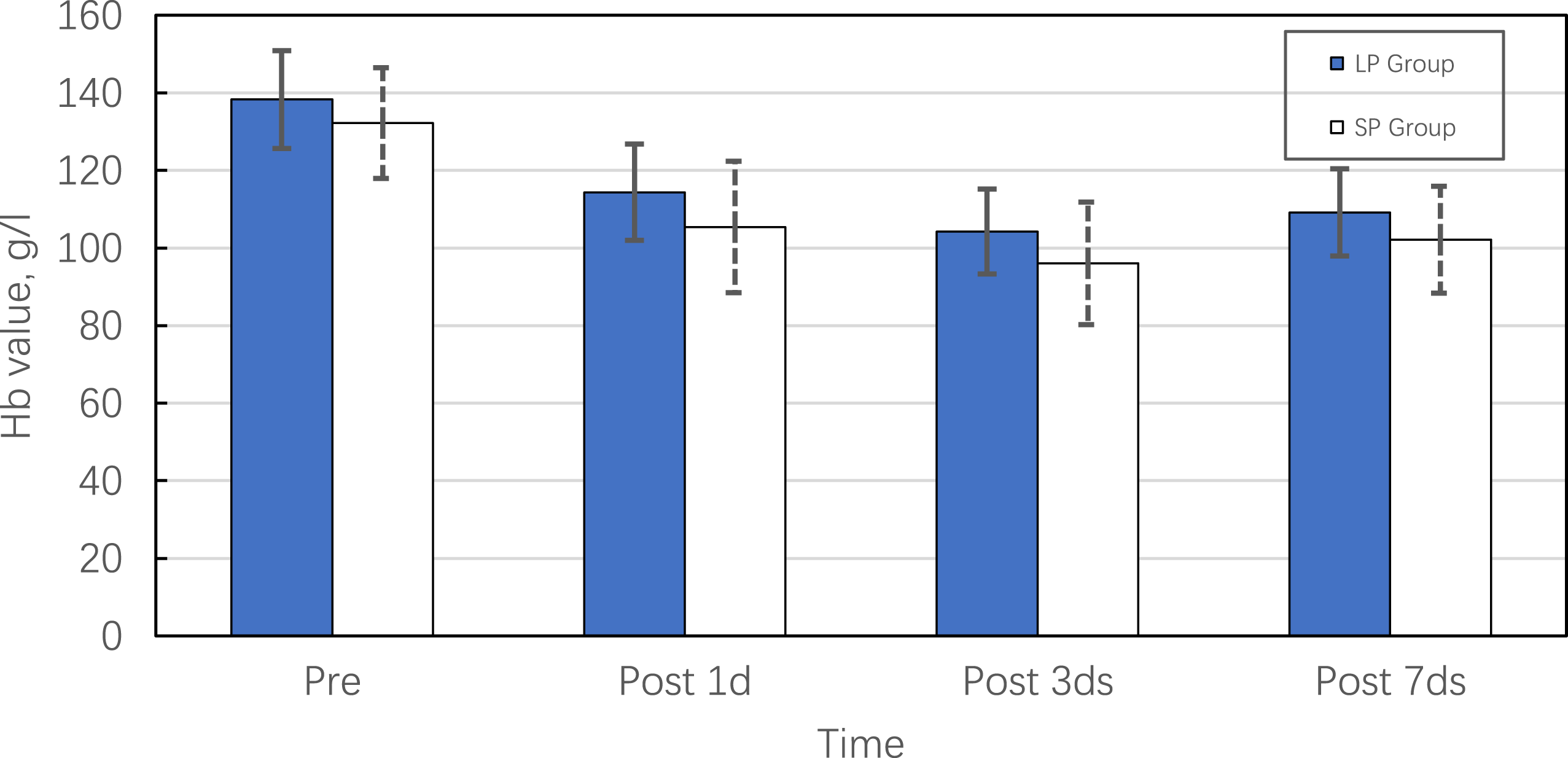
The course of Hb as a function of time for LP group and SP group. The standard deviation is indicated by error bars, positive for LP group and negative for SP group.

The course CK-MB as a function of time for LP group and SP group. The standard deviation is indicated by error bars, positive for LP group and negative for SP group.
Clinical scores
Clinical outcome.

Abbreviations: HSS: Harris Hip Score; LP: lateral decubitus; SF-12: Short-Form-12; SP: supine; UCLA: University of California at Los Angeles; VAS: visual analog scale; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
Radiographic outcomes
Radiographic outcome.

Abbreviations: FA: femoral anteversion; LLD: leg length discrepancy; SP: supine.
Complications
Complications.

Abbreviations: LP: lateral decubitus; SP: supine.
Discussion
In the present study, we confirmed that THA performed via DAA with patients in the lateral decubitus and supine positions yielded excellent clinical outcomes. Few studies have directly compared these two different positions for THA using DAA, although one reported that the lateral decubitus position had the advantages of shorter surgical duration and less blood loss; however, prospective studies were more convincing than retrospective studies. 13
Nevertheless, we can still draw conclusions based on the results of previous studies. Supine is the position in which most surgeons begin to learn the DAA. To reduce surgical duration, the lateral decubitus position should be avoided in patients undergoing bilateral THA at the same time. Patients undergoing the procedure in the supine position are positioned only once to complete the operation, which greatly reduces surgical duration. Surgery performed with the patient supine is advantageous in terms of anesthesia. Moreover, C-arm use is facilitated and image capture is more accurate. Theoretically, it is easier to anatomically locate the position of the pelvis, and acetabular cup implantation is more accurate. 17 The traditional position for classic posterolateral surgery is the lateral decubitus position. When the operative limb is in overextension, abduction, and external rotation, it is more likely to expose the femur and enter the medullary space, which can reduce the incidence of complications. In the lateral decubitus position, abdominal adipose tissue falls away from the incision and surgical field due to gravity. In addition, the lateral decubitus position causes changes in pelvic orientation that may affect implantation of the acetabular prosthesis, whereas in the supine position, there are less severe changes in pelvic orientation.8,9,18 Pelvic positioning is more reliable with the patient supine, and results in more consistent orientation of the acetabular component. 19
Among our cohort, operative data (i.e., surgical duration, length of hospital stay, blood loss, CK-MB, and Hb levels) demonstrated no statistically significant differences between the LP and SP groups. This could be due to the fact that DAA is a minimally invasive surgery with a small incision and involves a muscle gap approach, which results in less injury and bleeding. Despite this, compared to the lateral decubitus position, surgery in the supine position has a longer average surgical duration by approximately 20 min (Table 2, Figures 1–3). Our results demonstrated that the length of hospital stay and blood loss among patients who underwent surgery in the supine position had longer and greater average values, respectively, than those in the lateral decubitus position. We believe that longer surgical duration is partly associated with a longer length of hospital stay and more blood loss. Some authors believe that in the lateral decubitus position, the soft tissue around the incision can make full use of the advantages of gravity to expose the surgical area better and reduce blood loss.20,21 Of course, we still need further research to investigate whether the lateral decubitus position reduced blood loss and muscle damage.
There is no evidence that either the lateral decubitus or supine position favor faster recovery after THA using DAA. Although no difference was observed in clinical scores between these two groups in our study, all patients achieved significantly excellent functional scores and experienced improved quality of life during the latest follow-up.
We measured cup abduction, cup anteversion, LLD, femoral anteversion, and offset as described by Lewinnek, acceptable cup abduction was defined to be between 30° and 50°, and acceptable cup anteversion angle was defined to be between 5°and 25°. 22 In our study, postoperative radiological outcomes demonstrated that the prosthesis in these two groups was well positioned. Leg length discrepancy values were equal to the operative side minus the other side, which was denoted as positive if the operative extremity was longer than the contralateral side, while a smaller offset was regarded as a significant risk factor for lateral femoral cutaneous nerve injury following THA via DAA.23,24 Although there were no statistical differences in radiographic outcomes, in terms of functional recovery, it has yet to be established which radiographic data are most important and which parameter is most meaningful.
A few complications occurred after the operation (Table 6). In the lateral decubitus position, only one case of dislocation occurred postoperatively. In the supine position, one case of dislocation and one case of greater trochanter fracture occurred intraoperatively, three cases were due to difficult exposure during surgery, one case of unexplained persistent fever, and one case of poor hip functional flexion occurred postoperatively. Two patients experienced postoperative dislocation: a 59-year-old male (BMI, 21.2 kg/m2) and a 57-year-old female (BMI 25.1 kg/m2). Both presented as posterior dislocation of the hip caused by inadvertent roll-over after discharge. Both patients were treated with manual reduction under anesthesia, followed by fixation with nail shoes for 2–3 weeks. Although it is theoretically considered that the dislocation rate of DAA is lower than that of other approaches, dislocation can still occur in both positions. One case of greater trochanteric fracture occurred during the exposure process, which was believed to be caused by osteoporosis. We consider that unexplained persistent fever is related to a patient’s previous history of chronic osteomyelitis. Nevertheless, the results demonstrated that the incidence of complications in the lateral decubitus position was lower than that in the supine position, although a larger sample is required to confirm this result.
There were some limitations to the present study, the first of which were the small sample size and relatively short duration of follow-up. However, to the best of our knowledge, few prospective randomized trials have compared THA performed using the DAA in the lateral decubitus or supine positions. Nevertheless, studies with a longer follow-up are needed to examine whether the DAA in the lateral decubitus position is superior or equivalent to that in the supine position. All procedures in our study were performed by the same surgeon. While this enabled us to avoid the effects of varying surgical skill among different surgeons, our results should be verified and extended in a study including multiple randomized surgeons.
Conclusion
Both THA performed using the DAA with patients in the lateral decubitus position or supine position yielded excellent clinical outcomes, although the occurrence of complications among those who underwent the procedure in the lateral decubitus position was lower than in those undergoing the procedure in the supine position.
Footnotes
Declaration
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent to participate
Informed consent for all participants have been obtained, and identifying details of the participants will not be published in written descriptions.
Consent for publication
All authors declare that they agree to publish.
Availability of data and material
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
The statistical software used in this paper is the SPSS software 20.0.