
Abstract
Purpose
Giant cell tumour (GCT) of the bone is a benign but locally aggressive tumour, commonly occurs at the metaphyseal–epiphyseal junction of the distal femur, proximal tibia, and distal radius. For Campanacci grade II and III lesions of the distal radius and in cases of recurrence, we usually carry out wide resection and reconstruction. There are numerous publications on the treatment of GCT of the distal radius. Still, reports on the functional outcome using non-vascularized fibular graft arthroplasty without fusion remain limited.
Method
We reviewed patients who underwent wide resection and non-vascularized fibular graft arthroplasty from 2007 to May 2014. The assessment was done with Musculoskeletal Tumour Society Score (MSTS), Toronto Extremities Scoring System (TESS) and Disability of the Arm, Shoulder and Hand (DASH) scores. We also reviewed the radiographic results.
Results
Fifteen patients were recruited, of whom 10 cases used ipsilateral fibular graft and five used contralateral non-vascularized fibular graft. The average duration of follow up was 6 years (3.25–9.92 years). The average grip strength was 48.1% compared to the non-operated hand. The average MSTS score was 78.4 %, TESS score was 84%, and DASH score was 25.2. The average time to radiological union was 12.5 weeks. 64% (29–78%) of the range of movement is preserved compared to the normal side. The complication rate was 20%.
Conclusion
Fibula autograft arthroplasty is a feasible method of reconstruction after distal radius resection with good functional outcomes.
Introduction
Giant Cell Tumour (GCT) of the bone is a locally aggressive lesion with a high tendency for local recurrence. 1 The distal radius is the third most common site for GCT occurrence and it also has the highest incidence of recurrence.2,3 These tumours are graded via the Campanacci grading system. Grade I, the tumour, is confined within the bone; Grade II is where the bone is expanded, and Grade III is where the tumour has broken through the cortex with soft tissue extension. 4 Therefore, Campanacci Grade II and III tumours in this region are generally treated with wide local resection and reconstruction.5,6 The reconstruction options described in the literature include vascularized and non- vascularized osteoarticular fibular arthroplasty or arthrodesis,7–9 use of allograft 10 or osteoarticular allograft, 11 the fusion of wrist with iliac crest autograft 12 and transposition of the ulna with the fusion of wrist.13,14 We describe our series of patients treated with non-vascularized fibular graft arthroplasty.
Material and methods
This is a retrospective review of patients who underwent wide resection of distal radius and reconstruction with non-vascularized fibula graft arthroplasty from 2007 till 2014, with a minimum follow-up of three years. We recruited only patients with primary tumour at their first presentation for this study, excluding patients with recurrent disease. We identified suitable patients from our orthopaedic oncology database. They were then assessed in the clinic by the principal investigator during follow up where the following parameters were measured and compared to the unaffected contralateral limb; the range of motion (measured with a goniometer) and grip strength (measured with Jamar hydraulic dynamometer; model no. 5030J1). All measurements were made in triplicates, and the average was taken. Functional scores were evaluated with modified Musculoskeletal Tumour Society Score (MSTS), Toronto Extremities Scoring System (TESS) and Disability of the Arm, Shoulder and Hand (DASH) scores. Serial radiographs taken during follow-up were assessed by the investigators and reported by a radiologist to determine the time of union and radiological progress of replacement. Union is defined as bridging callus on at least three cortices on Anterior-Posterior and Lateral views of plain radiographs. Subluxations, dislocations and radiocarpal joint narrowing were measured three years post-surgery. We obtained ethical approval from the institutional review board and took informed consent from all subjects involved in this study.
Surgical Procedure
The same operating team performed the surgical procedure for every case. A pneumatic tourniquet is applied to both the operated limb and the donor’s leg. In most cases, the ipsilateral fibula was harvested but, in some cases, the contralateral fibula was used based on the surgeon preference after discussing with the patient. The approach used for the distal radius was either an isolated volar or combined volar and dorsal approach depending on the dorsal extension of the tumour into soft tissue.
The distal radius and the surrounding soft tissue were carefully dissected without spillage or breakage into the tumour. We routinely sacrifice pronator quadratus, as in the majority of cases, the tumour breaches the volar cortex of the distal radius and is contained by this muscle. The distal margin of resection was the radiocarpal joint and extrinsic radiocarpal ligaments, and the proximal margin was 3 cm–5 cm of normal bone (Figure 1). The tumour did not breach the radiocarpal joint in any of the cases. (a) All images are of the same patient in sequence showing left wrist swelling on the radial side extending to volar aspect. Radiograph showing Campanacci grade 3 lesion. (b) MRI shows a relative homogenous appearance of the tumour and there is cortical break with soft tissue extension. (c) The tumour resected out with pronator quadratus. A non-vascularized fibula graft with non-locking DCP. (d) Volar and dorsal aspect of the left wrist post resection of tumour. Fibula graft plated to the native bone (remnant radius). K-wires used to stabilise the fibula ulna joint and the fibula carpal joint.
As for harvesting the proximal fibula graft, the incision is made laterally over the fibula. The fibula is approached posteriorly to peroneal longus muscle. The common peroneal nerve is routinely identified and lifted anteriorly together with peroneal longus muscles. The fibula graft length is based on resection length. It is harvested with a small stump of fibula collateral ligament. The remnant of the lateral collateral ligament is anchored down to the soft tissue around the tibia to prevent lateral collateral ligament laxity of the knee joint.
The fibula graft is routinely trimmed 2 mm–3 mm shorter than the resected bone and inserted into the resection bed and rotated until it is positioned comfortably; the fibula carpal joints were stable and did not subluxate. All patients were purposely given a positive ulnar variance by shortening the donor fibula to allow better fibula carpal joint stability. The rotational alignment was marked with diathermy on both proximal fibula and proximal radius to determine the alignment for plating. The fibula is then plated to the radius with a 6-hole narrow Dynamic Compression Plate (DCP). A periosteal sleeve is kept from the resected bone and advanced over the host bone fibula junction during the plating. The remnant fibula collateral ligament is repaired to the carpal ligament. K wires are used to stabilise the fibula ulna joint and the fibula carpal joint. These wires are kept in situ for six weeks. There is no soft tissue reconstruction done for the distal fibula ulna articulation. The tourniquet is then released, and haemostasis secured. Finally, a single surgical drain is inserted, and the wounds are closed with interrupted sutures.
Postoperative protocol
A thermoplastic ulna gutter splint is applied in neutral position and kept for six weeks. Sutures are removed at two weeks, and the Kirschner wires at six weeks (Figure 2). After which, patients continued to wear the splint for another six weeks as night splints and physiotherapy is initiated. Regular usage of the arm is allowed after three months, and patients are advised against heavy lifting (anything more than 10 kg) and doing strenuous activities. Postoperative radiograph at six weeks (Kirschner wire removed).
Results
Summary of demography, approach and radiological findings.

The mean resection length of distal radius was 7.89 cm (range: 5–12 cm; SD ± 1.07). In seven cases, the volar approach was used in isolation, and in eight patients, a combined volar and dorsal approach was used.
The fibula carpal joint was reduced in 27% of subjects (assessed both radiologically and clinically), while 53% had less than 0.5 cm subluxation (Figure 3) and 20% had ≥0.5 cm subluxation of the joint. There were no dislocations of the joint. The fibula ulna joint was intact in all 15 cases. 60% had <2 mm joint space narrowing of the fibula carpal joint. Union rate was 93.3% (n = 14) and the average time to union was at 12.5 weeks (range: 5.6–27.9; SD + 7.2). Shows and example of fibula carpal joint subluxation.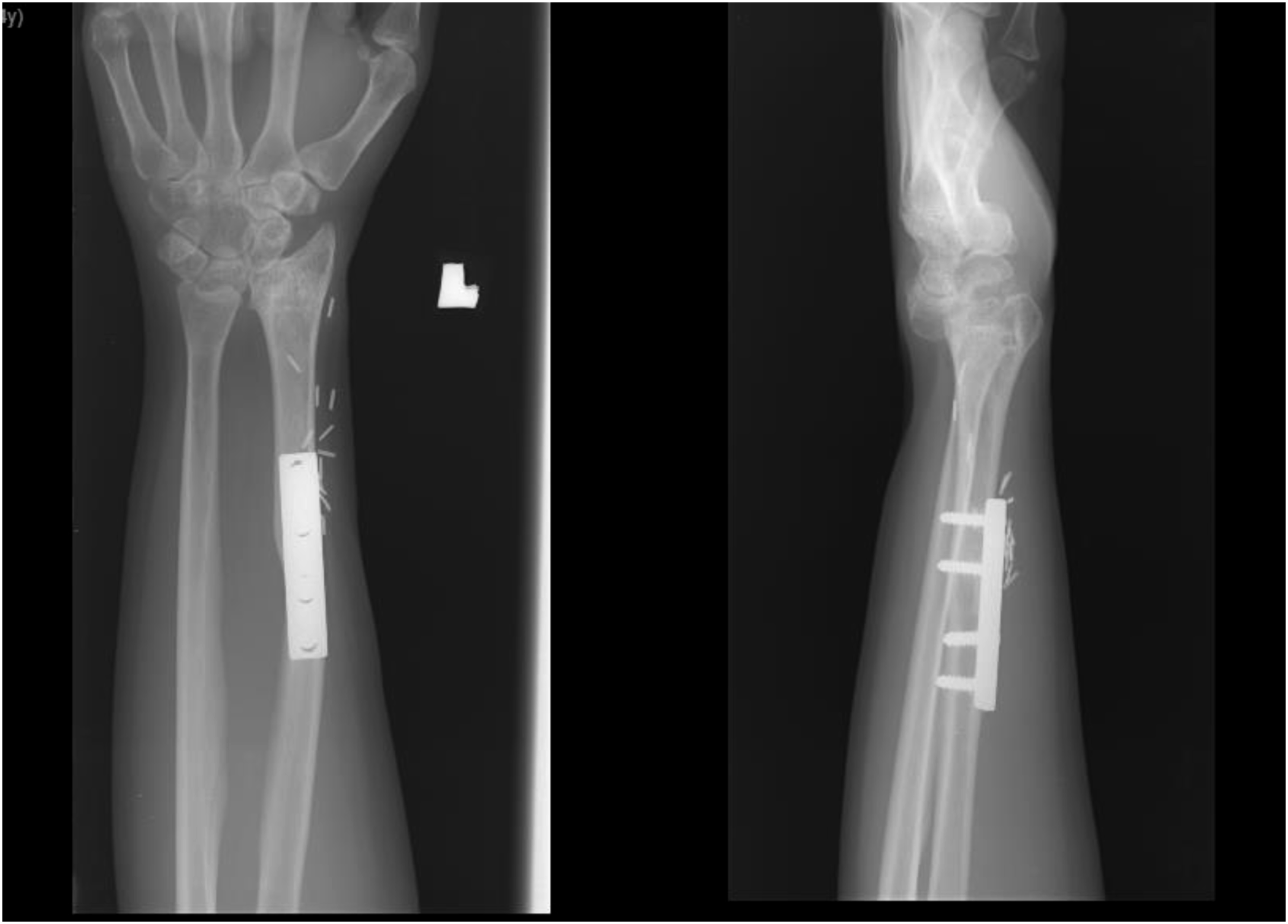
Summary of functional outcome.

*Percentage loss is in relation to the contralateral limb.
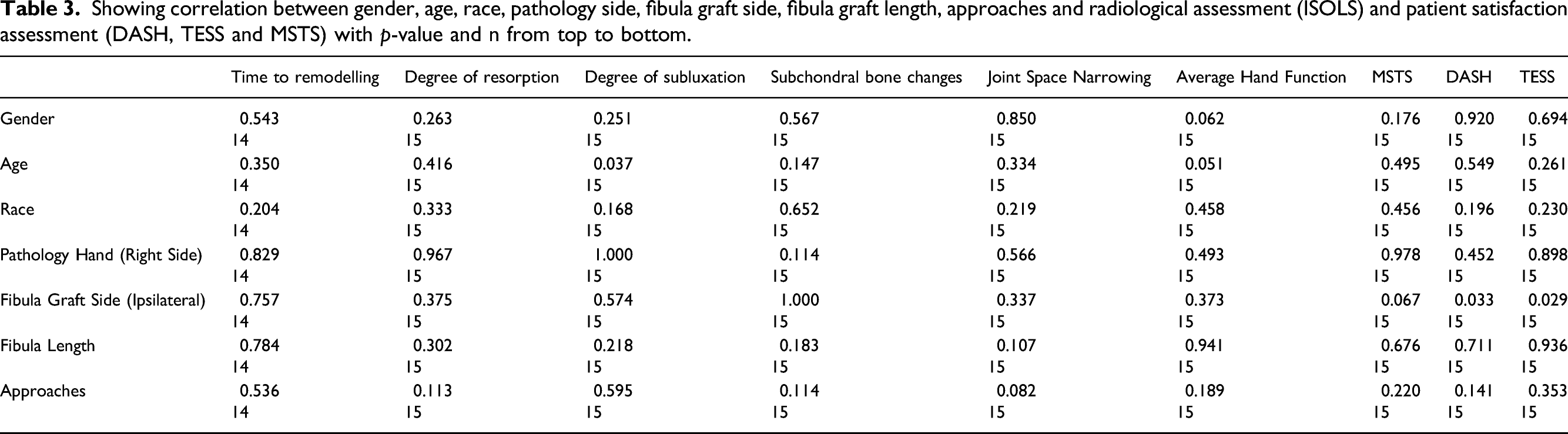
Showing correlation between gender, age, race, pathology side, fibula graft side, fibula graft length, approaches and radiological assessment (ISOLS) and patient satisfaction assessment (DASH, TESS and MSTS) with p-value and n from top to bottom.
We had one case of infected non-union, which was treated with debridement and external fixator followed by iliac crest bone grafting and fusion of the wrist. There was another case of graft collapse secondary to bony recurrence and subluxation of the fibula carpal joint. It was treated with a vascularized fibula graft from the opposite side. However, this graft eventually fractured distal to the plate. It was treated with plate removal and splinting. It eventually united with slight bowing and subluxation of the fibula carpal joint (Figure 4). One case of iatrogenic common peroneal nerve injury resulted in numbness and deep peroneal nerve distribution and inability to dorsiflex the big toe. It did not improve throughout the study. There was only one case of bony local recurrence (as noted above) and no cases of soft tissue recurrences. Shows series of radiograph for patient 7 (a) Immediate postoperative radiographs. (b) Well incorporated fibula graft (non-vascularized). (c) Bony recurrence within the graft with subluxation of wrist joint. (d) Revised with vascularized fibula graft. (e) Peri-prosthetic fracture of the vascularized fibula graft. (f) Union of the vascularized fibula graft after removal of plate and splinting. The close-up radiograph shows subluxation of the wrist.
These complications did not have a significant bearing on MSTS (p = 0.102) and DASH (p = 0.115) scores and grip strength (p = 0.551), but it significantly affected the TESS scores (p = 0.002). Figure 5 shows radiographs of patient 6 from presentation till the recent radiograph taken five years after the index surgery and the recent functional pictures. Shows patient no 6 (a) is the preoperative radiograph (b) is the recent postoperative radiograph (5 years and (c) shows clinical pictures of flexion, extension, pronation and supination.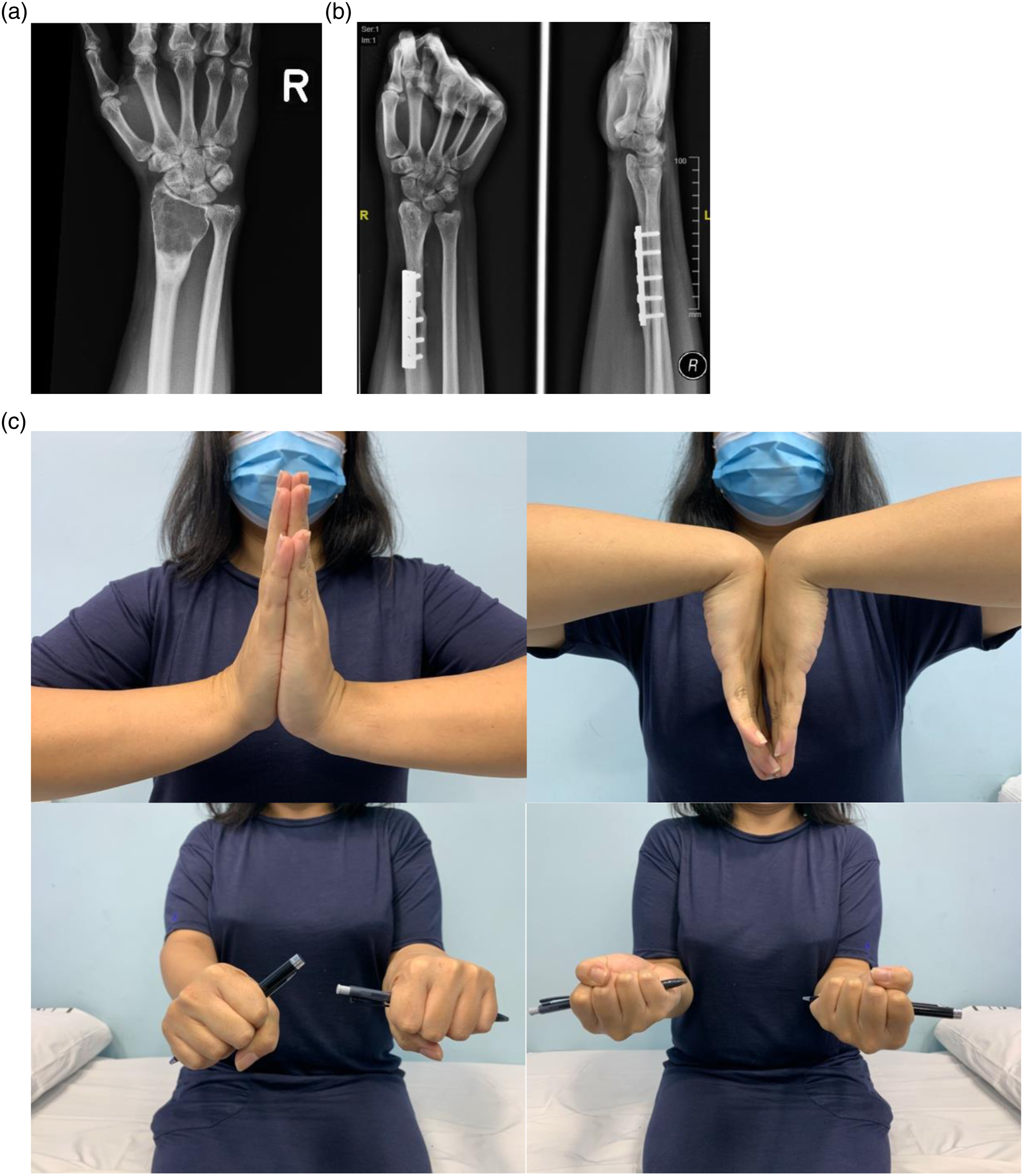
Discussion
The giant cell tumour of the bone is a locally aggressive lesion with a local recurrence rate of 0–65% depending on the grade of the tumour (Campanacci) and chosen treatment method. 15 Campanacci grade II and III tumours are generally treated with wide resection and replacement with or without wrist fusion (arthroplasty or arthrodesis) as the local recurrence rate for an intralesional procedure is high.16–18
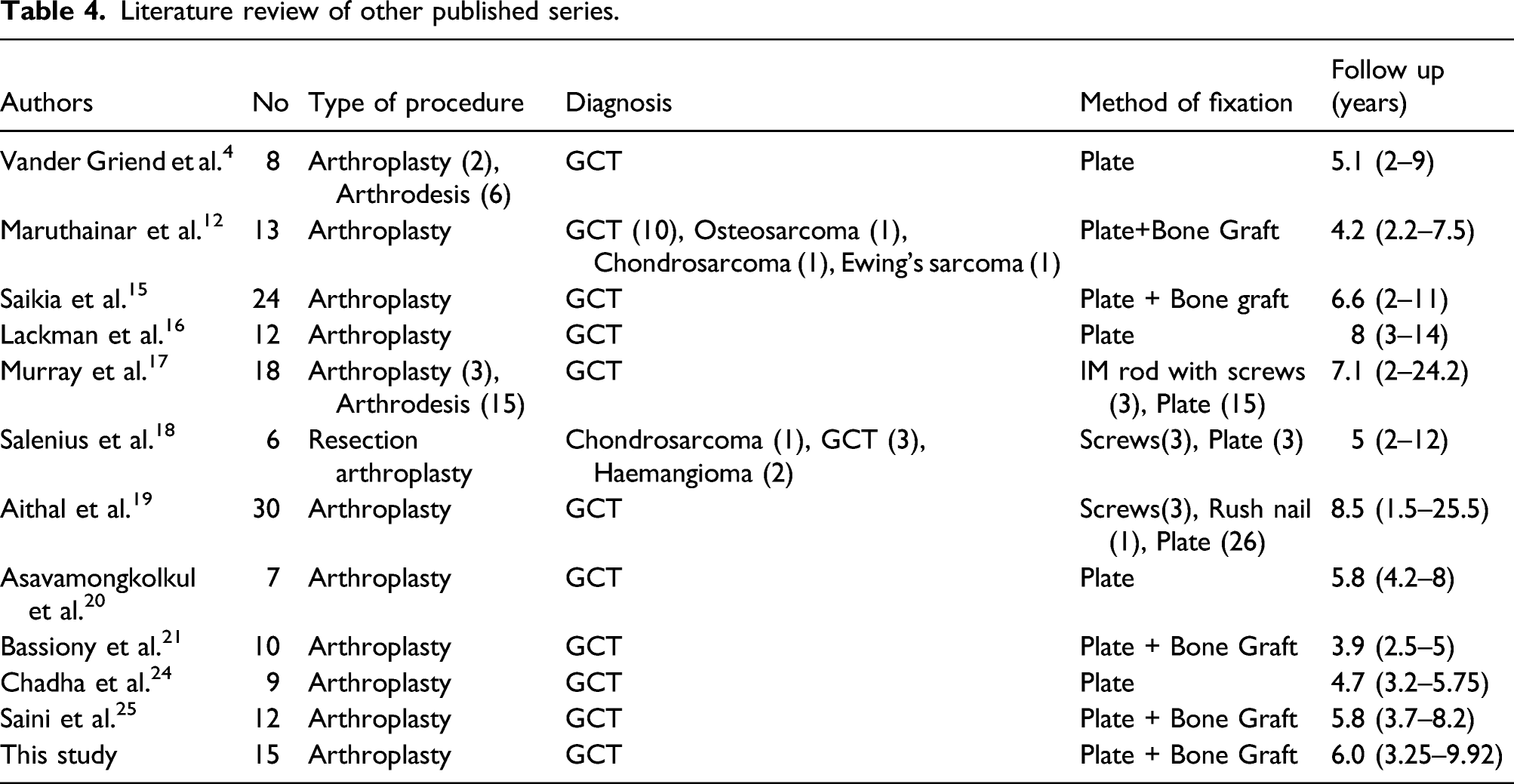
Literature review of other published series.
We prefer the volar surgical approach in resecting these tumours. Still, in almost half the cases, a combined volar and dorsal approach was used to ease resection as there was dorsal extension of the tumours. A combined dorsal approach allows us to release the dorsal extensor tendons from the dorsal compartments via direct visualisation and avoids spillage of the tumour due to tumour breakage.
We used ipsilateral fibula in two-thirds of the cases in this series and contralateral fibula in one-third of the patients. Although it is more convenient for two operating teams to operate on opposite sides of the patient, we prefer harvesting the ipsilateral fibula. This is because we realised that the ipsilateral fibula is more compatible anatomically than the contralateral fibula in terms of the fibula carpal joint’s stability. Furthermore, we have shown that patients with ipsilateral fibula have a better functional score (DASH and TESS scores).
Comparing publications with a large series in the literature with this study.

DF: Dorsi flexion; PF: Palmar flexion; Su: Supination; Pr: Pronation; NA: Not available.
Salunke et al. 13 reported 25 cases, and Puri et al. 14 reported 14 patients with GCT distal radius treated with resection and reconstruction with ulna transposition and fusion. Their MSTS scores were 80% and 87%, respectively. These scores are similar to our study, but their reconstruction form sacrificed the flexion and extension movement of the wrist. These authors cited the advantage of better union rates at the host bone graft junction (6.5 months and 4.9 months, respectively) as their graft was vascularized. However, the host graft junction’s union rate in our study was shorter despite utilising a non-vascularized graft. Our study’s union rate is 93.3% (n = 14), and the average duration for the radiological union was 12.5 weeks. The earliest radiological union was documented at 39 days. This may be due to the periosteal sleeve advanced to cover the host bone and graft junction. It may induce bone healing. There was only one case of non-union due to infection. Liu S et al. 29 reported a mean union time for non-vascularized fibula graft of 30.5 weeks, and Humail SM 30 reported a mean radiological union at 16 weeks.
The range of movement and grip strength documented in our study is similar to other reported series (Table 5). Furthermore, the rate of secondary procedures in our series was 13%, which is considered low compared to the other published studies (Table 5).
There is a risk of chronic leg pain, laxity of the collateral ligament at the knee, palsy of the peroneal nerve and dysaesthesia of the calf associated with harvesting of the proximal fibula graft. 21 In this series, we encountered two complications related to the operated site and one related to the donor site, amounting to a 20% overall complication rate. For the donor site morbidity, the patient had a loss of sensation over the common peroneal nerve distribution with a big toe drop even after 62 months of follow up. The complication rates reported in the literature vary from 0 to 87.5%.5,16,22-25,31 Therefore, our complication rate is considered low for non-vascularized fibular graft arthroplasty without fusion (Table 5). We have one case of bony recurrence within the transplanted fibula. We postulate that it may be due to transplantation of the tumour cell to the graft during the surgery.
There has been development in using a 3D printed prosthesis to replace native bone. To date, there are only some isolated case reports, and one such case is reported by V Kuptniratsaikul et al. 32 The advantage of such an implant is that it is custom made to fit the size and morphology of the resected segment and avoids donor site morbidity. But I suspect it will have all the complications associated with metal prostheses, such as infection and implant failure. What the future holds for such implants remains to be seen.
From this study, the author recommends using the ipsilateral fibula to advance the periosteal sleeve over the host bone junction and graft bone and to put the graft in a slight ulna plus position to have a more stable fibula carpal joint.
This study has its limitations in terms of the small number of recruited patients, attributed to this condition’s low prevalence rate. As we are using non-vascularized grafts, longer lengths are associated with higher complications, as described by Krieg and Hefti. 33 They reported a 15% complication rate of fatigue fractures and the incidence is higher when a graft 12 cm and longer was used.
Conclusion
Non-vascularized proximal fibula autograft arthroplasty without fusion is a feasible reconstruction option after distal radius resection for patients with giant cell tumours. It has a reasonable union rate and preserves the wrist joint while giving good functional outcomes. Furthermore, fusion is an available option if the arthroplasty fails or when the subject develops symptomatic osteoarthritis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.