
Abstract
Purpose:
The study described a novel surgical treatment of Haraguchi type 1 posterior malleolar fracture in tri-malleolar fracture and patient outcomes at intermediate period follow-up.
Methods:
All patients from January 2015 to December 2017 with tri-malleolar fracture of which posterior malleolar fractures were Haraguchi type 1, were surgically treated in this prospective study. Lateral and medial malleolar fractures were managed by open reduction and internal fixation through dual incision approaches. 36 cases of Haraguchi type 1 posterior malleolar fractures were randomly performed by percutaneous posteroanterior screw fixation with the aid of medial exposure (group 1). And 40 cases were performed by percutaneous anteroposterior screw fixation (group 2). Clinical outcomes, radiographic outcomes and patient-reported outcomes were recorded.
Results:
Seventy-six patients with mean follow-up of 30 months were included. There were no significant differences in the mean operation time (81.0 ± 11.3 vs. 77.2 ± 12.4), ankle function at different periods of follow-up, range of motions and visual analog scale (VAS) at 24 months between the two groups (p > 0.05). However, the rate of severe post-traumatic arthritis (Grade 2 and 3) and the rate of step-off rather than gap in radiological evaluation were lower in group 1 than that in group 2 (p < 0.05).
Conclusion:
Using our surgical technique, more patients had good outcome with a lower rate of severe post-traumatic arthritis, compared with the group of percutaneous anteroposterior screw fixation. Percutaneous posteroanterior screw fixation can be a convenient and reliable alternative in treating Haraguchi type 1 posterior malleolar fracture.
Introduction
Posterior malleolar fractures are relatively common, occurring in 4% of Weber Type A and 46% in each of Weber Type B and C ankle fractures. 1 In spite of a continuously growing number of studies, consensus has not been reached yet as for treatment of posterior malleolar fracture. 2 The size of involved articular surface has been questioned more recently as studies have demonstrated the importance of articular congruence and the stability of the joint. 3,4 As a result, even small displaced posterior malleolar fractures should be well fixed and surgical indications have expanded. 5
The use of computed tomography (CT) scanning has been widespread in the diagnosis of tri-malleolar ankle fractures over the recent decade, which brings a deeper understanding of the fracture patterns and a changed perception of the issues related to them. 6,7 The most frequently used classification of posterior malleolar fractures is Haraguchi classification, dividing the injuries into three types based on their appearance on axial CT. 8 Haraguchi type 1 posterior malleolar fracture is the type with a triangular fragment involving the posterolateral corner of the tibial plafond. On the basis of the classification scheme, 67% of posterior malleolar fractures are classified as type 1, accounting for a majority of the fractures. 8
Generally, Haraguchi type 1 posterior malleolar fracture can be fixed either with percutaneous anteroposterior screws or through a posterolateral approach using screws and/or a buttress plate. 9 –11 Anterior indirect reduction relies upon ligamentotaxis for the reduction 12 but fixation with percutaneous anterior to posterior screws may lack fixation strength. 13 However, direct reduction of the fracture through a posterolateral approach requires more extensive exposure and may require a position change during the operation. Therefore, the optimal surgical technique for Haraguchi type 1 posterior malleolar fracture may be questioned.
The aim of this prospective randomized paper is to compare two approaches for the reduction of the Haraguchi type 1 posterior malleolar fracture.
Materials and methods
Patient demographics
The study was a prospective research of patients who had undergone surgical treatment of tri-malleolar fractures performed at tertiary medical centers in China between January 2015 and December 2017. The study was approved by the medical ethic of authors’ affiliated institutions and all subjects provided informed consent prior to their participation in the study. The inclusion criteria were as follows: Closed tri-malleolar fracture requiring surgery, of which posterior malleolar fracture was a Haraguchi type 1, based on Haraguchi Two-Dimensional Computed Tomography Classification. 8 The exclusion criteria consisted of open fractures, historical operation of the ankle fractures, and the patients who were lost to follow-up. Before the operation, each patient received routine examinations by standard X-ray and CT scan with reconstruction. Finally, 76 patients (49 males and 27 females) completed the study, and were included in the final outcome analysis. Patient allocation to groups was randomized by computer prospectively through the use of sequentially numbered opaque envelopes. Envelopes were opened inside the operating theater by a nurse who was blind to the allocation. Odd number was assigned to group 1 and even number was assigned to group 2. The surgeries were performed by one attending trauma surgeon and two trauma fellows as surgical assistants, who all had significant experience in traumatic surgeries at a single institution. Thirty-six cases of Haraguchi type 1 posterior malleolar fractures performed by percutaneous posteroanterior screw fixation with the aid of medial exposure were in group 1. Forty cases performed by percutaneous anteroposterior screw fixation were in group 2. This sample size met the results of a power analysis. Surgical implants were all provided by single device manufacturer (Wego Group Co., Ltd, Shandong, China). The assessments were conducted by two surgical fellows. When there were disagreements in the assessment, the final scoring of the images was conducted by the attending surgeon. The demographics and injury conditions of the patients in both groups were noted in detail and compared (Table 1).
Demographics and injury conditions of the patients.
* The patients were assigned to the posteroanterior fixation or anteroposterior fixation groups and the groups compared (p < 0.05 was considered significant).
Operative procedures
Percutaneous posteroanterior screw fixation
After subarachnoid block anesthesia, the patient was placed in the supine position with a cushion placed underneath the ipsilateral hip to prevent the usual external rotation of the operative limb. The operative limb had the tourniquet inflated. The maximal duration of tourniquet was 90 min, and tourniquet would be released before the final closure. Lateral malleolar fracture was the first to be exposed, and a longitudinal lateral incision was performed along the projection line of the posterior fibular border. The soft tissue was posteriorly bluntly dissected over the fibula in order to allow reduction and plate fixation. Next, the cushion would be removed to restore the external rotation of the limb. The incision was made along the tibialis posterior tendon to expose the medial malleolus, with the length of incision to 7–8 cm as usual. Accurate reduction would be achieved and fixation with lag screws or/and ductile mini-plate would be performed in medial malleolar fracture. Then, the flexor retinaculum, which is the posterior component of medial malleolus, would be incised longitudinally to expose the tibialis posterior tendon sheath. The tendon was retracted posteriorly with the neurovascular structures. Posterior fragment could be perceived with a fingertip and well managed through medial approach if the fragment was in the state of malreduction. In our experience, the posterior fragment would spontaneously reduce with the aid of gentle dorsiflexion after reduction of medial and lateral malleolus fracture. The reduction was verified by ensuring reduction at the cortical apex of the fracture and fluoroscopically. The reduction was temporarily held by bone forceps. A K-wire would be introduced anteroposteriorly for the posterior fracture. And 1–3 K-wires (based on fracture size) reached the posterior fragment via some small stab incisions protected by sleeve in the anteroposterior direction. Next, K-wires would proceed in the anteroposterior direction while Achilles’s tendon was pushed medially in position of plantar flexion. On these occasion, K-wires would pierce the skin on the lateral side of Achilles’s tendon, avoiding iatrogenic injury of nerves or vessels. Finally, the fragments were stabilized with cortical lag screws via K-wires in the posteroanterior direction. The syndesmosis would be screened to ensure stability. In our experience, fixation of the posterior malleolar fragment is sufficient to stabilize the syndesmosis (Figures 1 and 2)
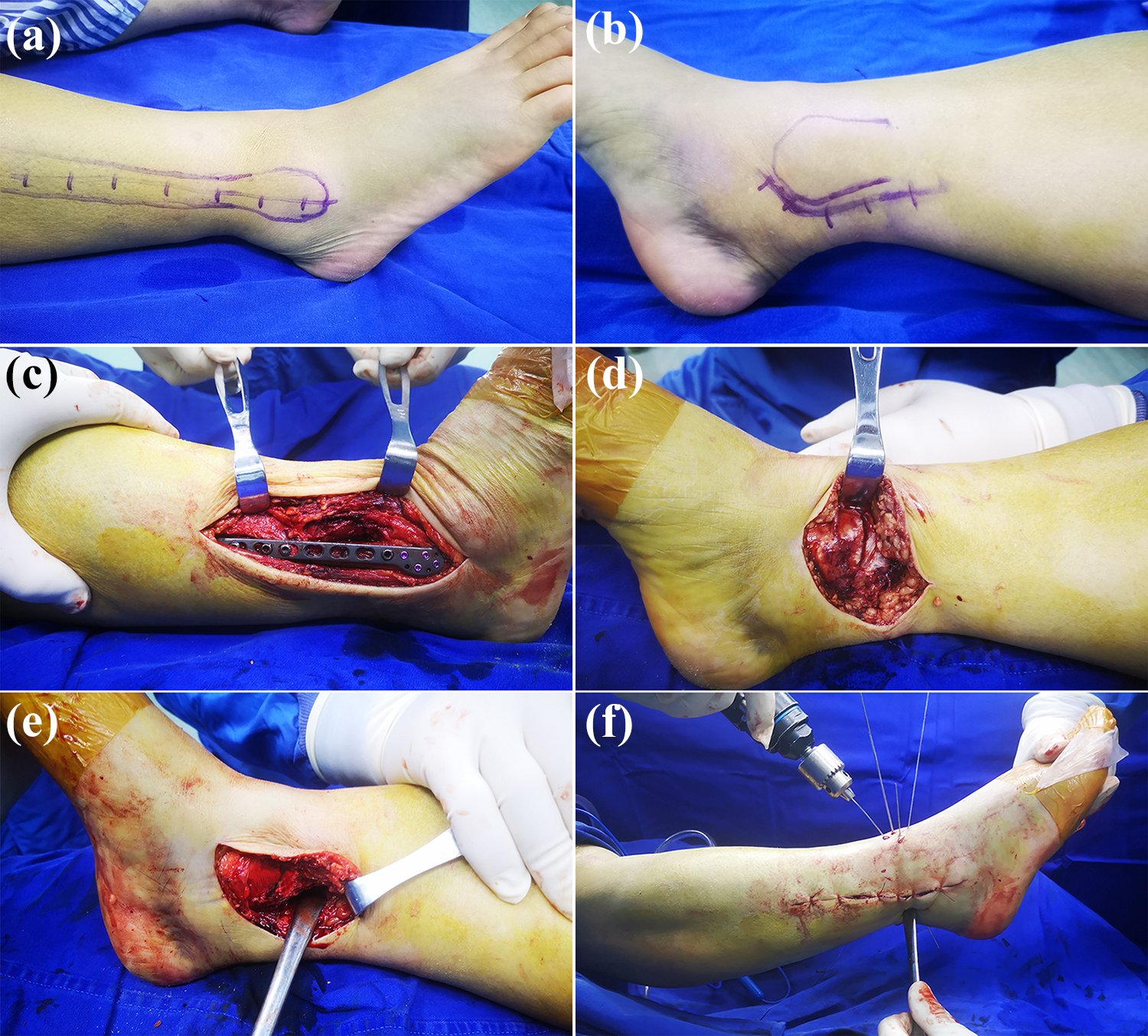
Photographs of operative procedure of tri-malleolar fracture fixation. (a) and (b) Mark of surgical incisions on lateral malleolus and medial malleolus. (c) The lateral malleolar fracture was the first to be fixed. (d) The medial malleolar fracture was exposed and fixed. (e) Posterior fragment could be reached and well managed through medial approach. (f) Serval K-wires (based on fracture size) reached the posterior fragment in the anteroposterior direction and proceed to pierce the skin on the lateral side of Achilles’s tendon.
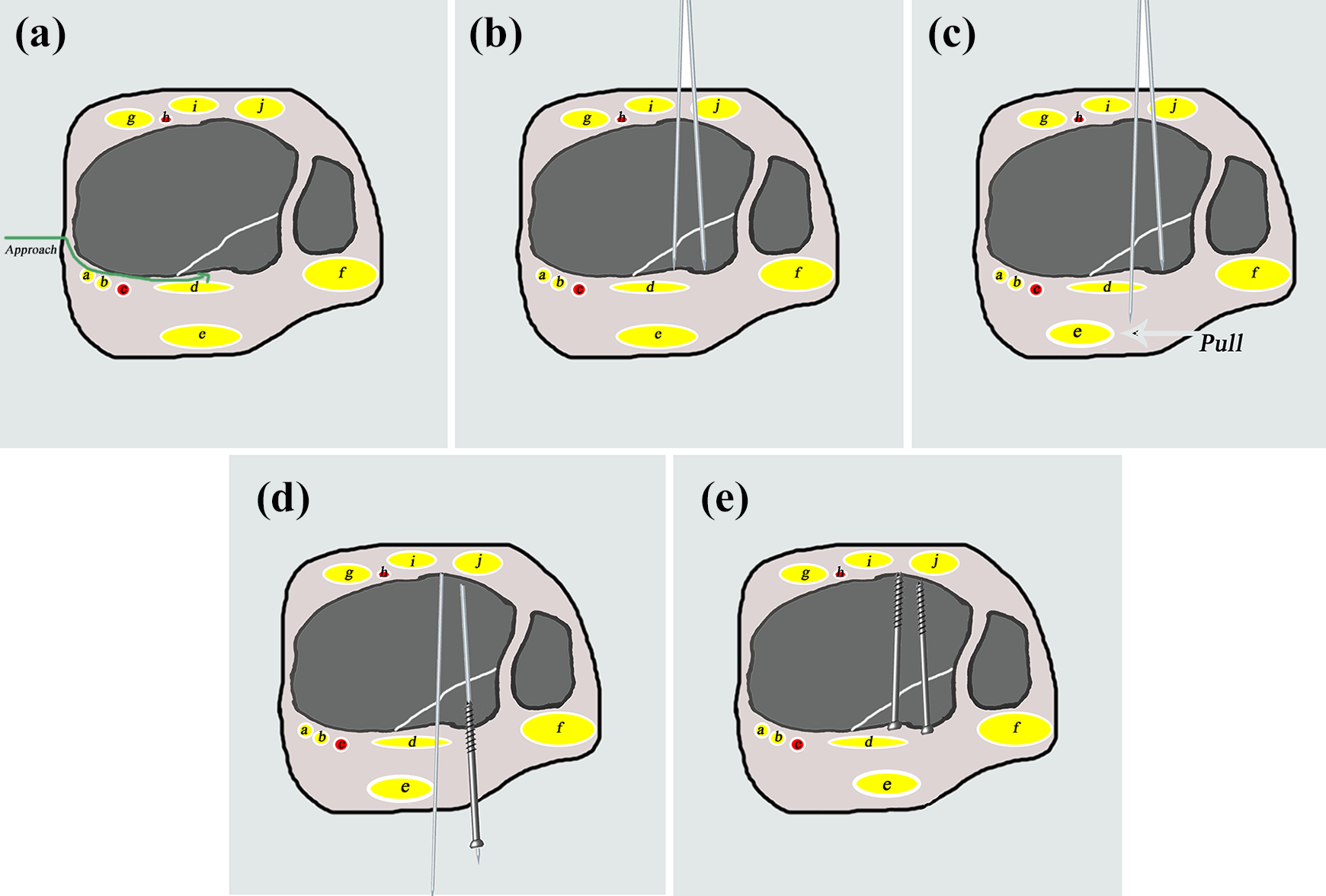
Drawings of operative procedure of percutaneous posteroanterior screw fixation. (a) Posterior fragment can be reached and well managed through medial approach. (b) Serval K-wires (based on fracture size) reach the posterior fragment in the anteroposterior direction. (c) K-wires proceed in the anteroposterior direction while Achilles’s tendon is pushed medially in position of plantar flexion. (d) and (e) Fragment is stabilized with cortical lag screws via K-wires in the posteroanterior direction. (a: tibialis posterior tendon. b: flexor digitorum longus. c: posterior tibial nerve and vessel. d: flexor hallucis longus. e: Achilles tendon. f: peroneal tendon. g: anterior tibial muscle tendon. h: anterior tibial nerve and vessel. i: extensor hallucis longus. j: extensor digitorum longus.)
Percutaneous anteroposterior screw fixation
Operation preparation and management of lateral and medial malleolar fractures were similar to that for the percutaneous posteroanterior screw fixation. The posterior malleolar fracture was only reduced by ligamentotaxis. After indirect reduction, 1–3 K-wires (based on fracture size) reached the posterior fragment in the anteroposterior direction. Length of lag screw would be measured and the fragments would be stabilized with cortical lag screws via K-wires in the anteroposterior direction.
Intraoperative and postoperative data
During the operation, operative time was recorded. Furthermore, the key steps of surgical approaches were clearly photographed.
At the postoperative follow-up, all patients were assessed with X-rays and CT scan within 24 h. (Figure 3) The reduction quality of the tri-malleolar fracture was evaluated by two surgical fellows. Reduction of posterior malleolus was evaluated by CT sagittal scan as good in case of a gap/step-off in the articular surface ≤2 mm, and as poor with gap >2 mm (Figure 4). Patients would be splinted for 2 weeks until the wound healed. Exercises then started under the supervision of a physiotherapist, with progressive weight bearing in a removable splint. Patients were discharged from hospital when their vital signs were stable and there was no exudation from the incision. Mobilization of the ankle and permission to weight-bear were determined on a case-by-case basis following an assessment of VAS pain score, local edema, image examination, and the stability obtained at the time of fixation.

Images of tri-malleolar fracture before and after operation. (a) to (e) Preoperative radiograph and computerized tomography showing a case of tri-malleolar fracture, of which posterior malleolar fracture was a Haraguchi type 1. (f) to (i) Postoperative radiograph and computerized tomography showing the posterior malleolar fracture was fixed by percutaneous posteroanterior screws.

Radiological evaluation of posterior malleolus reduction by CT sagittal scan. (a) Posterior malleolar fracture is evaluated as good with gap and step-off in the articular surface ≤2 mm. (b) and (c) Posterior malleolar fracture is evaluated as poor with step-off or gap ?2 mm.
All fractures were reviewed with postoperative X-rays by an orthopedic surgeon during each clinic visit. In addition, the ankle function was evaluated using the Olerud–Molander Ankle Score. 14 Range of motion of ankle plantar flexion and dorsiflexion was measured with a goniometer at 2 years after surgery. Arthritic changes were classified according to the Kellgren and Lawrence scale: 15 Grade 0-normal, no changes; Grade 1-mild, small marginal osteophytes without narrowing of the joint space; Grade 2-moderate, small marginal osteophytes with definite narrowing of the joint space, with or without subchondral sclerosis; Grade 3-severe, multiple large osteophytes, complete loss of joint space, subchondral bone sclerosis, loss of joint contour.
Statistics
The sample size calculation was based on the rates of step-off or gap between two groups. As 50 cases (25 cases in group 1 and 25 cases in group 2) were enrolled in the study, 8 cases of step-off or gap of the posterior malleolar fracture in radiological evaluation were observed in group 1 and 17 cases occurred in group 2. The rate of step-off or gap occurring in group 1 (R1) was 32% while the rate in group 2 (R2) was 68%. As two-sided test requested, α = 0.05, β = 0.2. We put the variables into computational formula:
Descriptive statistics were recorded and collated. The mean and standard deviation for the patient demographics and intraoperative outcomes were calculated from the original dataset. An unpaired t-test was used to compare the patient demographics and intraoperative outcomes between the two groups. The chi-squared test was used to measure the association between the categorical data of the two groups. Results were considered significant when p < 0.05. All statistical analyses were performed using SPSS 22.0 (SPSS Inc., IL, USA).
Results
During the study period, 76 patients completed the protocol in group 1 or group 2. There were no significant differences in the age, sex, and distributions of fracture etiology between the two groups (p > 0.05).
The mean patient follow-up was 30 months (range, 24–42 months). The period of injury to surgery was 6.7 ± 2.2 days in group 1 and 6.5 ± 2.4 days in group 2, with no significant difference between the two groups (p > 0.05). During surgery, the operation time of each patient was meticulously recorded. The operation time (81.0 ± 11.3 min vs. 77.2 ± 12.4 min) was not significantly different between the two groups (p > 0.05).
After surgery, radiological evaluation was the primary focus of this study. All patients were assessed with X-rays and CT scan within 24 h. Step-off and gap of the posterior malleolar fractures were evaluated. Five cases of step-off occurred in group 1 (12.8%) and 15 cases were noticed in group 2 (37.5%). Significant differences were observed in step-off of the posterior malleolar fractures. However, there was no significant difference in gap between group 1 (6 cases, 16.7%) and group 2 (10 cases, 25%). Furthermore, no significant differences were observed in ankle function (Olerud–Molander scale) at each follow-up period (p > 0.05). And range of motions of dorsiflexion and plantar flexion and VAS were both equal between two groups at 24 months after surgery (p > 0.05). Arthritic changes were classified according to the Kellgren and Lawrence scale at each patient’s last follow-up. There were significant differences in the number of severe posttraumatic arthritis (grade 2 & grade 3) between group 1 and group 2 (p < 0.05) (Table 2).
Intraoperative and postoperative data of patients.

* Mean operating time, period of injury to surgery, radiological evaluation, visual analog scale, ankle function, and grading posttraumatic arthritis were recorded and compared (p < 0.05 was considered significant).
Discussion
The distal tibia ends in a concave articular surface and serves to transmit axial compression force. The posterior malleolus plays an important role in stability and load distribution through the ankle. 2 In clinical practice, the author observed that worse prognosis and more severe posttraumatic arthritis would progress when displaced posterior malleolar fractures were part of the ankle fracture complex. Although the posterior malleolar fracture has no definitive management guidelines regarding optimal treatment, surgical indications may expand to fix even small displaced posterior malleolar fractures.
There are several classifications of posterior malleolar fractures based on radiological evaluation. Haraguchi two-dimensional computed tomography classification is the first CT-based classification, based on the analysis of axial CT scans of 57 patients. 8 The classification divides the injuries into three types and type 1 is the type with a triangular fragment involving the posterolateral corner of the tibial plafond. The posterior malleolar fracture is most likely produced by ligamentous and capsular avulsions in rotational injuries. Hence, the fixation of posterior malleolar fracture contributes to reduction of the articular surface and stability of the tibiofibular syndesmosis.
Internal fixation of posterior malleolar fracture can be performed by direct or indirect technique. The choice of approaches depends on the type of the fracture and the overall malleolar fracture pattern. In Haraguchi type 1 fracture, the posterolateral approach allows simultaneous direct reduction of the posterior malleolar fragments and the distal fibular fracture. 12,16 It is especially practiced with comminuted posterior fractures of Haraguchi type 3. 8 Several screws or a small buttress plate may be applied based on the size of the fracture. However, the posterolateral approach needs position changes during operation of tri-malleolar fracture, which may increase the risk of infection and do harm to patients with spinal injuries or multiple fractures. Indirect reduction and anteroposterior fixation is another technique widely used in ankle fracture surgery. It is most suitable for single, large triangular fragments, such as Haraguchi type 1 fracture. Similarly, the technique has its disadvantages. 10,17 Step-off or gap may exist because of indirect reduction. Furthermore, anteroposterior screws may not provide enough compression while the threads of lag screws partially cross the fracture line, especially in interfragmentary cases. 18
No published study has ever reported technique of percutaneous posteroanterior screw fixation in treating Haraguchi type 1 fracture. The study showed that percutaneous posteroanterior screw fixation could be safely used to address the management of Haraguchi type 1 posterior malleolar fracture without extensive exposure. No nerve or vascular injuries were observed in the study. Furthermore, better reduction was achieved in posteroanterior screw fixation with the aid of medial exposure than that in anteroposterior fixation. Based on postoperative CT scan, there were less cases showing step-off or gap of posterior malleolar fractures in group 1 and significant difference was observed in step-off between two groups. During operation, posterior fragment could be perceived with a fingertip and got reduction with leverage through medial approach and dorsiflexion if the fragment was in the state of malreduction. Meanwhile, K-wires could be verified reaching the posterior fragment. As a result, the technique was comparable with direct reduction.
There was significant difference in the number of severe posttraumatic arthritis (grade 2 and grade 3) between group 1 and group 2 at patients’ last follow-up. Without exception, cases of severe posttraumatic arthritis accompany the malreduced posterior malleolar fractures. However, there were no significant differences in VAS, Olerud–Molander Ankle Score, and range of motion of dorsiflexion and plantar flexion between the two groups. The study may require longer follow-up to confirm radiological evaluation and ankle function.
Limitations
There were several limitations to our study. The study only compared percutaneous posteroanterior screw fixation and anteroposterior screw fixation without direction reduction of posteromedial or posterolateral approaches for posterior malleolus fixation. Further research in comparing posteroanterior screw with posterlateral buttress plating should be undertaken. Furthermore, the period from surgery to the final follow-up was not equal in every case, which may affect the results of radiological evaluation. More patients should be enrolled and a long-term follow-up as required in order to establish the safety and efficacy of percutaneous posteroanterior screw fixation.
Conclusion
The study has described a new technique in treating patients with Haraguchi type 1 posterior malleolar fractures in tri-malleolar fractures. Using our surgical technique, more patients with a posterior to anterior screw placement had good outcome with a lower rate of severe post-traumatic arthritis, compared with the group of percutaneous anteroposterior screw fixation. Though, posterolateral approach with direct vision of the fracture fragment is the standard worldwide approach to the Haraguchi type 1 posterior malleolar fracture, percutaneous posteroanterior screw fixation may be a convenient and reliable alternative technique.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.