
Abstract
Purpose:
To evaluate the characteristics of abused children, families and abusive event and to identify risk factors associated with recurrence of child abuse.
Methods:
Retrospective data from 133 children aged between 2 months to 15 years old who were diagnosed as abuse between year 2002 and 2017. Thirteen items related to characteristics of the child, families, abusive event were selected. These factors were analyzed by multivariate logistic regression model for association with repeated child abuse.
Results:
Total of 133 subjects with average age of 5.25 ± 4.65 years old. There were 54 cases (40.60%) reported of repeated abuse. Majority of repeated abuse type in this study was physical abuse (73.68%). Most perpetrators were child’s own parents (45.10%). Factors associated with increased risk of repeated abuse were child age 1–5 years old (AOR = 4.95/95%CI = 1.06–23.05), 6–10 years old (AOR = 6.80/95%CI = 1.22–37.91) and perpetrator was child’s own parent (AOR = 21.34/95%CI = 3.51–129.72). Three cases of mortality were found with single-visit children and one case in recurrence. Most of death cases were children less than 1-year-old with average age of 7 months. Causes of death were subdural hematoma with skull and ribs fracture.
Conclusions:
Identifying risk factors for repeated child abuse help in recognizing child at risk to provide prompt intervention. This study found two factors associated with higher risk of abuse recurrence: child age 1–10 years old and abusive parents. Children who presented with these risk factors should be recognized and intensively monitored.
Introduction
Child abuse is an important problem with lifelong health sequelae. Many victims are abused by their parents and relatives, and they might have been mistreated by more than one abusive adult. Some victims also experience repeated abuse throughout childhood. Therefore, prevention is a priority in both developing and developed countries. 1
A literature review demonstrated that child and family characteristics have a significant effect on the risk of child abuse. Factors associated with child abuse are a child’s sex, premature birth, the number of siblings, and family poverty. 2 The relationships between poverty, level of schooling, and child abuse are recurring variables in many studies. 3
The recurrence rates for physical and neglect abuse reported in the literature range from 9% to 67%, depending on the age of the child; length of follow-up; type of initial or subsequent abuse; services provided; and whether the studies investigated reports, hospitalizations, or actual maltreatment. 4,5
Identifying children at risk of repeated abuse during their first hospital visit could aid healthcare professionals in providing intensive monitoring and may prevent further abuse. However, there are limited studies on the risk factors for abuse recurrence, indicating the need to explore and understand this important topic in order to facilitate its optimal treatment. The objectives of this study were to evaluate the characteristics of children, families, and abusive events, and to identify the risk factors associated with the recurrence of child abuse.
Methods
Subjects
The subjects included children aged 2 months to 15 years who were recorded as having been abused in our hospital’s medical records for the period 2002–2017. A total of 133 cases were reviewed.
Definition of physical abuse was any physical injury, mental injury, or threatened injury, inflicted by a person responsible for the child’s care on a child other than by accidental means. Sexual abuse was unwanted sexual intercourse through threats, physical harm, or exploitation with a child yet over 15 years of age whether a child shall consent or not. Neglect abuse was failure to provide for a child’s basic needs within their own environment.
When children were suspected with child abuse, they would be admitted to the hospital and separated from their parents/caregiver. After that we consulted with multidisciplinary team which comprised of pediatrician, psychiatrists, orthopedists, and social workers.
Data collection
After the study protocol was approved by the hospital institutional review board (approval number SI151/2016), we retrospectively reviewed the medical records of children who had been diagnosed as having been subjected to either physical, sexual, or neglect abuse. Data relating to the characteristics of the children, their families, and the abusive events were collected.
We divided the subjects into groups, based on any evidence of repeated abuse. Factors that were suspected to be related to repeated abuse were evaluated. These comprised children’s age; sex; disability; preterm birth; type of abuse (physical, sexual, and neglect); perpetrators (parent, stepparent, caregiver, and others); parent’s age and level of education; parental status (married and separated/divorced); number of siblings; and household income.
Data analysis
The data were analyzed using IBM SPSS Statistics for Windows, version 19 (IBM Corp., Armonk, NY, USA). Descriptive statistics (consisting of frequencies, percentages, means, ranges, SD, and correlation) were used. We assessed the associations between the risk factors and repeated abuse in a single logistic regression analysis, and reported the crude odds ratios and p-values. Variables with p-values <0.2 were entered into a multiple regression model. Statistical significance was defined as p < 0.05.
Results
The total of 133 subjects (male 62; female 71) had an average age of 5.25 years. The average ages of the fathers and mothers were 34.4 and 29.3 years, respectively. Most parents’ education level was primary and secondary. Demographic information about the characteristics of the children are shown in Table 1. There were 54 cases (40.60%) of recurrent abuse, with the large majority of those classified as physical abuse (73.68%). Most perpetrators of the repeated cases were the children’s own parents (45.10%). As shown in Table 2, those cases involving physical abuse showed a statistically significant association with an increased risk of repeated abuse (odds ratio [OR], 9.34; 95% confidence interval [CI], 1.16–75.18). Also, repeated abuse was more likely to recur if one or more of the following factors were present: a child age of 1–5 years (OR, 5.00; 95% CI, 1.63–15.34); a child age of 6–10 years (OR, 5.31; 95% CI, 1.64–17.26); the perpetrator being a parent (OR, 7.50; 95% CI, 2.14–26.24); the perpetrator being a stepparent (OR, 8.00; 95% CI, 1.58–40.63); and if the parent was separated or divorced (OR, 2.00; 95% CI, 0.93–4.31).
Characteristic of children and family.

Risk factors in univariate and multivariate logistic regression model for repeated abuse.
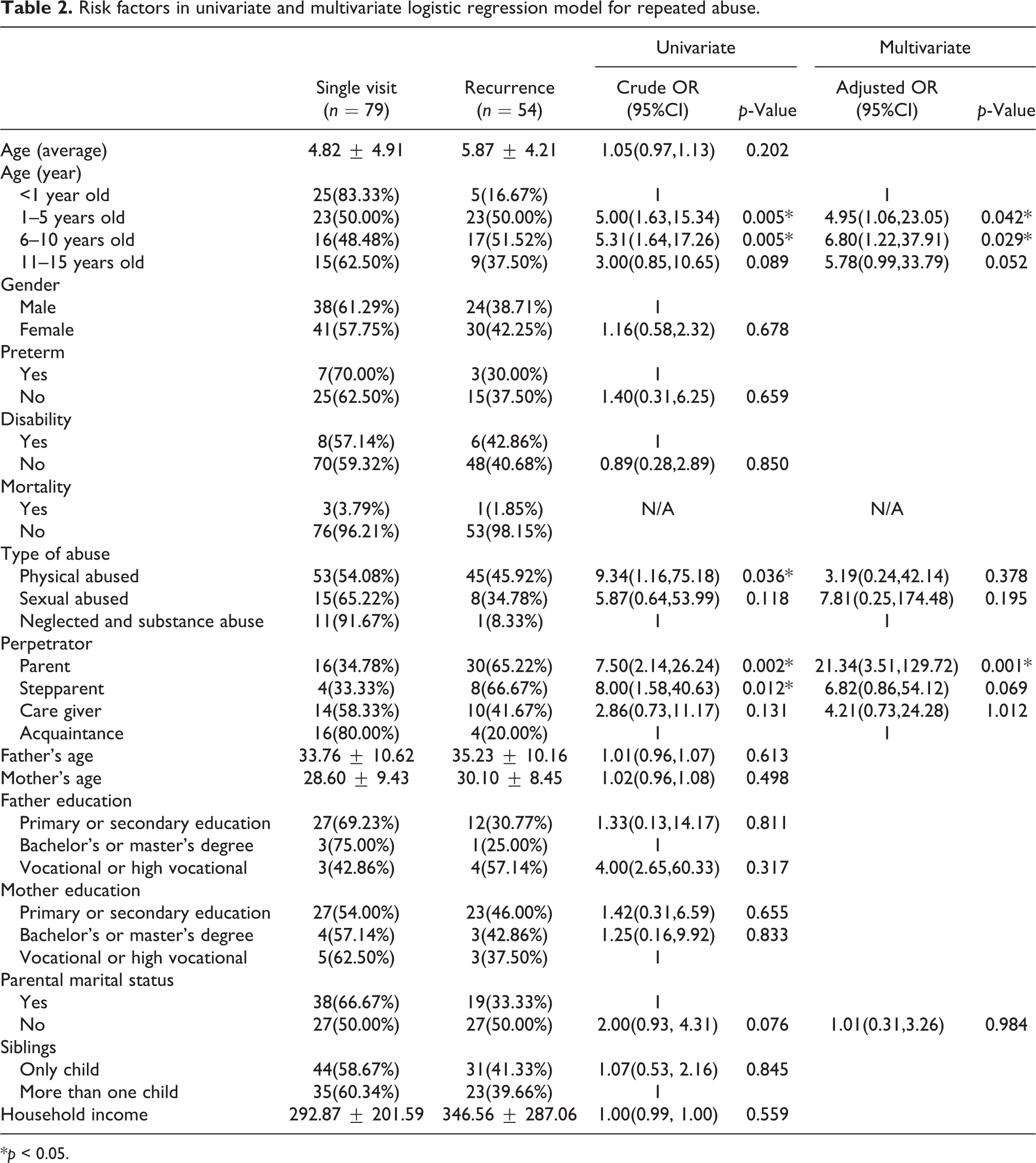
*p < 0.05.
Children’s sex, preterm birth, disability, number of siblings, parent’s age, and parent’s level of education demonstrated no statistical significance as risk factors for repeated abuse
Table 2 also presents the results of a multiple logistic regression analysis. It revealed that three risk factors were significantly associated with repeated abuse: a child age of 1–5 years (adjusted odds ratio [AOR], 4.95; 95% CI, 1.06–23.05); a child age of 6–10 years (AOR, 6.80; 95% CI, 1.22–37.91); and the perpetrator being the child’s parent (AOR, 21.34; 95% CI, 3.51–129.72).
As to the physical abuse cases, bruises, and burns constituted about 68.37% of the total physical abuse case, non-bony head injury (subdural hematoma) represented 16.33%, and fractures accounted for 14.29%. The most frequent location of the fractures was the femur (40%), followed by the forearm (13.3%) and humerus (13.3%). The majority of long bone fractures were in the diaphysis (66.7%).
The average ages of the subdural hematoma and fracture cases were 8 months and 2.8 years old, respectively. Three cases of deaths (3.79%) were found with single-visit children while one case (1.85%) was found in repeated cases. All of death cases were resulting from subdural hematoma with two out of four cases also had skull and ribs fracture. One case of death had history of previous physical abused with skull and ribs fracture. The overall average age at death being 7 months with the youngest case at 13 days old.
Discussion
This study identified a range of child, family, and other characteristics associated with risk for repeated abuse. Identifying the risk factors for repeated child abuse will assist healthcare providers to recognize children at risk. We found that the child’s age and the person committing the abuse were significantly associated with a higher risk of repeated abuse.
In our hospital when children were suspected with child abuse, they would be admitted to the hospital and consulted with multidisciplinary team. However, there were cases that we missed and resulting in recurrence abuse. Therefore, identifying these risk factors may help to enhance our management and surveillance for repeated case in the future.
Child factors
Age
The average age of the abused children in this study was 5.25 years. This was noticeably higher than the findings of another study. It found that the highest rate of abuse occurred from birth to 1 year of age, and that children <3 years had the highest risk of becoming victims of abuse or neglect. 2 In the current study, the child’s age was a significant risk factor: although infants (<1 year of age) had less repeated abuse, children aged 1–10 showed significantly higher risks of recurrence. This finding was consistent with previous studies. 6 –10 Moreover, some published studies have suggested that a low child age is a risk factor for recurrence. 11 In contrast, one Japanese study identified that a higher child age (9–13 years) was a significant predictor of recurrence. 12 Nevertheless, other studies have suggested that age is not a significant predictor. 13 –15 These variations in the findings and conclusions may be due to the studied populations being heterogeneous, comprising samples from both general and specific high-risk populations. Also, other studies have stated that there are more complicated mechanisms beneath the effect of child age on recurrence. 16,17
Sex
This study found that a child’s sex was not a significant risk factor for repeated abuse, which concurs with previous literature. 6 –8,10,14,17 However, the findings from some studies suggested that there is a greater recurrence rate for females than males. 9
Disability
It has been previously reported that children with disabilities are more vulnerable to abuse or neglect, and that they have an increased risk for child abuse recurrence. 9,18 –20 Despite that, the current study did not find a significant association between disability and the risk for repeated abuse. Although Connell et al. 8 found similar results to our study, their investigation was focused on a different population.
Preterm birth
Children who have a history of preterm birth may be more vulnerable to abuse. Other studies have found that premature birth was found to have a significant effect on the risk of child abuse. 2,21,22 Nevertheless, to our knowledge, no study has yet established an association between preterm birth and the risk for repeated abuse. The results of our study indicated that preterm birth is not a significant risk factor.
Abuse events
Types of abuse
It has been reported that the most frequent type of abuse was neglect, and the second was physical abuse. Previous studies 6,10,17 demonstrated that neglect abuse was associated with the highest risk of recurrence whereas physical abuse had the second highest significant association. The findings of those studies were also consistent with others which reported that neglected children are more likely to experience abuse recurrence. 18,20 In contrast, the majority of the abuse types found by the current study were physical abuse (73.7%), which was also the most common in repeated cases. This difference in findings can be explained by the population in our study being children who were brought to the emergency department with or without admission to the hospital. Unlike physical or sexual abuse, most neglected children may not be brought to the hospital; therefore, the frequency of neglect cases found by the current study could be underestimated. Ben-Natan et al. 21 identified that physical abuse was found more often in children aged 10 years or older. Although their finding contradicts literature reports that physical abuse is more common in younger children, 22 it is similar to the finding of our study.
The most common reason for children suffering with physical abuse to be taken to hospital was reported by one study to be bruises and burns (87.1%), 21 which corresponded with the findings of earlier research. 23 Our study demonstrated a similar result.
In this study, fractures accounted for 14.29% of all physical abuse cases, with the most common location of the fractures being the femur. This is consistent with previous studies which showed that fractures were the second most common presentation of physical abuse, after soft-tissue bruises and burns. 24 The incidence of fractures in child abuse cases ranges from 9% to 55%, depending on the type of abuse and the method of detecting fractures. 25 Approximately one third of the physically abused children required orthopedic treatment. 26
A previous study revealed that the incidence of death was 4% in individuals who had been evaluated previously and 3% in those with single visits. 27 This was concordant with our results that 3.79% were found with single-visit children and 1.85% in repeated cases. Most of death cases in our study were occurred in children less than 1 year of age (the youngest case was 13 days old). All cases were resulting from subdural hematoma that may be a result from shaken baby syndrome or fell from height which led to severe brain damage in young children. One case of death had history of previous physical abused with skull and ribs fracture, unfortunately, second abused caused death. Previous study from Deans et al. 28 showed that the mortality was significantly higher in children who experience nonaccidental trauma in children. The longer and more repetitive abuse can lead to more aggressive and brutal injures that can cause a life of a child. Therefore, we should be able to recognize children at risk from the initial episode and keep them under surveillance before it was too late.
Perpetrators
We found that most perpetrators were the children’s own parents (45.1%), which concurs with Ben-Natan et al. 21 Moreover, if the parents were the perpetrators, the abuse was associated with a higher risk of recurrence. Abuse by stepparents had a significantly higher rate of repeated abuse, despite the overall number of incidents involving stepparents being lower than that by the children’s biological parents. To our knowledge, there has not been a previous study into the association between the perpetrators and the risk of repeated abuse.
Parent factors
Parent’s age
The average ages of the fathers and mothers were 34.39 and 29.29 years, respectively. Wu et al. 2 found that a young age of the mother at pregnancy had a significant effect on the risk of child abuse. On the other hand, other studies 11,13 demonstrated that the age of the parent was not a significant risk factor for repeated abuse, which corresponded with our result.
Level of education
The educational attainments of the parents in the present study were mainly the primary and secondary levels. Earlier studies showed that parental level of education was not a significant indicator of repeated abuse, 11,14 which was also the case with our study. However, another study suggested that parents who were high school graduates were less associated with the risk of recurrence abuse. 17 It may be that more educated caregivers are better able to take care of their children and access the support services they need than less educated caregivers.
Parental marital status
Some published studies have suggested that parental marital status is not a significant predictor for recurrence, 11 which agrees with our result. By contrast, one study demonstrated that single parenthood increased the risk of repeated abuse, and stepparenthood predicted the likelihood of multiple recurrences of abuse. 6
Family factors
Number of siblings
Wu et al. 2 found having more than two siblings had a significant effect on the risk of child abuse. Other studies have suggested that having an increased number of children in the family presents a higher risk of recurrence. 6,10,17 This may be due to an increased burden being placed on caregivers as a result of having younger and/or more children, leading to higher levels of recurring or continuing abuse. Nevertheless, the number of siblings in the family did not reveal a significant effect on repeated abuse in the current study.
Household income
The average monthly household income in this study was 310.13 USD, which was much less than the average monthly household income in Thailand (843.70 USD). 29 Wu et al. 2 showed that poverty in the family had a significant effect on the risk of child abuse, and other published studies have suggested that family poverty is associated with a higher risk of repeated abuse. 7,11 Also, a Japanese study identified that financial instability was a significant predictor of abuse recurrence. 15
Limitations
There were some limitations to this study. Firstly, as it was predominantly based on medical records, patient information was partly missing in some cases. Other limiting factors were its small sample size in a tertiary-care setting, an unbalanced socioeconomic status, and the relatively small number of subjects identified as suffering with neglect or emotional abuse, all of which reduced the power of the study and limited its generalizability. Additionally, it is possible that reabuse occurred but was not reported to our multidisciplinary team; in other words, the number of reabused children in this study may well have been under-represented.
Conclusions
The risk factors for repeated child abuse should be evaluated to help recognize children at risk and keep them under surveillance. This study found two factors associated with a higher risk of abuse recurrence: a child age of 1–10 years, and the perpetrator being the child’s biological parents. Children who present with these risk factors should be recognized and sent for intensive child observation in order to prevent further abuse.
Footnotes
Acknowledgement
The authors of this study gratefully acknowledge Suchitphon Chanchoo for assistance with data collection and statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.