
Abstract
Introduction
The coracoid process is an important anatomical structure of the scapula, which can be used as a landmark in the diagnosis and treatment of scapula related diseases, such as acromioclavicular joint dislocation, anterior shoulder instability, and coracoid fractures. The aim of this study was to classify the coracoid process according to morphology and to measure the morphological parameters of the coracoid process.
Materials and methods
A total of 377 dry and intact scapulae were collected and classified in terms of the connection between the shape of coracoid process and common things in life. The anatomical morphology and the position related to acromion and glenoid socket of the coracoid process were measured in each type by three independent researchers with a digital caliper. The measurements were averaged and recorded.
Results
Based on obvious morphological features, five specific types of the coracoid process were described: Type I, Vertical 8-shape; Type II, Long stick shape; Type III, Short stick shape; Type IV, Water drop shape, and Type V, Wedge shape. Type I (30%) and Type III (29%) were more prevalent in China. The tip width of the coracoid process of Type IV was the shortest and significantly different compared to the other types (p <.05), contrary to the longest in Type V. The tip thickness of the coracoid process of Type I was the shortest and significantly different from the other types (p <.05).
Conclusions
The coracoid process was classified into five types based on obvious morphological features. Knowing of morphological classification and anatomical parameters of different types of the coracoid process, to some extent, may be helpful to diagnose and treat the shoulder joint disease, such as acromioclavicular joint dislocation, anterior shoulder instability, and coracoid fractures, and to theoretically reduce postoperative complications.
Keywords
Introduction
The coracoid process is not only an important anatomical structure on the scapula, but also an anatomical landmark for shoulder surgeries, playing a crucial role in the diagnosis and treatment of scapula related diseases, such as acromioclavicular joint dislocation, anterior shoulder instability, and coracoid fractures.1–4 Although the studies about the treatments of acromioclavicular joint dislocation, anterior shoulder instability, and coracoid fractures have been well-rounded, there are still some limitations because lacking of detailed measurements of the coracoid process. For example, lacking of the anatomical information about the insertion of CC (Coracoclavicular) ligaments in the coracoid process may increase the risk of cortical breach, and fractures of the coracoid process and the clavicle during CC ligament reconstruction for acromioclavicular joint dislocation.5–8 Besides, in the Latarjet procedure, before the osteotomy is performed during surgery, appropriate graft length from the tip of the coracoid process have not reached an agreement, which may lead to some complications including graft malposition, malunion nonunion and intraoperative graft fractures.1,9,10 These complications are attributed to lacking of a mastery of the coracoid morphology. Moreover, treating coracoid fractures without mastery of anatomical structure of the coracoid process may result in a secondary fractures and loss of fixation. 11
Some findings have underlined the importance of the coracoid process in diagnose and therapy of shoulder joint disease. 12 In general, conservative managements are adopted for type I to III of coracoid fractures, and surgical managements are adopted for type IV to V of coracoid fractures. 3 Eyres has divided the fractures of the coracoid process into five types based on morphometries, 13 which conducts the treatments of coracoid fractures. Moreover, it has been confirmed that its height and width ratio may have an influence on the occurrence of the shoulder impingement syndrome, one of the most common shoulder diseases. 14 However, these studies are still not precise enough for the measurement of coracoid process, and the guiding role for treatment of shoulder joint disease is relatively limited.
Therefore, the purposes of this study were to (1) to measure the morphological parameters of different coracoid types and (2) create a novel classification of the coracoid process according to their morphology.
Materials and methods
Ethics statement
All procedures of this study were approved by the Ethical Committee of Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University (No. SWMCTCM2017-0801), and performed based on the 1964 Helsinki declaration as well as its later amendments or comparable ethical standards.
Samples
A total of 377 dry and intact Chinese scapula were collected from the department of anatomy, Southern Medical University, 175 left and 202 right (the age and sex were unknown). Inclusion criteria: Adult specimens and scapula are intact; exclusion criteria: scapula fracture, coracoid process, acromion, or glenoid socket defect.
Sample measurements
Two investigators contemporaneously classified the coracoid process on account of morphological characteristics. A third investigator was delegated for a final determination, when any controversy arose during the observations. And two of them measured spatial position, anatomical morphology and angles of the coracoid process with a digital caliper (Mitutoyo America Corp, Aurora, IL) and goniometer, respectively. The Spearman’s rank correlation coefficient was added to test the inter-rater and intra-rater reliability.
The value of the report was the average of two investigators. All parameters were measured to third decimal place, and the result was kept to two decimal place. Figure 1 described the location of the bony landmarks. Angular and linear parameters of the coracoid process were quantified, angular parameters including ∠α, ∠β, ∠γ, linear parameters including the width, thickness, length, and distance. As illustrated in Figure 1, the following parameters of the coracoid process were measured: ∠α: the angle between tip axis and base axis of the coracoid process, ∠β: the angle between the connection from supraglenoid tubercle to infraglenoid tubercle and base axis of the coracoid process, ∠γ: the angle between tip axis of the coracoid process and vertical axis of the scapula glenoid, ab: the tip width of the coracoid process, op: the width of the front of the coracoid precipice, cd: the precipice width of the coracoid process (specific location at which changes of the surface of the coracoid process from the horizontal to the vertical direction), eq: the tip length of the coracoid process, sj: the precipice length of the coracoid process, mk: the base length of the coracoid process, eh: the length from tip to precipice of the coracoid process, iq: the tip thickness of the coracoid process, is: the precipice thickness of the coracoid process, lr: the base thickness of the coracoid process, en: the thickness from tip to base of the coracoid process, gl: the thickness from precipice to base of the coracoid process, et: the distance from tip of the coracoid process to acromion, eu: the distance from tip of the coracoid process to supraglenoid tubercles, ev: the distance from tip of the coracoid process to suprascapular notch, ew: the distance from tip of the coracoid process to upper corner of scapula. Linear and angular measurements. (a) ∠α: the angle between tip axis of coracoid process and base axis of coracoid process. (b) ∠β: the angle between the connection from supraglenoid tubercle to infraglenoid tubercle and base axis of coracoid process. (c) ab: the tip width of coracoid process; op: the precipice width of coracoid process; cd: the precipice width of coracoid process (specific location at which changes of the surface of coracoid process from the horizontal to the vertical direction). (d) eq: the tip length of coracoid process; sj: the precipice length of coracoid process; mk: the base length of coracoid process; eh: the length from tip to precipice of coracoid process; iq: the tip thickness of coracoid process; is: the precipice thickness of coracoid process; lr: the base thickness of the coracoid process; en: the thickness from tip to base of coracoid process; gl: the thickness from precipice to base of coracoid process. (e) ∠γ: the angle between tip axis of the coracoid process and vertical axis of scapula glenoid; et: the distance from the tip of the coracoid process to acromion; eu: the distance from tip of the coracoid process to supraglenoid tubercles; ev: the distance from tip of the coracoid process to suprascapular notch; ew: the distance from tip of the coracoid process to upper corner of scapula.
Statistical analyses
Statistical analysis was performed by using SPSS 20.0 software (Chicago, IL, USA). Since the coracoid process was divided into five types, the expected occurrence rate of each type is 20%. Assuming the allowable error was 0.05, the expected sample size was 246 specimens by the calculation formula of population rate. On this basis, 377 specimens were collected to expand the sample size. Categorical variables were expressed by frequencies and percentages which were tested by Chi-square. And all parameters of linear and angular measurements were presented by mean and SD (
Results
Classification of the coracoid process
Based on morphological classifications, five specific types of the coracoid process were described: Type I, Vertical 8-shape (“8” shaped, blunt at top and bottom); Type II, Long stick shape (the length is three times longer than the width, blunt at top and bottom, and the sunken in the middle not obvious); Type III, Short stick shape (the length is less three times longer than the width, blunt at top and bottom, and the sunken in the middle not obvious); Type IV, water drop shape (sharp at the top, blunt at the bottom and no sunken in the middle); and Type V, Wedge shape (blunt at the top, sharp at the bottom and no sunken in the middle). Figure 2 and Figure 3 showed the different types of the coracoid process. Type I-Vertical 8-shape (30%) and Type III- Short stick shape (29%) were more frequent in China, followed Type II- Long stick shape (17%) and Type V-Wedge shape (13%). Type IV-Water drop shape (11%) was the least frequent. Hand-drawn diagram of classification of coracoid process. (a) Type I, Vertical 8-shape (“8” shaped). (b) Type II, Long stick shape (the length is three times longer than the width). (c) Type III, Short stick shape (the length is less three times longer than the width). (d) Type IV, Water drop shape (narrow at the top and wide at the bottom). (e) Type V, Wedge shape (wide at the top and narrow at the bottom). Cadaveric classification of coracoid process. A total of 377 scapulae were obtained used to classify into five types.

Linear and angular measurements
After tests, the Spearman’s rank correlation were significant at the 0.01 level (two-tailed) in linear and angular measurements.
The distance and angular measurements of the coracoid process.

Data were shown as the mean ± SD.
aValues in the same column with different superscripts are significantly different at p < .05, Type V.
bValues in the same column with different superscripts are significantly different at p < .05, Type I.
cValues in the same column with different superscripts are significantly different at p < .05, Type IV.
dValues in the same column with different superscripts are significantly different at p < .05, Type III.
eValues in the same column with different superscripts are significantly different at p < .05, Type II.
Distance measurements: et of Type I (43.92 ± 5.54 mm) was the longest, while et of Type III was the shortest (42.13 ± 6.56 mm). eu of Type IV (22.41 ± 2.96 mm) was the shortest, eu of Type I (28.06 ± 3.96 mm) was the longest. ev of Type IV (42.29 ± 5.27 mm) was the shortest, while ev of Type II (46.68 ± 4.77 mm) was the longest. ew of Type IV (84.96 ± 8.83 mm) was the shortest, ew of Type I (89.16 ± 9.63 mm) was the longest. These differences were statistically significant (p < .05) (Table 1).
The width and length measurements of the coracoid process.

Data were shown as the mean ± SD.
a,b,c,d,e Values in the same column with different superscripts are significantly different at p < .05.
aType I.
bType II.
cType IV.
dType V.Data were shown as the mean ± SD, and.
eType III.
Length measurements: eq of Type IV (15.72 ± 3.17 mm) was the shortest and significantly different from the other types. sj of Type II (22.11 ± 3.38 mm) was shorter than that of Type V (23.42 ± 2.82 mm). eh of Type IV (35.31 ± 4.21 mm) was the shortest and significantly different from the other types. These differences were statistically significant (p < .05) (Table 2).
The thickness measurements of the coracoid process.
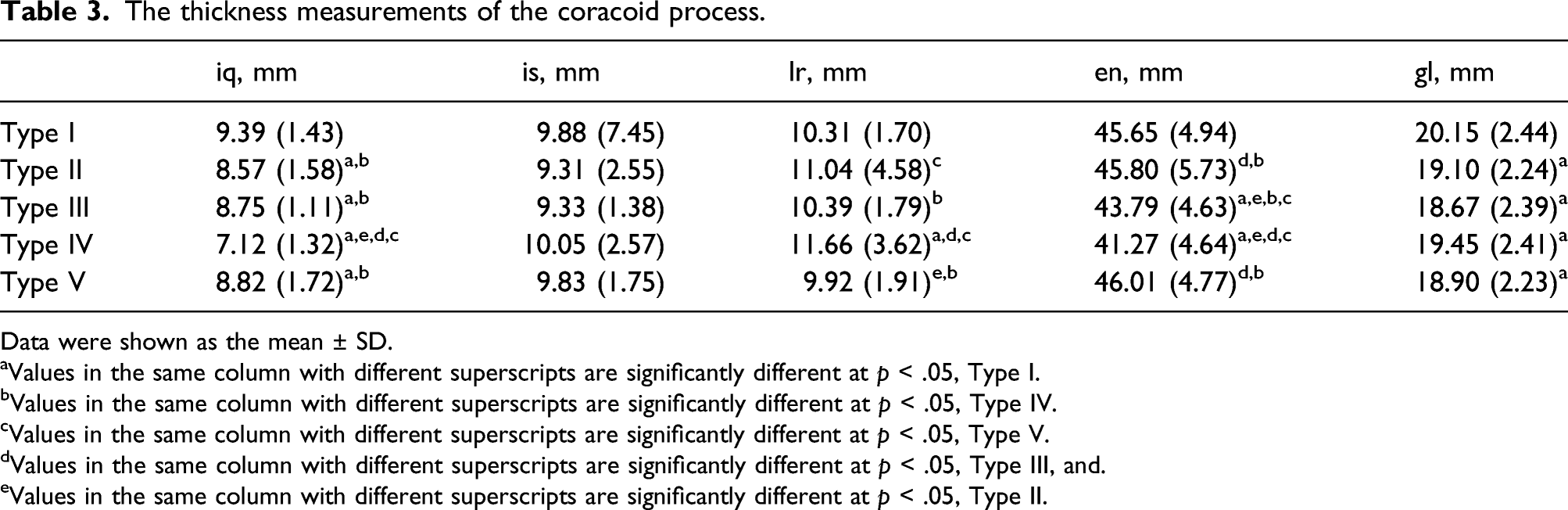
Data were shown as the mean ± SD.
aValues in the same column with different superscripts are significantly different at p < .05, Type I.
bValues in the same column with different superscripts are significantly different at p < .05, Type IV.
cValues in the same column with different superscripts are significantly different at p < .05, Type V.
dValues in the same column with different superscripts are significantly different at p < .05, Type III, and.
eValues in the same column with different superscripts are significantly different at p < .05, Type II.
Discussion
In the present study, the coracoid process was classified into five types, Type I-Vertical 8-shape and Type III- Short stick shape were more frequent in China, and Type IV-Water drop shape was the least frequent. The angles, distances, widths, lengths, and thickness of different types have significant difference. For example, the angle between tip axis and base axis of the coracoid process (∠α) of Type V (102.03°) is smaller than that of Type II, Type III, and Type IV, the precipice width of the coracoid process (cd) of Type V is shorter than that of the other types, and the length from tip to precipice of the coracoid process (eh) of Type IV is shorter than that of the other types.
The coracoid process is mentioned as the “lighthouse of the shoulder” in surgeons since one of the most fundamental principles of shoulder surgery is to embark on an approach that is lateral to the coracoid process. To avoid the vital neurovascular structures that run medially, such as the brachial plexus and branches of the axillary artery and vein. 15 Besides, The coracoid also serves as a critical anchor for many tendinous and ligamentous attachments, including the tendons of the pectoralis minor, coracobrachialis, and short head of the biceps brachii muscles, and the coracoclavicular, coracohumeral, coracoacromial, and transverse scapular ligaments. 15 Damage to any of the above structure may lead to changes in the structure of coracoid process. Therefore, a more in-depth study of the morphology of coracoid process is necessary.
In coracoid-related diseases, acromioclavicular joint dislocation is very common, which is the separation of the outer end of clavicle from acromion that is indirectly related to violence suffered by the coracoid process, since the stability on vertical direction of the acromioclavicular joint is maintained by the coracoclavicular ligament. 16 In recent years, CC ligament reconstruction using double button device17–21,6 with allografts22,23 have become a common surgical treatment, which requires to drill a bone tunnel in the coracoid process and the clavicle. The thiner sclerotin or malposition of bone tunnel on the coracoid process are liable to cause iatrogenic fracture. 24 Therefore, the position and size of the bone tunnel should be individually designed according to patient differences. In our results, the precipice width of the coracoid process of Type V is shorter than that of the other types, thus a smaller bone tunnel is recommended and surgeons should be more cautious in the procedure. And, the length from tip to precipice of the coracoid process of Type IV is shorter than that of the other types, wherefore the bone tunnel on the coracoid process is posterior to that of the other types. What’s more, the thickness from precipice to base of the coracoid process, of the Type I was thicker than that of the other types, thus drilling a deeper bone tunnel is required when surgeons reconstruct CC ligament. Therefore, according to different types of the coracoid process, surgeons could determine the treatments of acromioclavicular joint dislocation ahead and individually.
Anterior shoulder instability is also closely related to the coracoid process. Because of the main management of anterior shoulder instability, Latarjet procedure requires to free the end of the coracoid process along with the tendon, and then anchor it to the glenoid socket with screws. 25 Before osteotomy during the procedure, the exact graft length from the tip of the coracoid process is not clear. In recent years, a concept “safety margin” is described, which anterior to the insertion of CC ligament. Dolan et al. 14 described safety margin as 28.5 mm from the tip of the coracoid process. And Lian et al. 26 reported safety margin for osteotomy as 23.93 mm from the tip of the coracoid process. In the literature conducted by Lian et al., the length of the coracoid process is 42.10 mm, therefore, the graft length for osteotomy is 2 mm posterior to the midpoint of the coracoid length. In our results, the length from tip to precipice of the coracoid process of Type IV is shorter than that of the other types, thus the graft length for osteotomy is approximately 18.5 mm according to the proportion, 27 which is shorter than that of the others.
Coracoid fracture is a rare but directly related injury, accounting for approximately 3–13% of all scapula fractures, which typically occur because of high-energy trauma, such as a motor vehicle accident.28–30 Eyres et al. have proposed a classification scheme which divides coracoid process fractures into five types. 31 The specific classification is as follows: type I, tip or epiphyseal fracture; type 2, mid-process; type 3, basal fracture: type 4, superior body of scapula involved; type 5, extension into the glenoid fossa. In general, Type I, Type II and Type III of the coracoid fractures frequently treated with conservative managements whereas type IV to V frequently usually managed with internal fixation. Bhatia et al. 22 suggested that different diameters of the screws used for fixing the coracoid fracture should be recommend in different genders owing to coracoid process has a smaller diameter in females. Therefore, the choice of screw in internal fixation should be determined according to the size of coracoid process in different shapes. For example, smaller screws should be adapted for Type IV coracoid process due to the shorter diameter. To restore the anatomical reduction of the coracoid process, the orientation of internal fixation should be diverse in different types of coracoid process as well as the diameters of the screws. In the results, α of Type V (102.03°) is smaller than that of Type II, Type III, and Type IV, thus surgeons should pay attention to different orientation of internal fixation in the different types in the procedure.
However, limitations still exist in this study. Because this study is a measurement on air-dried specimens, the information about age, sex, body height, and races cannot be traced. What is more, regarding dry scapula as object, the length from the tip of the coracoid till the point anterior to the CC ligaments was not measured. And the age and gender of donors were unknown. Besides, the effect of degenerative changes of scapula on the results was not considered.
Conclusion
The coracoid process was classified into five types based on obvious morphological features. Knowing of morphological classification and anatomical parameters of the coracoid process, to some extent, may be helpful to diagnose and treat the shoulder joint disease, such as acromioclavicular joint dislocation, anterior shoulder instability, and coracoid fractures, and to theoretically reduce postoperative complications. As for CC ligament reconstruction for acromioclavicular joint dislocation, the diameter of the bone tunnel is smaller in Type V, the location of the bone tunnel is posterior to the general in Type IV, the thickness of the bone tunnel is thicker in Type I. As for Latarjet procedure for anterior shoulder instability, shorter graft length for osteotomy will be harvest in Type IV. With regard to coracoid fractures, the orientation of internal fixation is smaller than in Type IV.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Luzhou People’s Government - Southwest Medical University Shi-zhen Zhong Academician Talent Team Sub-project (2018zszysrctdxm), Southwest Medical University Research Project (2020ZRQNA045) and 2020 Orthopedics (Shangantong) special scientific research project of Sichuan Medical Association (2020SAT26).
Author’s Note
These authors contributed equally to this work.
Data and materials availability
The data and materials used and analyzed during the current study are available from the corresponding author on reasonable request.