
Abstract
Purpose
It is known that the incidence of paediatric orthopaedic trauma peaks in the summer months as a result of increased and uncontrolled physical activity. The aim of this study was to review the experience of a single centre with paediatric orthopaedic traumas and determine the relationship between the severity and the variations in the incidence of traumas in relation to the seasons and temperatures during the study period.
Materials and Methods
A single institutional review of the historical data of all patients aged 0–16 years who presented for orthopaedic trauma between January 2018 and December 2020 in the emergency department of Level 1 tertiary orthopaedic trauma centre was conducted. 65,182 paediatric orthopaedic trauma cases had been retrieved from the hospital data base during the 3 -year study period. We classified the traumas according to the variants of the patients’ and by holidays, seasons, school days and weekends, months and in which part of the body it occurred.
Results
After excluding the summer vacation, 77% of paediatric orthopaedic trauma patients attended to the hospital on weekdays and 23% on weekends. While it was observed that hot weather had a statistically positive effect on trauma attendance, rainy weather had an negative effect (p < 0.05). Trauma attendances were found to be statistically higher in summer months, except for injuries that may occur with indoor activities such as metacarpal fracture, phalanx fracture and pulled elbow (p < 0.05).
Conclusion
Orthopaedic trauma at a Level 1 tertiary health care trauma center do vary significantly with the weather and are highest in the summer season. Therefore, it should focus more attention on preventive strategies for paediatric trauma in the summer season.
Introduction
Fractures are common orthopaedic problems in children that in most cases require urgent or emergency intervention and significantly affect the child and family’s daily life.1,2 These unforeseen emergencies can place a significant burden on medical resources and often result in medical staff overload and a shortage of hospital rooms. They have potentially substantial social and economic consequences, both in the short and long term.2,3 These effects can be a systematic factor in providing inappropriate medical care. Sports and games are the leading causes of paediatric fractures,1–4 and the vast majority of major paediatric injuries in emergency departments are fractures. 5 Evaluation of the incidence and presentation of paediatric fractures is needed to take appropriate preventive measures to allocate and plan the correct medical workforce and resources.
Previous studies have reported that the incidence of certain fractures varies by age, season, weather and day of the week.6–13 These studies provide information on risk factors for fractures and possible preventive measures. On the other hand, most studies are limited to specific fractures, certain age groups and specific hospitals. Population-based data are lacking in these studies, particularly those covering the population across the country.14–18
A common belief was that holidays and vacations are associated with injuries. However, the effect of increasing or decreasing the breakage rates of the summer peak is somewhat inconsistent.9,19–22 Most studies have shown unimodal variability during warm seasons and peaks, especially in summer.9,19–22 Most of these studies were conducted in cold climates and may not represent fracture rate variability in hot countries; It may also not fully reflect the new generation children’s lifestyle.19,22–24
Coronavirus disease-19 (Covid-19) is a serious acute respiratory syndrome caused by a new coronavirus and was declared a pandemic by the World Health Organization on 11 March 2020, when the first cases were officially announced in Turkey. 25 Since this date, schools in Turkey have continued to teach via distance online education and restrictions on going out of the house began.
The primary aim of this study was to review the experience of a single centre with paediatric orthopaedic traumas and determine the relationship between the severity and the variations in the incidence of traumas in relation to the seasons and temperatures during the study period and the secondary aim of the study is to compare this 3-year period with each other as the pre-Covid and Covid pandemic period.
Materials and Methods
A single institutional review of historical data was conducted in a Level 1 tertiary orthopaedic trauma centre. All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as amended in 2008. Informed consent was waived due to its retrospective nature. We used the search engine in the hospital’s electronic archive to search for patients under 16 treated in the emergency department between 01 January 2018 and 31 December 2020. The patients were screened to identify those coded as fractures or dislocations according to the International Classification of Diseases (ICD) −9 (805 ** to 839 **). 26
Dates were chosen in accordance with the local computerised recording system. An orthopaedic surgery resident or attendant made a diagnosis in the emergency room. We excluded duplicate reference records for the same injury. Head and rib fractures were excluded because they were not treated in our department. Presentation timing and limb involvement were also collected, as well as a patient’s demographic data. The dates were designated as vacation days (non-school days out of work), summer vacation (01 July–30 August) and school days. In addition, the location of the fracture of the body parts were evaluated separately by the season of the year. The patients were divided into two main groups, 2018 and 2019 as the prepandemic period and 2020 as the pandemic period.
Weather data were collected using the online Turkish Meteorology Services archive for minimum and maximum daily temperatures and rainfall level. 27 These values were generalised over the entire field of study and were similar to previous years’ readings. Summer holidays in Turkey also occur during the hottest months of the year, June, July and August. The hospital where the study was conducted is a Level 1 tertiary trauma centre and serves approximately three million people, in addition, approximately 30% of the population in this region is under the age of 16 and the annual population growth rate is 7.8%. 28 During the study, the total number of paediatric patient attendances to our hospital was reviewed using the hospital’s information processing system (Panates Software System/Istanbul/Turkey). Approximately 926,626 paediatric patient attendances had been made.
Statistics
The IBM SPSS Statistics 22 (IBM SPSS, Turkey) program was used to evaluate the study findings. The suitability of the parameters to the normal distribution was assessed with the Shapiro Wilks test. The Chi-square test and Fisher’s Exact Test were used in the comparison of qualitative data. Spearman’s rho correlation analysis was used to examine the relationships between parameters that did not conform to normal distribution. A Poisson regression analysis was conducted for multivariate analysis. Significance was evaluated at the p < 0.05 level.
Results
Evaluation of trauma rates according to gender.
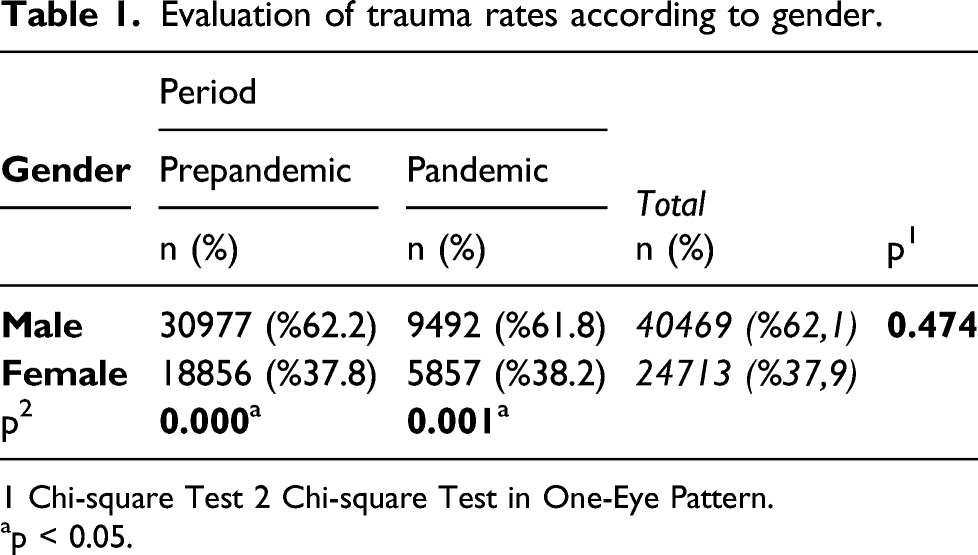
1 Chi-square Test 2 Chi-square Test in One-Eye Pattern.
ap < 0.05.
Evaluation of the rates of hospitalised trauma patients.
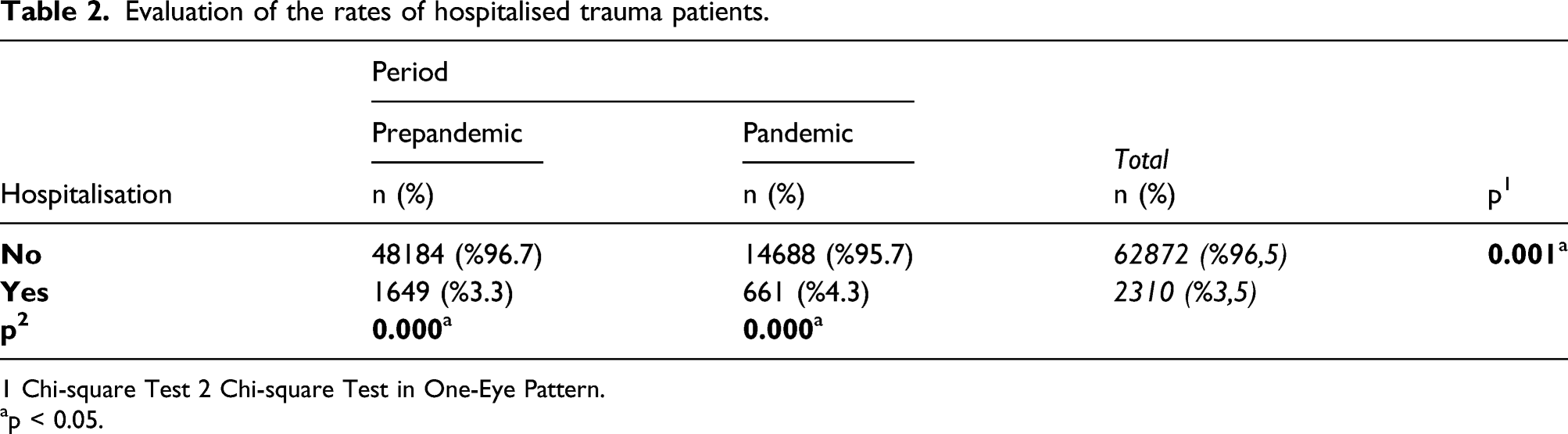
1 Chi-square Test 2 Chi-square Test in One-Eye Pattern.
ap < 0.05.
Evaluation of the rates of operated trauma patients.

1 Chi-square Test 2 Chi-square Test in One-Eye Pattern.
ap < 0.05.
Evaluation of trauma attendance rates between seasons.
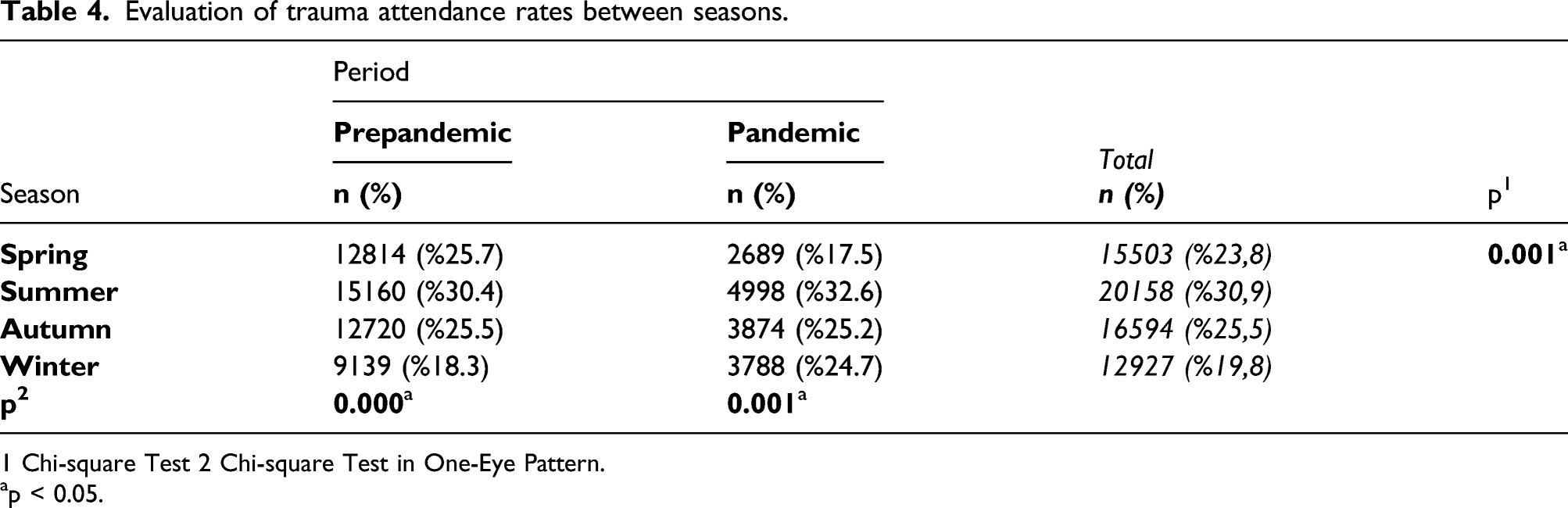
1 Chi-square Test 2 Chi-square Test in One-Eye Pattern.
ap < 0.05.
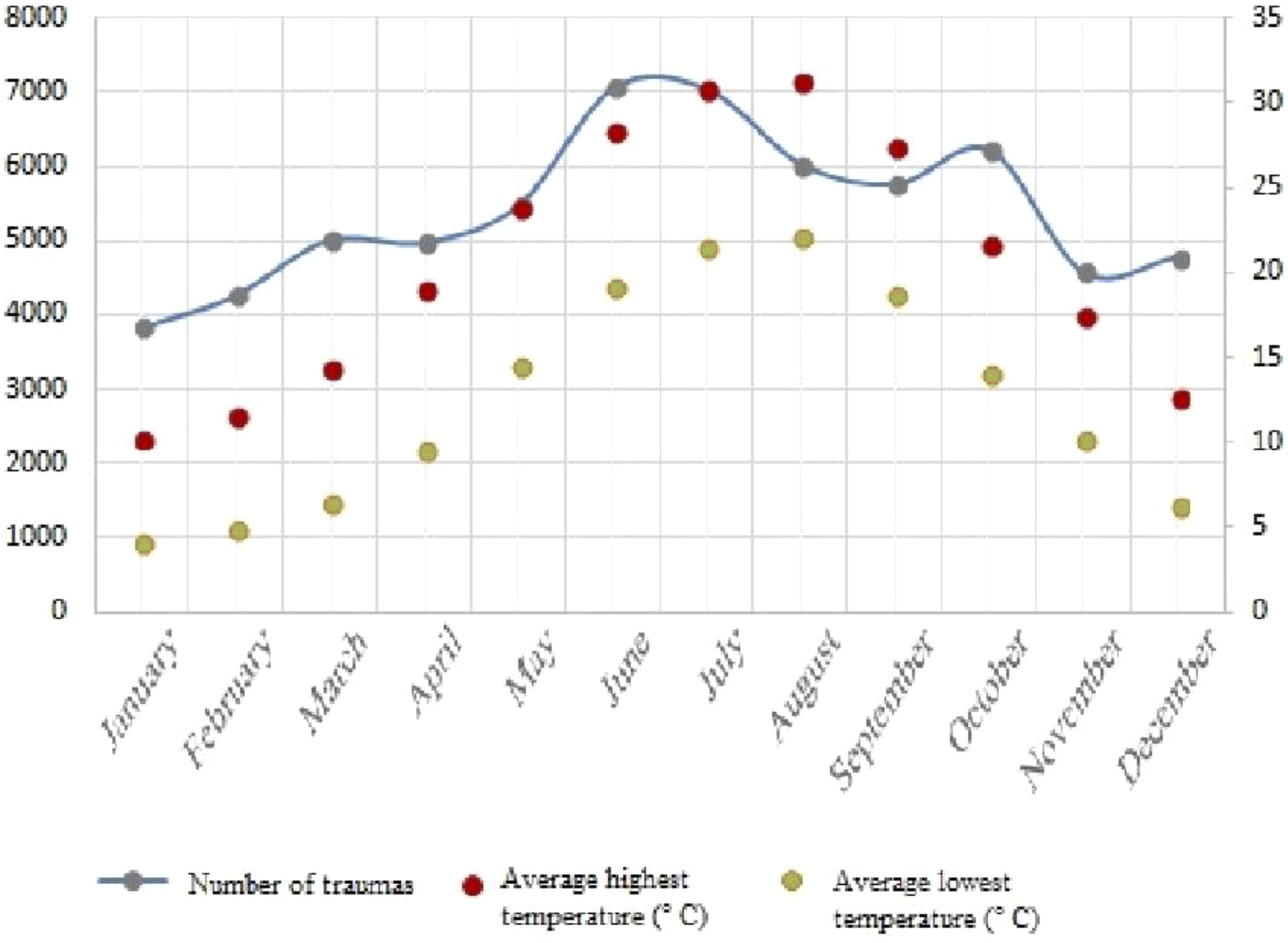
Weather and paediatric trauma risk (left Y axis: number of fractures, right Y axis: degrees (Celsius)).
Evaluation of the trauma rates of operated between seasons.

1 Chi-square Test 2 Chi-square Test in One-Eye Pattern.
ap < 0.05.
An evaluation of attendances to the hospital based on meteorological parameters yielded the following findings (Table 6): There was a positive statistically significant correlation between hospital attendances and the average temperature, average high temperature, average minimum temperature and average daily sunshine, respectively (p: 0.000; p < 0.05). There was a reverse 78.8% and statistically significant correlation between hospital attendances and the average number of rainy days and average monthly rainfall, respectively (p: 0.002, p: 0.028; p < 0.05). Evaluation of the correlation between the attendances and the parameters of temperature, sunshine duration and rainfall. Spearman Rho Correlation Analysis. ap < 0.05.

Evaluation of the effects of the attendances on temperature, sunshine duration and rainfall parameters by Poisson regression analysis.

ap < 0.05.
Discussion
Many studies reported that the number of people who visit a trauma centre on any given day is partially affected by weather.1–3,7,9,19–21,29,30 Seasons are represented differently by a wide range of weather events and temperatures. We identified seasonal, weather and timing factors associated with paediatric trauma attendance. Using a multivariate model, we identified the relationships between trauma attendance rates and seasonal and temperature values.
In a study in Sweden by Landin, the incidence of paediatric fractures peaked between May and August from 1950 to 1979, with only a slight decrease in July. 3 In later studies conducted in Sweden, Norway and the United Kingdom, similar results were reported, especially during the first snowy days or winter sports weeks. The increased incidence has been observed.1,19,20
In a 2003 UK study of seasonal variation of forearm fractures, the highest fracture rates in children were reported in the spring rather than the summer months, although the rate was still high during the summer months. 10 Researchers from the UK (2005) 9 and Boston (2016) 21 found that the highest rates of trauma consultation occurred on hot and dry days outside of school but also noted that the rate of increase declined during the peak of summer. In their study, the incidence was small in the middle of summer, and rates were still higher than most of the year. These studies showed that although the warm season as a whole was more dangerous, it was spring and not summer when fracture rates were highest. Moreover, the studies projected that summer fracture rates might increase in the future.
In our region, where the Mediterranean climate prevails, the difference between spring and summer is even more critical. On the other hand, Segal et al. reported a bimodal peak in the incidence of fractures in the spring and autumn in Israel, which has similar climatic characteristics to our country. The fracture incidence was the lowest in the summer. 31
In this study, we observed that traumas other than metacarpal fracture, phalanx fracture and pulled elbow were higher during the summer months. We believe this is because these traumas generally involve less energy trauma and can occur at home. The fractures caused by high energy trauma in the summer months might be because children are more involved in outdoor activities. In previous studies, a variety of reasons were proposed for seasonal changes in the incidence of refraction. Those included changes in outdoor activity due to weather conditions, changes in vitamin D metabolism due to the change in day length, increased slippery ground in winter and reduced visual acuity due to early sunsets in winter.32–39 Studies have reported that most paediatric fractures are primarily due to outdoor injuries during sports activities; regular daily vigorous physical activities increased the risk of fracture.4,40
This study found a statistically significant relationship between the increase in mean air temperature and paediatric fractures; this finding was consistent with the literature.21,41 We believe it was because children are less likely to attend outdoor activities in rainy weather. In parallel with the literature, we found a statistically significant decrease in fracture incidence in seasons with high total rainfall. 42 A study from Scotland evaluating children’s emergency attendances over 3 months in the summer found that more trauma attendance occurred on sunny, hot days than cloudy, cooler days. 43 In a study conducted in the United Kingdom, increased maximum daily temperature was associated with more paediatric and adult trauma attendance, with children affected more than adults. 44 The results of our study are consistent with these reports. However, we adopted a more detailed approach to each application by evaluating temperature and precipitation seasonally and monthly rather than general daily temperature.
The pattern of injuries in the paediatric population is essential for the planning and management of trauma systems. Injuries are the leading cause of death in children after infancy. Children and adolescents are recognised to have a specific set of injury patterns, severity, aetiology and consequences associated with major trauma. 45
In many studies conducted around the world following the Covid-19 pandemic, it has been shown that trauma attendances decreased significantly in the paediatric population during the pandemic period.25,46,47 In the current study, similar to other studies, it was determined that paediatric trauma attendances decreased significantly during the pandemic period. However, in the prepandemic period, distal radius fracture, metacarpal fracture, pulled elbow, metatarsal fracture and phalanx fracture were significantly higher than the pandemic period; it was determined that there was no significant difference between the prepandemic period and the pandemic period in the traumas of clavicle fracture, humerus fracture, forearm fracture, femur fracture, tibia fracture and femoral neck fracture. We think that the reason for this may be that children were less exposed to fractures caused by minor trauma due to the restrictions on going out during the pandemic period, as they were less involved in activities outside the home.
Limitations
The primary limitation of the study was its retrospective nature. We assumed that our study cohort represented the general population. We did not collect data on fracture risk factors such as medications or chronic diseases. The study relied on data collected from the trauma logbooks of hospital computer systems to create a multivariate model. These limitations constitute the adaptability of the results in the study. To increase the adaptability of the results to the general population, a variety of paediatric and adolescent trauma patients and patients referred to us from other centres were also included in the study cohort.
This study’s findings were based on the experience of only one centre, which may limit the applicability of the results. While data from individual hospital records may limit understanding and explaining the phenomenon, extensive epidemiological studies may reflect regional or national trends and distributions. These limitations constitute the applicability of the results in the study. However, despite these limitations, the general trends in seasonal variations and their effect on paediatric trauma are widely applicable to temperate regions in the Northern Hemisphere.
A positive feature of this study was that it was conducted on a larger cohort than similar studies conducted to date and included traumas common in the paediatric period, such as pulled elbow and phalanx fracture. In addition, although our study was limited to Turkey’s social, economic and climatic characteristics, they were similar to countries such as Greece, Italy, Spain, the United States of America (USA, California), Chile and Lebanon, etc. These countries have similar climatic characteristics (Mediterranean) in which four seasons are experienced.
Conclusion
Local seasonal variations in paediatric fractures appear to be highest during the summer months. These rates may reflect the transition to a more active lifestyle with more outdoor activities during summer vacations. In our country, which is located in the northern hemisphere and Mediterranean climate prevails, the summer season includes the months of June, July and August, and the average temperature of these months during the working period is 25.1°C and it is observed that there is an increase in paediatric trauma attendance with the increase in mean air temperature. On the other hand, paediatric trauma attendance rates decrease on days with increased daily precipitation. The increased pattern of hospital attendances observed during the summer months should aid resource planning. Moreover, it should focus more attention on preventive strategies for paediatric trauma. We believe that a prospective study analysing the data presented, followed by more detailed data on specific injury mechanisms, could help improve injury prevention measures and medical resource routing. Additionally, with the overall increase in temperature resulting from climate change, 48 these data can provide information on changes in the epidemiology of paediatric trauma over time. As global temperatures slowly rise, there may be a corresponding increase in paediatric trauma referral rates.
Footnotes
Acknowledgements
We thank Sibel Kanat for assistance in the statistical analysis of our data and preparation of table for this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors. All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as amended in 2008.