
Abstract
The advancement in science and research has led to development of medical maggots which feed exclusively on dead tissue. Medical maggots have three important functions namely debridement, disinfection, and stimulation of wound healing. The modern use of medical maggots now goes by the term “Maggot Debridement Therapy” (MDT) for use in wound management. MDT is still used infrequently due to the effectiveness of surgical debridement and antibiotics for treatment of wound infection. Lately, there was emergence of Multi-Drug Resistant Organism (MDRO) likely due to inappropriate antibiotics usage. Maggot secretions have been shown to be effective in inhibiting some MDRO, for example, Methicillin-resistant Staphylococcus aureus, thus making MDT an attractive option for wounds with MDRO. We report two patients with multiple medical comorbidities, diagnosed with serious MDRO Diabetic Hand Infections treated with three cycles of MDT followed by Negative Pressure Wound Therapy.
Introduction
The medicinal value of maggots has long been known to the Australian Aborigines, Burmese, Chinese, and Mayan people who used maggots to heal wounds around 2000 BC. 1 Modern use of Maggot Debridement Therapy (MDT) for bone and soft tissue infections was first introduced by William Baer in 1931. 2 Baer used MDT for 21 patients with chronic osteomyelitis. The wound of these patients healed well after MDT.2,3 The subsequent approval of MDT by the United States Food and Drug Administration in 2004 allowed this therapy to be used worldwide in wound management. 1 MDT has three benefits namely, debridement, disinfection, and stimulation of wound healing 3-8. Maggots debride by secreting proteases which dissolve necrotic tissue and infective material.3,7,8 These medical maggots also have modified mandibles called “mouth hooks,” and they have some rough bumps around their body which poke the dead tissue and physically remove these unhealthy tissues.1,6 Maggots gut secretion is a disinfectant that may inhibit growth of organisms including Staphylococcus aureus, Streptococcus pyogenes, Methicillin-resistant Staphylococcus aureus, and to a lesser extent Pseudomonas aeruginosa.5,9-11 Furthermore, maggots secrete enzymes at the wound bed which may stimulate fibroblast proliferation, neovascularization, and growth of granulation tissue to help the wound heal.3,7,8,12 Maggot crawling can also increase local temperature, stimulate growth factors, and alter electrical potential on the wound bed.3,7,8 The use of MDT declines after the introduction of effective antibiotics, modern dressings, and disinfectants. Nevertheless, now there is a surge in Multi-Drug Resistant Organisms (MDRO) in chronic wounds resulting in no appropriate antibiotics for treatment. MDT becomes more relevant in these cases.
MDT is more commonly used for lower limb wounds. 4 The usage in hand wounds is rare. A large case series showed the use of MDT in hand wounds is only 1.5% compared to 90.5% cases in lower limb wounds. MDT has an important advantage in hand wounds. 4 Every gram of tissue in the hand is important for hand function. Precise microsurgical debridement of only devitalized tissue is of the utmost importance for hand wounds. It may not always be easy to distinguish the border of devitalized tissue and healthy tissue in the hand during surgical debridement. Maggots can help by only debriding the dead or necrotic tissue. 6 They do not feed on healthy tissue.3,7 Maggots can also help to create a boundary between necrotic and healthy tissue to aid future surgical debridement if required.3,7,10
MDT is an alternative biological debridement option for patients who are not fit for surgery or for patients with chronic wound that have failed other options of treatment. 13 We report two patients with serious MDRO infection of the hand in which undergoing repeated debridement surgeries was not possible due to patients’ multiple medical comorbidities. Both patients were eventually successfully treated with three cycles of MDT followed by Negative Pressure Wound Therapy (NPWT).
Case report
A 71 year-old female, right hand dominant, had underlying uncontrolled diabetes mellitus, hypertension, and end-stage renal failure on hemodialysis using the left internal jugular vein catheter for the past 3 years. She already had amputation of her left thumb and bilateral below knee amputation in the past for serious infections. She presented with gradual onset of throbbing pain in her left hand for 2 months and discoloration of the palm following an ipsilateral brachiocephalic fistula creation 4 months ago. She was diagnosed with wet gangrene of left palm due to left brachiocephalic fistula steal syndrome. Subsequently, she underwent emergency ligation of the fistula by the Vascular team and debridement of the left hand and ray amputation of left middle finger by the Orthopedic Hand team. Intraoperative tissue culture grew Morganella morganii, Enterococcus faecalis, and Carbapenem Resistant Escherichia coli. She required multiple surgical debridement every two to 3 days due to recurring slough and uncontrolled infection. She also had a combination of multiple antibiotics, including clindamycin, piperacillin/tazobactam, cefepime, ampicillin, meropenem, and colistin, as advised by the Infectious Disease team, to treat the MDRO. However, the wound condition did not improve. Three cycles of MDT were applied to the wound. Application of dressing was easy, and steps were shown in Figure 1. The supplier of medical maggots brought new maggots for each cycle of dressing. These maggots were stored and transported in a small container placed in an ice box to keep the maggots dormant in a temperature of less than 10 degrees Celsius. The wound size was measured and the criteria of 5–10 maggots/cm2 was strictly adhered to. This patient wound size was about 30 cm2. Normally, we only calculate the size of the wound covered by slough. Therefore 150 medical maggots required for this patient per cycle with the total cost of RM 325 (USD 80) per cycle (including cost for maggots of RM1.50 per maggot, cost for dressing set of RM50, and nursing charge of RM50). Each cycle was 3–4 days because that was the life cycle of medical maggots Lucilia cuprina used in Malaysia. We avoid leaving the maggots for more than 4 days to prevent Blowfly strike. These medical maggots were developed by Institute of Medical Research (IMR) and further commercialized by a local distributor. The wound was cleaned with normal saline before applying medical maggots. It is important not to use other modern gel dressing such as hydrogel at the same setting as it reduces the effectiveness of these maggots. A sturdy dry gauze fence held in place with plaster was used to surround the wound, and the wound was tightly bandaged. We did not find it necessary to seal the wound using transparent dressing. Dressing was changed every three to four days. Physiotherapy was done regularly. After completing one cycle of MDT, maggots increased in size and were removed by irrigation using normal saline and disposed as per medical waste. After three cycles of MDT, there were reduced slough, increased granulation tissue, and significant reduction in inflammatory markers (Figure 2). A repeat tissue culture showed successful eradication of MDRO. Subsequently, we applied two cycles of NPWT to further improve the growth of granulation tissue. We planned for wound coverage; however, patient was not keen for any further surgical procedure. Based on our experience, we used medical maggots for at least three cycles for most wounds. We would decide to stop maggot therapy once at least 80% of slough had been removed from the wound bed and will start using NPWT after that to further promote granulation. This patient stayed in hospital for 51 days due to multiple surgical debridement to control the infection. At the end of treatment, the range of motion of the index finger metacarpophalangeal joint (MCPJ) was 0–80°, proximal interphalangeal joint (PIPJ) was 0–60°, and distal interphalangeal joint (DIPJ) was 0–5°; ring finger MCPJ was 40–80°, PIPJ was 30–100°, and DIPJ was 5–30°; little finger MCPJ was 30–80°, PIPJ was 20–90°, and DIPJ was 5–60°.

Step by step guide for application of maggot dressing. The first step is to build a sturdy fence using gauze and plaster. Subsequently, aspirate saline into pipette and squirt it into a test tube containing dormant maggots that are kept in a coolbox to maintain temperature of less than 10 degrees Celsius. Aspirate maggots with saline solution using pipette. Drop the maggots onto a sterile gauze. Apply the gauze onto wound and finally secure with bandage.
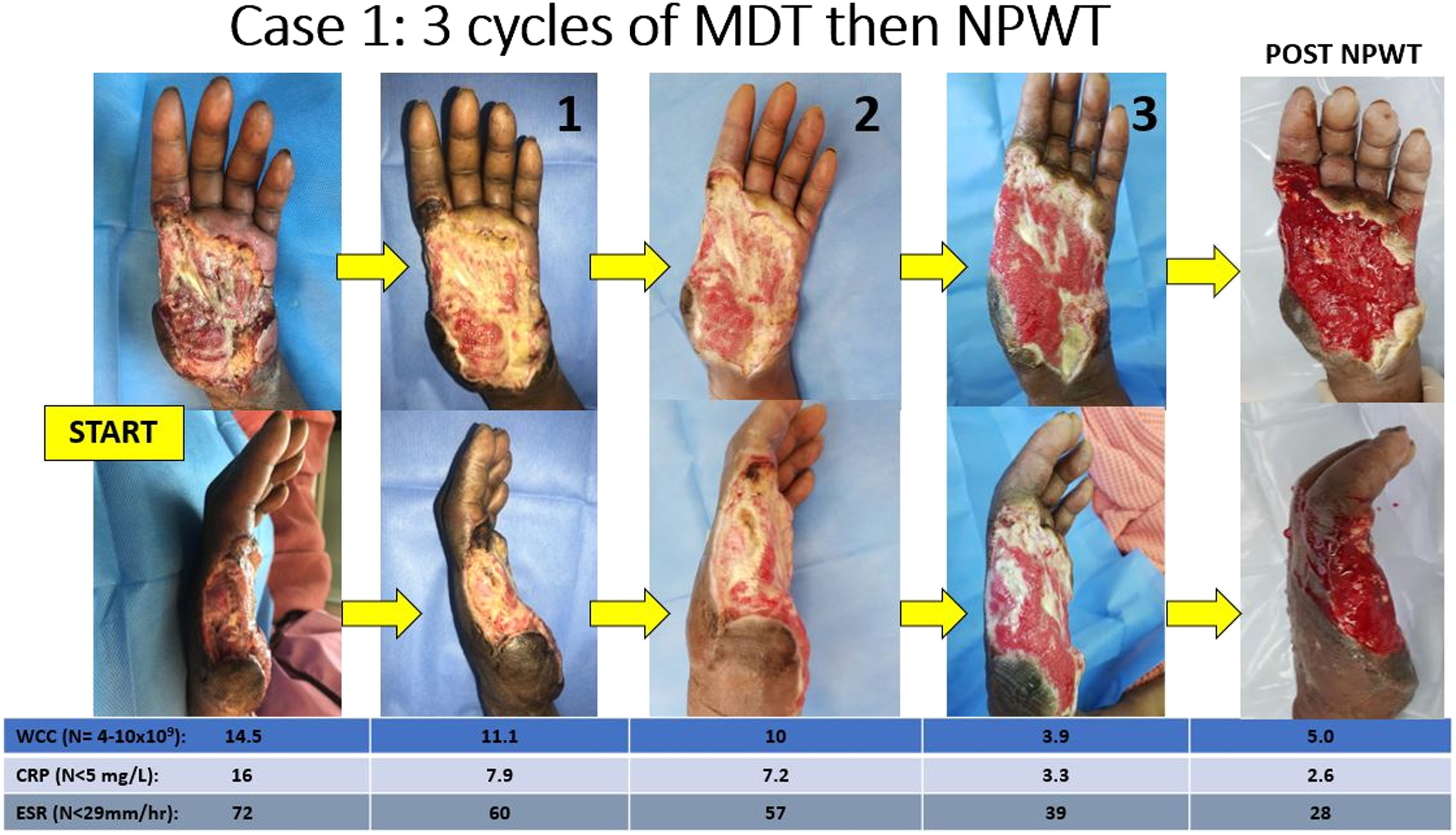
Wound healing after 3 cycles of maggot debridement therapy (MDT) for case1. Labels 1, 2 and 3 indicate the wound condition after number of cycles of MDT. The last photo on farrightis after completion of negative pressure wound therapy (NPWT) WCC-white cell count, CRP-C-reactive Protein, ESR-erythrocytese dimentation rate (Normal reference range).
A 56 year-old female, right hand dominant, retired dental assistant, with underlying poorly controlled diabetes mellitus, congestive cardiac failure, and history of right transtibial amputation and left third toe ray amputation, presented with left palm swelling for 4 days. She accidentally cut her left palm while cutting vegetable using a knife 1 week ago. On presentation, her left ring finger was kept in flexion with pus discharge beneath the hyperkeratotic skin on her left palm. The clinical diagnosis was left ring finger flexor tenosynovitis with extension to the left palm. She underwent urgent surgical debridement of left ring finger and left palm. Extensive slough and pus were found over the left ring finger extending to the palm. Four days after the surgery, her left ring finger became gangrenous. She subsequently underwent ray amputation of the left ring finger. Tissue and bone culture grew Extended Spectrum Beta Lactamase inducer Escherichia coli and Pseudomonas aeruginosa. The patient was treated with intravenous cefepime based on sensitivity results for 6 weeks to treat for osteomyelitis. Nevertheless, the wound remained unfavorable with multiple small islands of slough scattered throughout (Figure 3). Three cycles of MDT were applied, and steps were described as per Case 1. The wound size covered by slough was 50 cm2. This patient required 250 maggots per cycle of maggot therapy. The medical maggot used was also Lucilia cuprina developed by IMR. Total cost of dressing was RM475 (USD 120) per cycle (including RM1.50 per maggot, RM50 for dressing set, and nursing charge of RM50). Three cycles of MDT were used used for the wound. There was clinical improvement as evidenced by reduction in slough, increased in granulation tissue, and no clinical signs of infection. Subsequently, NPWT applied to further improve granulation tissue growth (Figure 3). The wound subsequently healed by secondary intention. This patient was not compliant with physiotherapy. She was diagnosed with depression and had low mood and low motivation in the ward. The total hospital stay was 61 days. At the end of treatment, range of motion of all fingers were limited with joint contractures due to poor compliance to physiotherapy.

Wound healing after 3 cycles of maggot debridement therapy (MDT) for case 1. Labels 1, 2, and 3 indicates the wound condition after number of cycles of MDT. The last photo on far right is after completion of negative pressure wound therapy (NPWT) WCC-white cell count, CRP-C-reactive Protein, ESR-erythrocytese dimentation rate (Normal reference range).
Discussion
Most countries use medical maggots Lucilia sericata.1,6,8,11-17. In our setting, the species available is Lucilia cuprina. Study conducted by Arora and colleagues showed that Lucilia cuprina had similar antimicrobial activity against Staphylococcus aureus and Escherichia coli. Another local study had also shown Lucilia cuprina can effectively debride wounds. 18 Therefore, both species could be used in MDT.
The indications of MDT are diabetic foot ulcer, pressure sore, chronic lower limb wounds, traumatic wounds, and venous ulcers.1,3,7,8,16,19 There were reports of good wound healing after use of MDT in several off-label indications such as palliative malignant wound and ischemic wound.4,17,20 Meanwhile, the contraindications of MDT are allergy, infected wound causing severe sepsis requiring emergent debridement, exposed large blood vessels, sterile body cavity, and entomophobia.3,7,8 Critical limb ischemia (Ankle Brachial Systolic Index < 0.6) is a relative contraindication to MDT. 14
Two methods of application of maggots to wound bed described in the literature were free larvae and bagged larvae. 13 Theoretically, maggots need to be freely crawling to exert physical debridement effect. However, a recent randomised controlled trial conducted by Dehghan and colleagues to compare these two methods have shown similar efficacy of debridement 21 .
A review of literature showed many studies reporting success in using MDT in lower limb wounds. Mumcuoglu and colleagues treated 656 lower limb wounds using maggots in hospitalised and ambulatory patients. 19 Majority of wounds were diabetic, arterial, and venous ulcers. 19 Majority of wounds had adequate debridement with only 1.1% cases were deemed ineffective. 19 Another study reported the off-label use of MDT in critical limb ischemia of the lower limb resulting in wound healing and improved skin perfusion in 2.5 months. 20 There were also many reports on the use of MDT in diabetic foot ulcers, lower limb degloving wounds, and necrotizing fasciitis wound after surgical debridement with successful wound healing 8,12,16,18,22. Furthermore, Paul and colleagues conducted a case–control study comparing MDT and surgical debridement in which they found the effectiveness of biological debridement using MDT was comparable to surgical debridement. 23 This study concurs with the findings of Blaizot and colleagues who conducted a trial to compare the effectiveness of debridement of MDT and other dressings. 6 They found that maggots debride faster than many other dressings as early as 1 week follow-up. 6 To sum up, MDT is a well-established and effective biological debridement option used for lower limb wounds. Despite that, MDT is still considered the “last resort” by many wound clinicians.1,3,4,7
The use of NPWT in combination with MDT has been described in the literature.4,22,24,25. One case series showed combination of MDT and NPWT in up to 36% of cases in large wounds and 6% in small wounds 4 . MDT helps with debridement and disinfection. Meanwhile, NPWT helps to remove exudates produced by maggot secretions once completed MDT. 25 Both MDT and NPWT also improved neovascularization of the wound bed which is important for wound healing.24,25
The use of MDT in hand wound is still rare. Von Beckerath and colleagues conducted a study to look at the trend of using MDT in hospitalised patients in Germany and found that the use of MDT for hand wounds was less than 1% of all cases from 2011 to 2016. 4 Chan and colleagues reported a patient who presented to hospital 2 days after sustaining crush injury of the hand, in which the wound was infested with maggots. 26 The authors found very little devitalized tissue in the wound. 26 They believed the maggots perhaps reduced bacterial load in the wound and hence prevented the patient from dying of sepsis. 26 The advantages of maggot used for lower limb should generally be applicable to upper limb as well. When compared to radical surgical debridement and complex flap procedures for hand wounds, MDT was safer, more cost effective, easier, and allowed shorter hospital stay because dressing could be changed in the outpatient setting.15,19 On top of that, patients with multiple comorbidities and poor cardiac function might not be able to undergo multiple surgical debridements or long complex flap reconstructive surgery. Nevertheless, the strict precaution of using MDT is to adhere to the application of 5–10 maggots/cm2 size of the wound and changing the dressing every 3 days to avoid Blowfly strike. 1 Blowfly strike is a condition caused by either too many maggots applied to the wound or the maggots left too long in the wound. These maggots grow and replicate to invade blood vessels and produce side products such as ammonia at a high concentration that might suppress immune function and cause encephalopathy.3,7,10. This side effect of MDT is rare when adhere to the manufacturer’s recommendation.
We found two studies on use of MDT for hand wounds 27,28. Bohac et al. described the use of MDT followed by NPWT for fungal infection of the hand. 27 The wound was colonized by Proteus after MDT, which the author treated with ciprofloxacin. Nevertheless, the wound had favorable outcome. Jiang et al. described the use of MDT for severe diabetic hand in a patient with multiple comorbidities not suitable for surgery. 28 MDT was shown to be an effective biological debridement tool for the wound. Two patients described in our case report also showed good debridement potential of medical maggots for hand wounds, which supports Bohac and Jiang’s study. However unlike Bohac's patients, our cases were not colonized by Proteus after MDT. 27 The advancement in sterilization of maggots has improved the success rate and safety of MDT. 29 Even though one study has shown that Proteus mirabilis, a maggot gut commensal, was unable to be removed by the sterilization process, this organism produces a bactericidal agent to kill other pathogenic bacteria that colonise the wound bed.29,30 We did not prophylactically treat patients on MDT with ciprofloxacin because of concerns of rapid emergence of resistance to ciprofloxacin in the setting of treating chronic wounds with MDRO. In most cases, the residual Proteus mirabilis colonising the wound may inhibit more virulent bacteria which might invade and cause wound infection.
By further literature search, we found two studies that showed the synergistic effect of antibiotics and maggot secretions against Methicillin-resistant Staphylococcus aureus.5,9 The maggot secretions were shown to modulate and slow the development of resistance to ciprofloxacin. 9 Another study reported that patients who used MDT had shorter course of antibiotics treatment. 12 On the other hand, there was a report on unsuccessful use of MDT for pyoderma granulosum wound colonised by Escherichia coli and Pseudomonas aeruginosa. 31 The author claimed that the ability of these organisms to produce biofilm might have inhibited the action of maggot secretions. 31
Both our patients had chronic MDRO infection of the hand which was resistant to all available antibiotics and repeated surgical debridement was not feasible. The wound condition improved after three cycles of MDT followed by NPWT. Contrary to the study above, one of our patients with hand wound infected with Escherichia coli and Pseudomonas aeruginosa had favorable clinical outcome after MDT. Therefore, MDT can be used even if the wounds are colonised with these organisms. Our patients were able to perform physiotherapy when using MDT. There were no side effects associated with use of MDT in both our patients. Both patients also did not have entomophobia and were able to tolerate the minimal “crawling sensation” caused by the maggots. The discomfort was minimal, and both patients slept well during treatment.
For hand wounds, granulation tissue is not desirable because it causes contraction, adhesion, and prevents smooth gliding of tendons 32 . However, all our patients had multiple medical comorbidities and were not suitable candidates for complex flap surgery to cover the wound. Their main expectation was to avoid another amputation. Therefore, our aims were biological debridement, to control infection, promote granulation, and finally wound coverage using skin graft.
Conclusion
In conclusion, MDT is an alternative biological debridement method that should be kept in mind when managing complex hand wounds. It may also be used synergistically with antibiotics for MDRO infected wounds to control infection and promote wound healing especially in patients with multiple comorbidities who refuse amputation and who are not suitable candidates for complex wound reconstruction and coverage surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.