
Abstract
Purpose
To report the arthroscopic and clinical findings of patients with extensor carpi ulnaris (ECU) tendinopathy treated with wrist arthroscopy and open surgical repair.
Methods
We retrospectively reviewed the medical records of seven patients with chronic ECU tendinopathy who were treated with diagnostic wrist arthroscopy and open surgical repair between 2010 and 2017. Seven cases diagnosed with ECU tendinopathy had undergone open procedure for the ECU tendinopathy, as well as wrist arthroscopy in the same session. Any pathology of the triangular fibrocartilage complex (TFCC) diagnosed by wrist arthroscopy were treated simultaneously with open procedure for the ECU tendinopathy. The functional outcome was evaluated by comparing the preoperative and final follow-up values of range of motion (ROM), grip strength, visual analog scale (VAS) for pain, modified Mayo wrist score and quick disabilities of the arm, shoulder, and hand (DASH) score.
Results
TFCC tears were identified in four patients of which repair was performed concomitantly. The average follow-up period was 39 months (range, 25–49 months). At the final follow-up, all the outcomes including average VAS score (6.4→1), the ROM (173→192°), quick DASH score (42.5→18.2), and modified Mayo wrist score (48.6→79.3) improved significantly.
Conclusion
When treating patients with ECU tendinopathy, the possibility of TFCC combined injury should always be considered. If surgical treatment is planned, we suggest a wrist arthroscopy for more accurate diagnosis an intra-articular pathology, particularly for patients whose MRI findings suggest a degenerative tear or degeneration at the periphery of the TFCC. Additionally, if ECU and DRUJ stability is obtained by repair or reconstruction of the concurrent pathologies in the ECU subsheath, TFCC and other intra-articular structures, the results will be favorable.
Introduction
The extensor carpi ulnaris (ECU) tendon and its subsheath (fibro-osseous tunnel) are an important extrinsic stabilizer of the distal radioulnar joint (DRUJ). The floor of the ECU tendon sheath is also an important stabilizer of the TFCC, which provides intrinsic stability to the DRUJ. 1 Due to specific anatomical features, the ECU tendon is vulnerable to trauma from direct blows, excessive stretching, or repetitive overuse. In addition, because it is an important stabilizer of the TFCC, both structures are prone to injury. Allende and Le Viet 2 reported that TFCC injury or degenerative tear was present in 11 of every 27 ECU lesions patient. Thus, accurate diagnosis and proper, timely treatment is essential. ECU tendinosis can coexist with other conditions in the ulnar side of the wrist, so the diagnosis must not be considered as an exclusion of all other possible diagnoses. A full clinical and radiological assessment of the other important ulnar side wrist structures is necessary to exclude coexistent pathologies in the TFCC, lunotriquetral ligament (LT), DRUJ, or ulnar styloid. This is because optimal results can only be obtained when the co-existing pathologies are treated simultaneously. 3 Ultrasound (US) and/or magnetic resonance imaging (MRI) are the imaging modalities of choice for the diagnosis of ECU tendinopathy and instability.4,5 However, some authors have shown that MRI findings may not be accurate in trauma patients, especially those with suspected carpal instability, due to post-traumatic changes.6,7 Wrist arthroscopy is the gold standard diagnostic tool for diagnosis of carpal instability including TFCC lesions. 8 For patients with recalcitrant symptoms of ECU tendinopathy, sixth dorsal compartment release should be considered. 9 In order to improve diagnostic accuracy, we performed wrist arthroscopy on patients when they received surgical treatment for ECU tendinopathy. We report on the findings from wrist arthroscopy and the results of treatment. The findings highlight the importance of wrist arthroscopy.
Material and methods
Patients
Demography of the patients.

aFovea+: Fovea tenderness; DRUJ+: Distal radioulnar joint instability; ECU+: Extensor carpi ulnaris instability.
bMRI: Magnetic resonance imaging; TFCC: Triangular fibrocartilage complex.
cA/S: Arthroscopic synovectomy; USO: Ulnar shortening osteotomy*.
Plain radiographs including anteroposterior, lateral, and both oblique views of the wrist were performed in all cases. MRI scans were performed obtained from all patients. The patients were diagnosed with ECU tenosynovitis, and six of the seven were diagnosed with degenerative triangular TFCC changes with intra-articular lesion. Diagnostic wrist arthroscopy and arthroscopic synovectomy of the radiocarpal joint were performed in all patients before the incision for ECU tendinopathy was made. During arthroscopy, the TFCC lesions were classified according to the Palmer system. 10
Surgical technique
All procedures were carried out under general anesthesia or regional block, with tourniquet control. The patient lay in a supine position with the affected arm on a hand table. Before exploration for ECU, diagnostic arthroscopy and synovectomy of the radiocarpal (RC) joint were performed. The operated arm was placed in a wrist traction tower and vertical traction with a force of 4–6 kg was applied through plastic finger trap devices to the middle three fingers for joint distraction. An arm tourniquet was applied.
Demography of the patients.
aTFCC: Triangular fibrocartilage complex; L-T: Lunotriquetral ligament; ECU: Extensor carpi ulnaris.
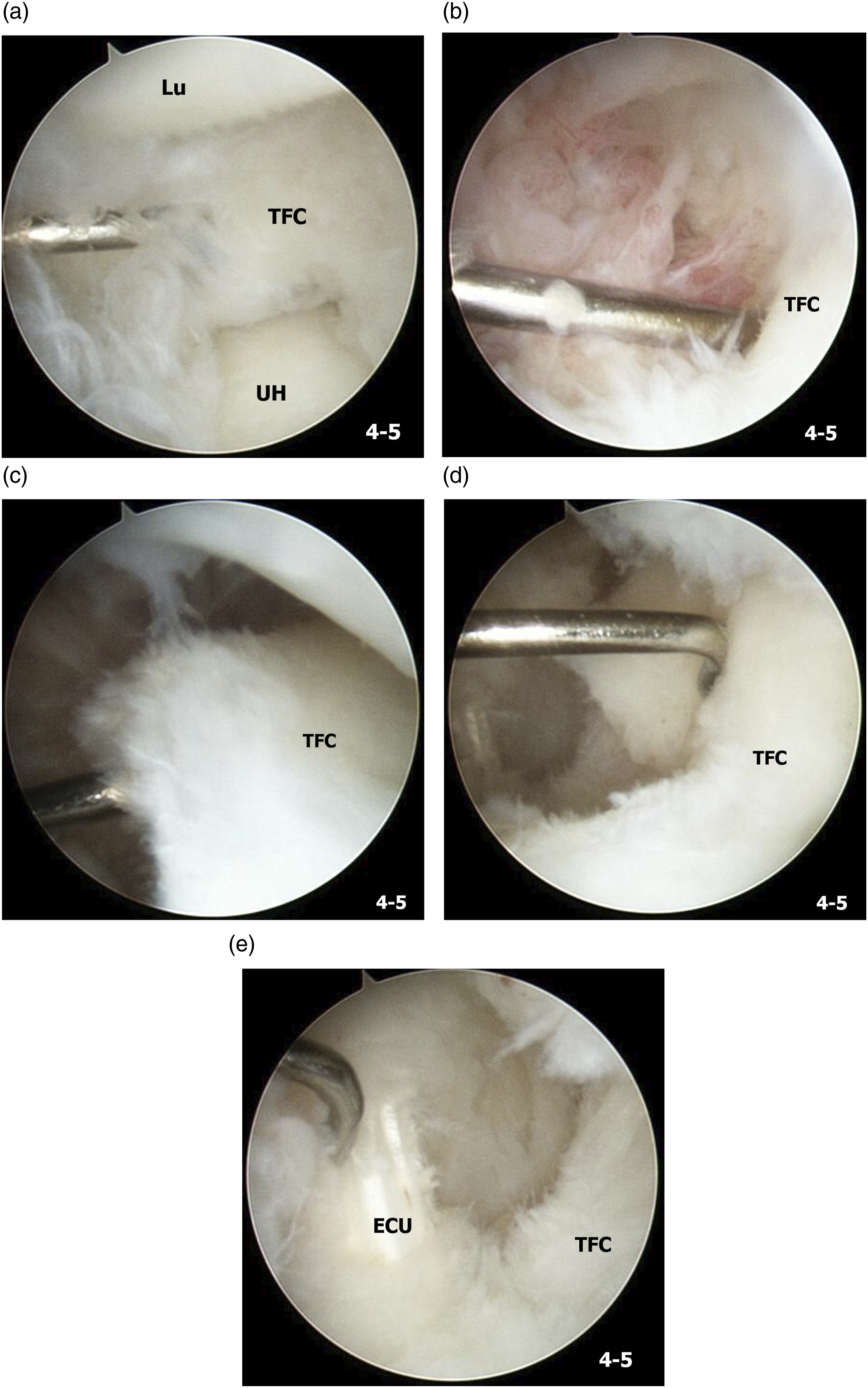
Case 5, A 64-year-old female patient with Lt. ECU tendinopathy. Lt. wrist ulno-carpal arthroscopy images. (a) Signs of a central perforation and degenerative changes along the perforation margin of the TFCC. (b) Signs of synovitis at the fovea. (c) Positive hook test. (d) A massive tear in the TFCC including the periphery and the fovea after synovectomy and debridement. (e) A partially ruptured ECU tendon after synovectomy and debridement (UH, ulnar head; TFC, triangular fibrocartilage; Lu, lunate; ECU, extensor carpi ulnaris).
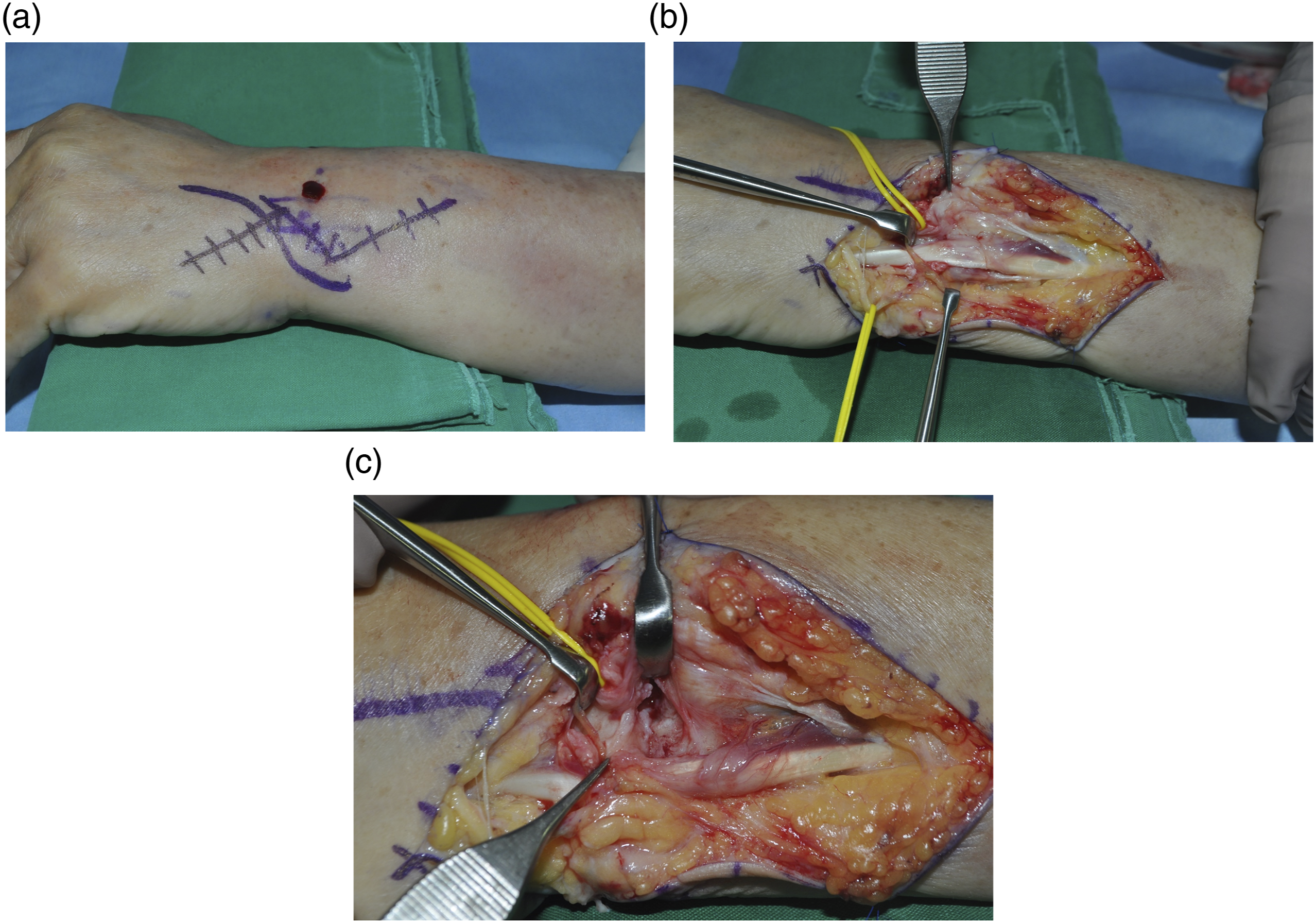
Intraoperative photographs of the same patient showing (a) the zig-zag incision along the ECU tendon; (b) the ECU tendon after division of retinaculum and fibro-osseous dorsal sheath using stair-step incisions; and (c) a ruptured osteofibrous sheath after retraction of the ECU tendon on the ulnar side.

An intraoperative photograph illustrating repair of the TFCC fovea with a microsuture anchor.
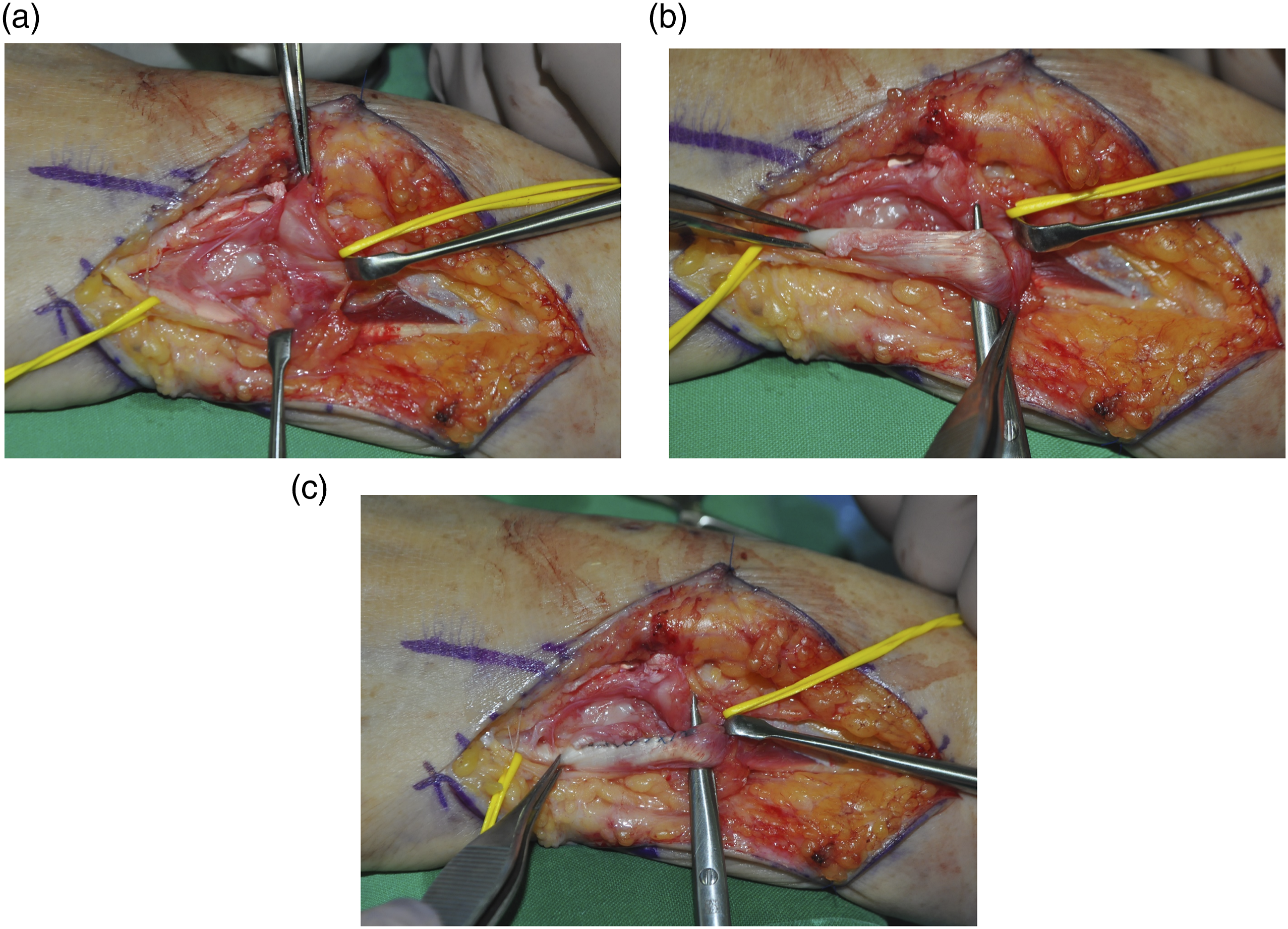
Intraoperative photographs showing (a) osteofibrous sheath repair using a microsuture anchor, (b) partial rupture of the ECU tendon, and (c) ECU tendon repair after debridement.
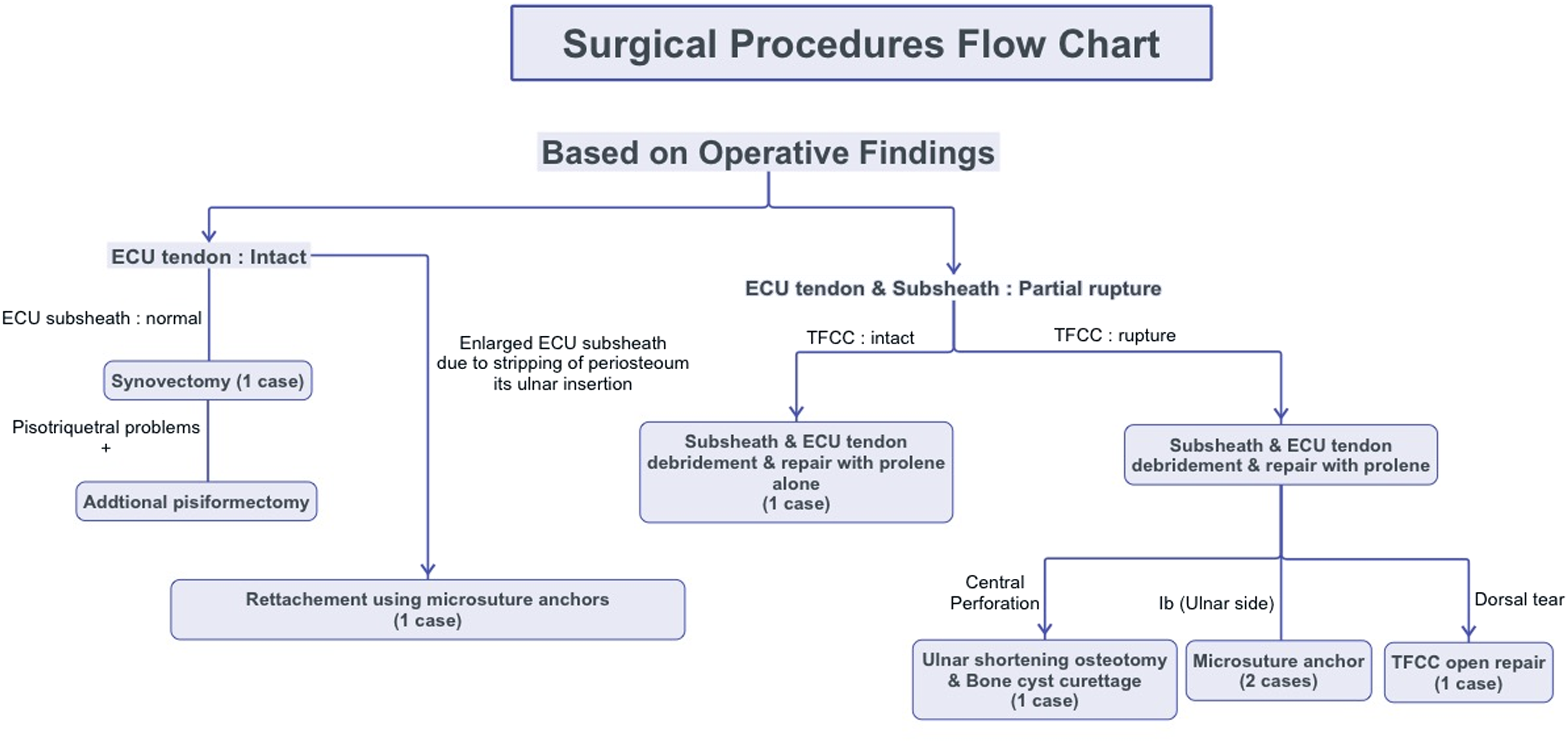
Flow chart of surgical procedures based on the operative findings.
Postoperative management varied according to the surgical procedure that was performed. The wrist was immobilized with a sugar tong splint for 2 weeks, after which a short arm cast was applied for 4 weeks in cases without a TFCC rupture. The short arm cast was applied for 6 weeks in cases where the TFCC had been repaired.
Clinical evaluation
Demography of the patients.

aVAS: Visual analog scale; pre/last f/u: preoperative/last follow-up.
bMMWS: Modified mayo wrist score; E: excellent; G:good; F: fair; P: poor.
cDASH: Disabilities of the arm, shoulder, and hand.
Statistical analysis
IBM SPSS version 20.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. We used a paired t-test to compare the preoperative and follow-up ROM, grip strength, VAS for pain, modified Mayo wrist score and quick DASH score. p values <.05 were considered statically significant. 13
Results
We identified TFCC injuries in four patients, two of which were classified as type 1B, one as a dorsal tear that was not described in the Palmer classification, and one as a type 2C injury (Table 2). After a mean follow-up period of 39 months (range, 25–49 months), all patients returned to their previous activities. The average VAS score decreased from 6.4 (range, 4–9) preoperatively to 1 (range, 0–3) at the final follow-up (p .000). The mean ROM of the wrist improved to 192° (97.6% of that of the normal side), compared to a preoperative ROM of 173° (84.9% of that of the normal side) (p = .039). The mean grip strength improved from an average of 21.4 kg (74% of that of the normal side) preoperatively to 22.6 kg (88.6% of that of the normal side) at the last follow-up (p = .143). Clinically, the patients were evaluated using the quick DASH score and modified Mayo wrist score, which is a point system based on four categories: pain, functional status, motion, and grip strength. The average quick DASH score decreased from 42.5 preoperatively to 18.2 at the final follow-up (p = .007). The average modified Mayo wrist score increased from 48.6 preoperatively to 79.3 at the final follow-up (p = .011). According to this score, there were one excellent, three good, and three fair results at the final follow-up (Table 3).
Of the three patients who showed fair results, a 64-year-old female had no particular co-existing diseases. However, her ROM was 95% of the normal 180° and the grip strength was 18 kg (90% of the normal). In addition, she complained of mild pain after vigorous activities and was considered to have fair outcomes with a total score of 75 points. One of the patients, a 37-year-old female scored 20 points for the pain and functional status, and her grip strength was 18 kg (82% of normal), therefore, she scored of 15 points, and her total score was 70 points which was considered fair. During the final follow-up, lateral epicondylitis, wrist dorsum ganglion, and long finger trigger finger were found simultaneously in the same arm, and may have affected the results. Further, one of the patients, a 35-year-old female, scored 20 points for the pain and functional status. ROM was 206° (97% of normal) and the grip strength was 14 kg (70% of normal), therefore, she scored of 10 points. She was considered to have fair outcomes with a total score of 65 points. This patient was diagnosed with a ganglion in the DRUJ after the first surgery, followed by postoperative constant tingling sensation in the dermatome of ulnar nerve dorsal sensory branch; this may have affected the final results. Among the three patients who had received TFCC repair upon arthroscopic discovery of an injury, we found no DRUJ instability, and the VAS scores were zero in all patients at the final follow-up (Figure 6). Clinical photos taken 26 months postoperative, show excellent functional results.
Discussion
Anatomically, in full supination, ECU tendon is subject to maximal traction and exits the sixth compartment at an angle of 30°, resulting in a greater contribution to true wrist extension.4,14 Therefore, the amount of tension on the ECU subsheath and the retinaculum is greater during forearm supination with the wrist in flexion and ulnar deviation. 15 Understanding these anatomical features of the ECU tendon is very important when diagnosing ECU tendon pathology. The patients in this study also reported ulnar side pain during diagnosis, which was aggravated upon supination. It should be noted that the ECU subsheath is an integral constituent of the TFCC. Subsheath injury is usually associated with adjacent soft tissue disruption, most often of the triangular fibrocartilage (TFC). Four out of seven patients presented with TFCC damages of which three were repairable.
Melone and Nathan 16 reported that, because of the complex anatomy of the TFCC, disruption of the TFC proper, also termed the articular disk, seldom occurs as an isolated injury. Destabilizing injuries of the DRUJ characteristically disrupt not only the TFC but also the adjacent ECU subsheath and other critical soft tissues to a variable extent. In this series, 28 (67%) of the included 42 cases had associated injury to the ECU subsheath with subluxation of the ECU tendon. Allende and Le Viet 2 also described the concept of multicomponent injury of the TFCC. Although they did not undergo wrist arthroscopy, in their series of 28 wrist (27 patients) with ECU disruption, 11 patients (41%) demonstrated substantive concomitant injury, usually involving the TFC. Among them, two patients underwent ulnar shortening together with positive ulnar variance and TFCC was reinserted into the ulnar styloid in three patients. However, in four patients treatment was not intraoperatively significant, and two patients with central degeneration underwent TFCC debridement. Moreover, four patients had LT ligament tears necessitating—exploration, and suturing was performed in only one clinically significant patient. The findings of this clinical study also emphasized that restoration of ulnar wrist instability requires simultaneous repair of all the co-existing pathologies to achieve optimal clinical outcomes. Recognition of this variable, often extensive, spectrum of injury to the ulnar wrist is essential to optimal management of ECU subsheath disruption resulting in ECU tendon and DRUJ instability. Therefore, accurate diagnosis of ECU pathologies is required. Clinically, the use of selective local anesthetic injection can aid in diagnosis of ulnar wrist pain, given the myrid of differential diagnosis. 3 However, using local anesthetic injection at several sites for examination is not practically feasible in clinical practice. Furthermore, in patients with ECU tendinopathy, the tender point is close to the fovea. This can hinder accurate physical examination, and at the same time DRUJ instability test may be difficult to perform due to pain. In our experience, clinically differentiating the ECU tendon disease process from TFCC traumatic disruption accurately is challenging. In this study, TFCC was intact in two of the six patients with foveal tenderness and in one of the two patients with DRUJ instability. Moreover, two patients who underwent TFCC repair did not exhibit DRUJ instability on physical examination.
Radiologically, US and/or MRI are the radiologic imaging modalities of choice for the diagnosis of ECU tendinopathy and instability.4,5 MRI may demonstrate tenosynovitis, recurrent subluxation or dislocation, or either partial or complete rupture of the tendon. MRI also helps in the assessment of other structures in the ulnar side of the wrist, as it can be used to exclude coexistent pathologies in the TFCC, DRUJ, intercarpal ligament, and the ulnar styloid that are not readily visible on US images.4,17 However, some authors have found that MRI findings may not be accurate in trauma patients, especially in the investigation of suspected carpal instability, due to post-traumatic changes.6,7 Similarly, although we performed MRI on all patients, we could not obtain accurate information on the state of the TFCC. The results were consistent with the arthroscopic findings in only one patient who exhibited central perforation, but not with the arthroscopic findings in four patients who exhibited degenerative tear or degeneration at the periphery of the TFCC. Currently, wrist arthroscopy is the gold standard diagnostic tool for carpal instability including TFCC lesions. 8 Therefore, we strongly suggest that wrist arthroscopy should be carried out to ensure accurate diagnosis and treatment for all patients who undergo surgical treatment for ECU tendinopathy. This is because it is difficult to accurately differentiate between ECU tendinopathy and TFCC injury clinically, and MRI can only provide limited information on the state of the TFCC. Furthermore, the ECU subsheath and TFCC are anatomically closely related; therefore, injuries can occur simultaneously. Based on our experience, we suggest performing wrist arthroscopy for the accurate diagnosis and treatment for patients whose MRI findings suggest a degenerative tear or degeneration at the periphery of the TFCC.
ECU tendinopathy can be classified into tenosynovitis of the tendon sheath, tendinopathy and tendon instability. These conditions can occur in isolation or synchronously, and can develop gradually. The initial treatment is conservative.
For patients with recalcitrant symptoms, sixth dorsal compartment release should be considered. 9 Allende and Le Viet 2 reported that completely isolated ECU lesions are rare: of 36 patients, 22 were able to return to previous activities; seven experienced at least a 30% decrease in grip strength; five showed decreased ROM; and two required ECU tenolysis. In the current study, all seven patients were able to return to previous activities. They showed improvement in VAS, grip strength, quick DASH, and modified Mayo wrist score. However, during the final follow-up visit, three patients only had fair functional modified Mayo wrist score, but this was not related to the ulnar wrist pain.
When accompanied by a TFCC injury, concurrent repair of the TFC,2,16 has been reported as successful method of surgical repair. We were able to obtain good results through TFCC repair in three patients.
Our study has a number of limitations. First, it was an observational study of one procedure. Therefore, we could not evaluate the efficacy of our method in comparison with a group that had undergone surgical treatment without wrist arthroscopy. Second, the sample size was small, and each patient had several pathologies; therefore, we did not evaluate the results of each treatment. Third, the follow-up period was relatively short. Thus, studies with a longer follow-up period are needed to investigate disease progression in patients who have received arthroscopic debridement, ECU tendon repair, and ulnar shortening osteotomy.
Conclusion
The incidence of TFCC rupture associated with ECU tendinopathy is not precisely known. However, since the ECU subsheath is recognized as an integral part of the TFCC, TFCC injury is highly likely to occur with ECU tendinopathy. Therefore, when treating patients with ECU tendinopathy, the possibility of TFCC combined injury should always be considered. If surgical treatment is planned, we suggest a wrist arthroscopy for more accurate diagnosis an intra-articular pathology, particularly for patients whose MRI findings suggest a degenerative tear or degeneration at the periphery of the TFCC. Additionally, if ECU and DRUJ stability is obtained by repair or reconstruction of the concurrent pathologies in the ECU subsheath, TFCC and other intra-articular structures, the results will be favorable.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This paper was supported by Fund of Biomedical Research Institute, Jeonbuk National University Hospital (CUH2019-0034).
Ethical approval details
This study received approval from our institutional review board at Jeonbuk National University Hospital (CUH 2020-10-042).