
Abstract
Purpose
The aim of this study was to present to the literature a rare injury mechanism that causes knee dislocation (KD) and describe its characteristics.
Methods
A retrospective review of patients with KD who were treated between January 2014 and December 2019 at our hospital was performed. Patients with KD due to rotavator machine injury were included in Group 1 and all patients with KD due to other etiological reasons were included in Group 2. Patients’ age, gender, side, injury mechanism, time to surgery, length of stay (LOS), operation time, follow-up time, neurological injury status, vascular injury status, open injury status, and surgical interventions were evaluated.
Results
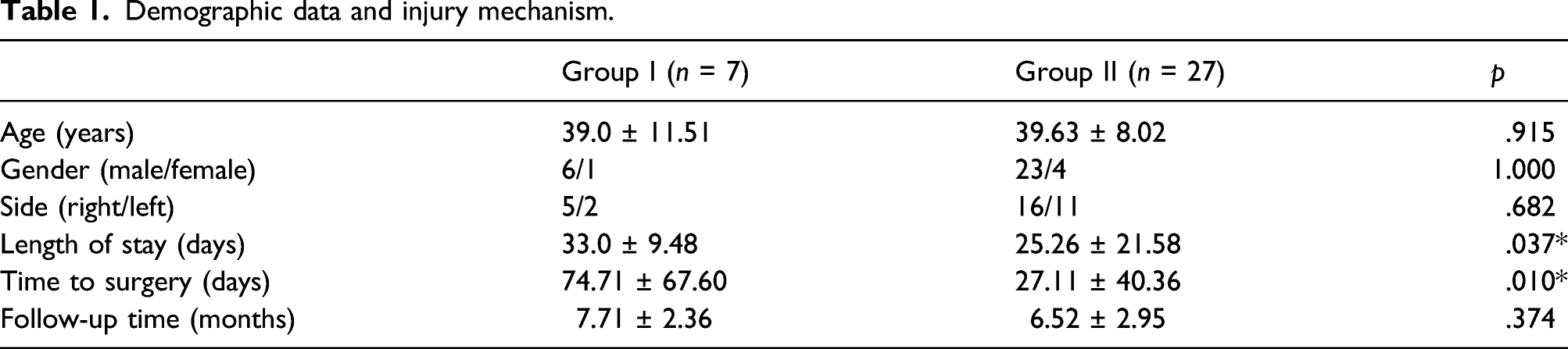
A total of 34 patients were evaluated in the study. There was no statistically significant difference between the groups in terms of age, gender, side, or follow-up time (p = .915, p = 1.000, p = .682, p = .374, respectively). However, LOS and time to surgery were statistically significantly longer in Group 1 (p = .037, p = .010, respectively). Moreover, neurovascular damage was statistically significantly more common in Group 1.
Conclusion
As a rare injury mechanism for KD, rotavator machine injuries cause more neurovascular injuries in patients compared to other injury mechanisms and increase the time to surgery and LOS due to preoperative soft tissue damage.
Introduction
Knee dislocations (KDs) are rare injuries and make up only 0.2% of all orthopedic trauma cases.1–5 However, KDs are potentially limb-threatening injuries.4,5
KDs usually occur because of high-energy trauma, the most common being motor vehicle accidents at a rate of more than 50%. Sports injuries (33%) and simple falls (12%), especially in obese patients, are other common etiological factors.6–8
The rotavator machine used by farmers to cultivate the soil causes KD injuries. In our literature review, we determined that this machine injury mechanism that causes KD has not been reported before.
The aim of this study was therefore to present to the literature this rare injury mechanism that causes KD and describe its characteristics.
Materials and methods
A retrospective review was made of the hospital’s electronic database to obtain details of patients with KD who were treated between January 2014 and December 2019 at our hospital. The study was approved by the institutional review board. All patients provided written informed consent before study participation.
Patients who were treated for KD in our clinic were included in the study. Patients who did not undergo surgical treatment or whose follow-up was incomplete after treatment were excluded from the study.
Patients with KD due to rotavator machine injury were included in Group 1, and all patients with KD due to other etiological reasons were included in Group 2. The rotavator machine, which has two arms, is controlled by hand, is used with push-and-pull movements, and works with circular movements on the part in contact with the ground. When patients using this machine lose control, their legs get caught on the machine and KD occurs as a result of rotational forces on the knee (Figure 1). It was determined that when the farmers realized that they had to press the button on the arm of the device to operate the rotavator machine, they disabled the control mechanism by continuously tapping the operating button. Thus, the security mechanism was disabled with this method applied by the farmers (Figure 2). When farmers using rotavator machines lose control, their legs get stuck on the machine (a) and KD occurs because of rotational forces in the knee (b). KD: knee dislocation. Farmers must press the button (a) on the handle of the device to operate the rotavator machine. It was determined that they deactivated the control mechanism by continuously tapping the operating button (b).

A detailed neurovascular examination was performed for all patients when they presented to the emergency department (ED). Emergency vascular repair was performed by cardiovascular surgery for patients with vascular damage. In the ED, an external fixator was applied first in two of these cases, and an above-the-knee splint was applied for the others first. After the external fixator was kept for 4 weeks and the splint for 3 weeks, the patients underwent surgical intervention. Posterior Cruciate Ligament (PCL), Medical Collateral Ligament (MCL), Lateral Collateral Ligament (LCL) posterolateral corner, and MCL reconstructions were performed with a pneumatic tourniquet under anesthesia, respectively. Anatomical ligament reconstructions were performed for all patients included in the study.
In the postoperative period, cefazolin sodium at 3 × 1g was administered to the patients for 24 h. Enoxaparin sodium at 4000 IU was administered subcutaneously for 3 weeks, with the first dose 12 h after surgery. The same rehabilitation program was applied to all patients. Passive knee flexion and extension were not restricted. Only foot contact was allowed on the injured side for 6 weeks. In the first 3 weeks, only isometric exercises were given, and then isometric exercises were given together with isokinetic exercises. A hinged knee brace was used for the first 3 months. A return to sports was allowed after 9 months.
Patients’ age, gender, side, injury mechanism, time to surgery, length of stay (LOS), operation time, follow-up time, neurological injury status, vascular injury status, open injury status, and surgical interventions were evaluated.
Statistical analysis
Statistical analyses were performed using SPSS 22.0 (IBM Corp., Armonk, NY, USA). As descriptive statistics for numerical variables, median and minimum-maximum values were determined. Since the number of samples per group was below 30, nonparametric test procedures were used. The Mann–Whitney U test as the nonparametric alternative to the independent two-sample t-test and KruskalWallis variance analysis as the nonparametric alternative to one-way analysis of variance were used to determine the relationships between parameters. The chi-square test was used in the analysis of categorical data. The results were evaluated within 95% confidence intervals and p < .05 was considered significant.
Results
Demographic data and injury mechanism.
Neurovascular status.

A temporary external fixator was applied for one patient in Group 1 and one patient in Group 2. A ligament reconstruction surgery procedure was applied for all patients included in the study.
Discussion
In the current study, we have identified a rare injury mechanism causing KD in our patients that has not been reported before: rotavator machine injury. This rare injury mechanism causes more neurovascular injuries in patients compared to other injury mechanisms and increases the time to surgery and LOS due to preoperative soft tissue damage.
Overall, KDs are more likely to be reported in younger patients.2,9,10 The mean age of our cohort was 39.5 ± 8.65 years.
The mechanism of injury for KDs could be divided into high-energy and low-energy dislocations.5,11,12 Motor vehicle injury was the most common mechanism of injury previously determined.2–5,13 The most important finding of the current study has been the demonstration of a rare mechanism of injury causing KD. Moreover, the type of injury that we have described has characteristics similar to high-energy injuries.
In the current study, neurological damage was found in 23.5% of patients with KD. In the previous literature, neurological injury was reported in 6.2–50% of cases.2,3,5,14,15 Previous authors agreed that the peroneal nerve is the most common site of neurological injury.1,5,15–17 In the current study, peroneal nerve damage was detected at a rate of 23.5%, and this is consistent with the previous literature. However, more neurological injury is seen with the rotavator machine injury mechanism.
The popliteal vessels are relatively fixed at the adductor hiatus and fascial arch of the soleus.5,17 The large displacement that occurs during KD can easily injure the tethered artery. 17 In previous studies, vascular injuries were reported at rates of 1.6–64% in patients with KD.2,3,9,10,14,18–21 Vascular injury was found in 14.7% of patients in the current study. The rate of vascular injury among cases of the rotavator machine injury mechanism was also found to be higher than the rate among other patients in the current study.
Open dislocation and vascular injuries were associated with higher rates of amputation in the previous literature.2,14,22 Amputation rates have been reported to range from 2.5% to 9.2% in previous publications on patients with KDs.2,14,23,24 In the current study, the amputation rate was 0%.
We recommend that farmers working with rotavator machines wear trousers and shoes that protect against sharp tools. Moreover, farmers should be informed that tapping the power switch, which they see as a more practical way of using the rotavator machine, can cause knee injuries. Rotavator machine manufacturers should take extra precautions about these situations that cause knee injuries and detailed information about this issue should be provided in user manuals.
The limitations of this study are the use of data obtained from retrospective screening and the fact that it was conducted at a single center. However, its strengths are that the study was carried out at a Level 1 trauma center and that it demonstrates a rare mechanism of injury causing KD.
Conclusion
In this study, rotavator machine injuries have been defined as a rare injury mechanism that causes KD. This mechanism causes more neurovascular injuries in patients compared to other injury mechanisms and increases the time to surgery and LOS due to preoperative soft tissue damage. It should be kept in mind that patients affected by this rotavator machine injury mechanism that causes KD may have more challenges in treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.