
Abstract
Background
The coronavirus disease 2019 (COVID-19) pandemic has affected people in various ways, including restricting their mobility and depriving them of exercise opportunities. Such circumstances can trigger locomotor deterioration and impairment, which is known as locomotive syndrome. The purpose of this study was to investigate the incidence of locomotive syndrome in the pandemic and to identify its risk factors.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic, which began in early 2020, has affected people in a variety ways 1 and living environments have been transformed significantly. 2 In order to prevent the spread of COVID-19 and to help medical institutions cope with the increasing number of seriously ill people, governments were forced to lock-down cities and/or severely restrict people from leaving their homes. 3 Companies have rapidly progressed the digital transformation of their work and actively adopted telework to minimize employees’ movements. In addition, many patients with musculoskeletal disorders have been hesitant to visit hospital due to anxiety about infections and to prevent the spread of infection. Restrictions on movement, reduced opportunities for exercise, and delays in treatment during the COVID-19 pandemic may have triggered worsening of musculoskeletal disease and deterioration of locomotor function in the community.
Locomotive syndrome is a condition proposed by the Japanese Orthopaedic Association (JOA) in 2011 that refers to the decline in mobility due to musculoskeletal disorders. 4 In patients with locomotive syndrome, social participation and activities of daily living are often limited, and as the condition progresses, they may have difficulty in living independently and thus require nursing care. The JOA has developed a self-checklist called a loco-check, which makes it easy for people to know if they have locomotive syndrome. Although the prevalence of locomotive syndrome may be increasing due to the circumstances surrounding COVID-19, no study has yet investigated the occurrence of locomotive syndrome during the pandemic. The purpose of this study was to investigate the prevalence of locomotive syndrome pre- and intra-pandemic among patients who visited an orthopedic outpatient clinic, and to investigate the new incidence of locomotive syndrome during the COVID-19 disaster. Furthermore, we identify risk factors for the onset of locomotive syndrome in patients who developed it during the pandemic.
Materials and methods
Timing of the survey
This large-scale multicenter questionnaire survey was conducted between 1 November 2020 and 31 December 2020 in Osaka, Japan. At the time of the survey, Japanese people had already experienced the first and second waves of the COVID-19 pandemic, and in April, when the first wave occurred, the government declared a state of emergency and severely restricted people from going out. This survey period marked the beginning of the third wave, and 1 week later, the government declared a second state of emergency, requiring people to stay at home.
Study design
This research has been approved by the IRB of the authors’ affiliated institutions. All patients who visited four private orthopedic clinics for any symptoms during the surveillance period were asked to participate in this survey. Those who provided informed consent were enrolled and could withdraw freely if they wished during and after completing the questionnaire. The enrolled participants had an appointment in the clinic and were visiting the clinic for the first time or for a return visit to the clinic.
Questionnaires
The participants were asked to answer the questionnaire about their general information, symptoms, exercise habits, and locomotive syndrome. The questions about symptoms include where the region of the patient’s complaint (spine, shoulder/hand, hip/knee joint, or other) and how the symptoms have changed compared to before the pandemic (deteriorated, stable, stable, or newly occurring). They were also asked whether they had refrained from visiting the hospital during the pandemic. We asked them about changes in their exercise habits (stable, increased, decreased, and no exercise habit) before and after the pandemic. Participants were asked to complete the loco-check, a self-administered checklist developed by the JOA 4 to detect locomotive syndrome, at two time points: pre- and intra-pandemic (current).
Diagnosis of locomotive syndrome
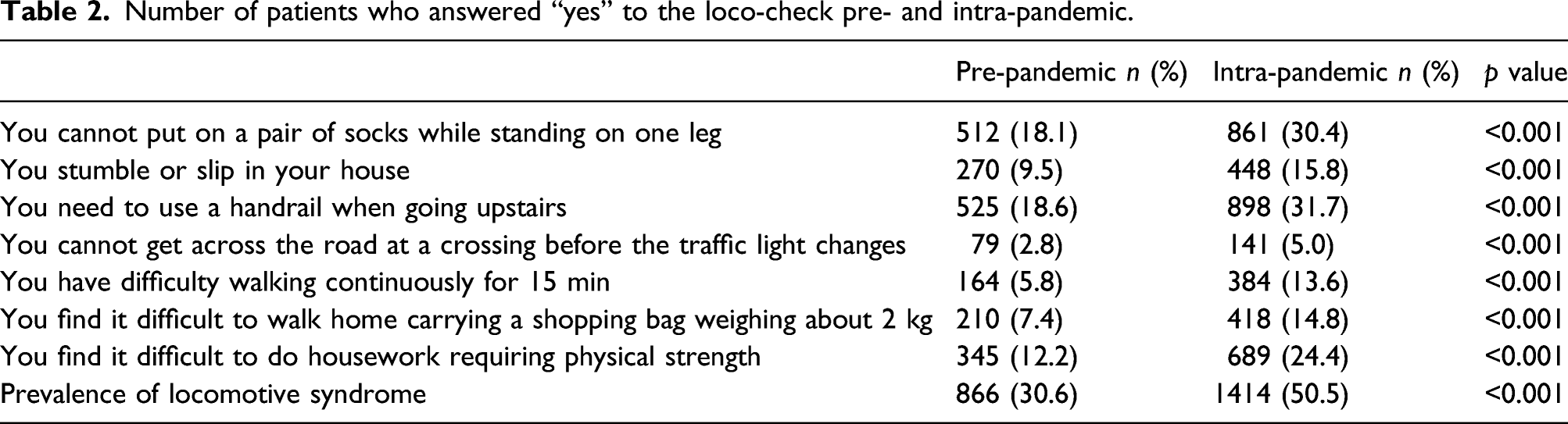
Diagnosis of locomotive syndrome was based on the responses to the loco-check. The loco-check is assessed based on the following seven statements: (1) You cannot put on a pair of socks while standing on one leg; (2) You stumble or slip in your house; (3) You need to use a handrail when going up stairs; (4) You cannot get across the road at a crossing before the traffic light changes; (5) You have difficulty walking continuously for 15 min; (6) You find it difficult to walk home carrying a shopping bag weighing about 2 kg; and (7) You find it difficult to do housework requiring physical strength. Those who respond positively to any of the above categories may possibly have locomotive syndrome. Several studies have verified the usefulness of the loco-check to detect early-stage locomotive syndrome.5,6 The participants who met one or more of the above categories were considered to have locomotive syndrome in this study.
Statistical analysis
Based on their responses to the loco-check, patients were diagnosed with locomotive syndrome pre- and/or intra-pandemic. Patients without any symptoms of locomotive syndrome pre- and intra-pandemic were defined as the Normal-Normal group, while patients who had newly developed locomotive syndrome during the pandemic were defined as the Normal-Locomo group. We compared demographics, and changes in symptoms and exercise habits between pre- and intra-pandemic in the two groups. Furthermore, a multiple logistic regression analysis was used to investigate the risk factors for developing locomotive syndrome during the pandemic. Responses to the loco-check in the Normal-Locomo group were compared by each complaint. The student t-test was used to compare continuous variables, and the χ-square test was used to compare categorical variables. In the multiple logistic regression analysis, “shoulder/hand” was used as a reference to calculate adjusted odds ratios (aOR) for complaints, and “stabile” was used for changes in symptoms and exercise habits. Statistical tests were conducted with a two-sided 5% significance level. All analyses were performed using R (http://www.r-project.org).
Results
Characteristics of all patients.

Number of patients who answered “yes” to the loco-check pre- and intra-pandemic.
Univariate comparison between normal-normal and normal-locomo group.

Locomo: locomotive syndrome.
Multivariate logistic regression analysis for associated factors with the development of locomotive syndrome.

Responses to the loco-check for Normal-Locomo group according to complaints.

Discussion
This is the first study to investigate the association between the COVID-19 pandemic and locomotive syndrome. The pandemic not only put people at risk of infection, but also imposed restrictions on going out and moving around, deprived them of opportunities for exercise, and caused some to refrain from visiting hospitals. This situation can lead to deterioration of a disease and the locomotor system, thus causing locomotive syndrome, especially in patients with musculoskeletal disorders. The prevalence of locomotive syndrome in Japan has been reported to be 34–40%,7,8 while in this study, it was 30.6% before the pandemic and increased to 50% after the pandemic. Furthermore, 30% of those who had no symptoms of locomotive syndrome had developed it. Locomotive syndrome is a major cause of being bedridden and need for nursing care, resulting in a shortened healthy lifespan. During the chaos of a pandemic, controlling COVID-19 infection is of course a top priority; however, preventing motor impairment and dysfunction is also of importance.
One of the risk factors for the development of locomotive syndrome during the pandemic was deteriorating or new onset of symptoms of musculoskeletal disorders. Since the treatment of musculoskeletal diseases is often not urgent, many elective surgeries were canceled or postponed during the period of infection spread. 9 Some patients were hesitant to go to the clinic, including 37% of all patients in our study, although this was not associated with the development of locomotive syndrome. In addition to these factors, the psychological stress caused by the COVID-19 pandemic may have contributed to the acceleration of chronic pain. 10 Among musculoskeletal disorders, spine and hip/knee joint symptoms were significant risk factors for the development of locomotive syndrome. Patients with spinal problems often had difficulty in walking, climbing stairs, and putting on socks while standing on one leg, while the most patients with hip/knee complaints had difficulty in climbing stairs.
Reduced or no exercise habit was also an independent risk factor for developing locomotive syndrome. Due to the implementation of strategies to control the COVID-19 infection, training gyms, gymnasiums, and other exercise facilities were closed in many countries, depriving people of exercise opportunities. Voluntarily refraining from going out and the popularization of telework have also reduced the amount of activity in daily life, with some reports showing a 40% decrease in the number of steps taken compared to before the pandemic. 11 Regular exercise is a vital management strategy for addressing chronic pain and musculoskeletal disorders.12,13 Furthermore, since exercise can affect systemic diseases such as diabetes 14 and hypertension, 15 as well as mental health 16 and immune functions, 17 many concerns have been raised about lack of exercise during a pandemic. 18 Ensuring daily exercise may be an extremely effective treatment for maintaining health in a pandemic such as the COVID-19 pandemic. 19
More than a year has passed since humanity’s battle with COVID-19 began, and vaccination programs have started, and eventually we will overcome COVID-19 in the near future. However, social distancing and restrictions on going out are expected to continue for the foreseeable future. Furthermore, patients infected with COVID-19 are at risk for more severe motor impairment. 20 In addition to the loss of physical activity due to hospitalization or isolation at home, the infection itself can cause damage to the muscle through excessive production of proinflammatory cytokines in hypercatabolic conditions. 21 Thus, it is necessary to develop a treatment strategy for locomotive syndrome compatible with the COVID-19 era. As controlling musculoskeletal symptoms and ensuring exercise habits are important to prevent it, the solution may be remote rehabilitation and telemedicine. 22 Bhuva reported that 97% of patients were satisfied with receiving spine physical medicine and rehabilitation via telemedicine during the COVID-19 shutdown. 23 In addition, home fitness has increased in popularity because of convenience and safety, and this trend looks to be the new normal for the foreseeable future. 24
This study had several limitations. First, this study may contain a recall bias. Because the survey was conducted after the pandemic occurred, responses prior to the pandemic would have been retrospective. It is also possible that negative emotions including fear and anger associated with COVID-19 may have influenced the results. Second, this study only included patients who visited an outpatient spine clinic, and it is unclear whether the results can be applied to the general population. However, patients with musculoskeletal diseases are at higher risk of developing locomotive syndrome, and it may be worthwhile focusing on them rather than the general population. Third, this study did not include patients with COVID-19. The effect of the viral infection itself on the locomotor system has not been examined, and further studies are needed to investigate this issue. Finally, the diagnosis of locomotive syndrome was based on the loco-check alone. Though locomotive syndrome is generally diagnosed using two physical examinations and a 25-question survey, this requires more time and communication, which may not be feasible during a global pandemic. However, previous studies have proven that the loco-check is useful in identifying early locomotive syndrome, and therefore, we believe that this study provides insights into patients with early locomotive syndrome. Despite these limitations, this study still represents a valuable investigation with a relatively large sample size into the trends in locomotive syndrome during a pandemic.
Conclusions
This large-scale multicenter cross-sectional study demonstrated that the prevalence of locomotive syndrome in outpatients with musculoskeletal disorders increased significantly after the COVID-19 pandemic. In addition, among the patients with no symptoms of locomotive syndrome, 30% developed it in the wake of the pandemic. In addition to older age, deteriorated or newly developed symptoms of musculoskeletal diseases, especially complaints about the spine or hip/knee joints, were independent risk factors for the development of locomotive syndrome. Furthermore, decreased or no exercise habit was associated with developing locomotive syndrome. To prevent people from becoming bedridden and requiring nursing care, it is crucial to treat musculoskeletal disorders and ensure adequate exercise habits, even during a global pandemic such as the COVID-19 pandemic.
Footnotes
Acknowledgments
We sincerely appreciate all persons who participated in the current survey at Shimada Hospital, Ishikiri Hospital, Shiraniwa Hospital, and Nishinomiya-Watanabe Hospital.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approvals
The study protocol was approved by the Institutional Review Board of our institution (Osaka City University: No. R02996). All information has been handled in accordance with the standards for privacy of individually identifiable health information of health insurance portability and accountability act in Japan.