
Abstract
Purpose
We describe a novel technique that uses an aiming drill guide and ankle arthroscopy for direct visualization and reduction of the depressed articular surface located between the posterior tibia and the fractured posterior malleolus. This technique requires less soft tissue dissection to visualize and reduce the depressed articular surface.
Methods
Between June 2014 and May 2019, 126 patients were surgically treated for trimalleolar fractures. Among them, 11 had depressed articular fragment between the posterior tibia and the fractured posterior malleolus reduced using our novel technique. The study included six men and five women, with a mean age of 46.5 (range: 23–62) years.
Results
In eight (73%) cases, the articular surface was reduced, with the articular surface step-off being less than 2 mm, as noted on postoperative computed tomography (CT). Syndesmosis congruity within an anterior-to-posterior difference of less than 2 mm was confirmed in nine (82%) cases via postoperative CT. The mean 100-mm visual analog scale (VAS) and the mean Olerud-Molander ankle score at the final follow-up were 16.6 ± 14.5 and 87.7 ± 7.5, respectively.
Conclusions
The depressed articular fragment located between the posterior tibia and the fractured posterior malleolus can be treated using an aiming drill guide and ankle arthroscopy. Ankle arthroscopy is used for direct visualization of the depressed articular surface, and the aiming drill guide can guide the bone plunger precisely to the depressed articular surface for reduction. This technique requires less soft tissue dissection than conventional techniques to visualize and reduce the depressed articular surface.
Introduction
Posterior malleolar fractures involving the weight-bearing articular surface can be associated with depressed articular fragments between the posterior tibia and the fractured posterior malleolus, which are sometimes difficult to approach and reduce unless the fractured posterior malleolus is opened (Figure 1).1–6 When the large osteochondral fragment is not reduced, it may block anatomic reduction and prevent the restoration of normal joint relationship and stability.
6
Weber
6
described a method to reduce osteochondral fragments that are proximally dislocated and impacted between the posterior tibia and the fractured posterior malleolus. Through the posterolateral approach, the main fractured posterior malleolar fragment was elevated and opened to reduce the impacted osteochondral fragments using a bone plunger. However, this technique required a wide incision and extensive soft tissue dissection. Unless the joint was opened, the articular surface and fracture reduction would not have been visualized. We developed a technique using ankle arthroscopy for direct visualization and an aiming drill guide for reduction of the depressed articular surface. The ball tip of the aiming guide was placed at the depressed articular surface under arthroscopic visualization. A bone plunger was then inserted into a cannula connected to the guide and pushed downward to reduce the depressed surface. The aiming drill guide could guide the bone plunger precisely to the depressed articular surface where the ball tip of the device was located. The purpose of this study was to evaluate the clinical and radiologic outcomes of posterior malleolar fractures associated with a depressed articular surface that was treated by the aforementioned technique using an aiming drill guide and ankle arthroscopy. (a, b) Preoperative radiographs show posterior malleolar fracture. (c) Computed tomography (CT) scan shows depressed articular surface between the posterior tibia and the fractured posterior malleolus (arrow).
Materials and methods
Subjects
This study was a retrospective case series. Between June 2014 and May 2019, 126 patients were surgically treated for trimalleolar fractures. Among them, 11 had a depressed articular surface between the posterior tibia and the fractured posterior malleolus reduced using our novel technique. The study included six men and five women, with a mean age of 46.5 (range: 23–62) years. Approval from the appropriate institutional review board was obtained, as well as informed consent from all patients.
Indication for using the present technique was the posterior malleolar fracture associated with a depressed articular fragment of at least 10 mm in diameter and more than 2 mm of depression located between the posterior tibia and the fractured posterior malleolus. The depressed fragment should not be rotated or inverted when observed via computed tomography (CT) (Figure 2). Computed tomography scans were routinely taken preoperatively to identify the exact size, location, and orientation of the fracture fragment. Small osteochondral fragments that were rotated and displaced were difficult to reduce using our technique. Small osteochondral fragments that were blocking the reduction of the posterior malleolar fracture were pushed downward into the joint using the aforementioned technique and removed using an arthroscopic grasper. (a) CT scan shows the depressed articular fragment (black arrow), which was approached through the lateral malleolar fracture gap (dotted arrow). (b) The lateral malleolar fracture was widened for the approach by displacing the distal fragment posteriorly (white arrow). PF = proximal fragment, DF = distal fragment, PT = peroneal tendon.
Operative technique
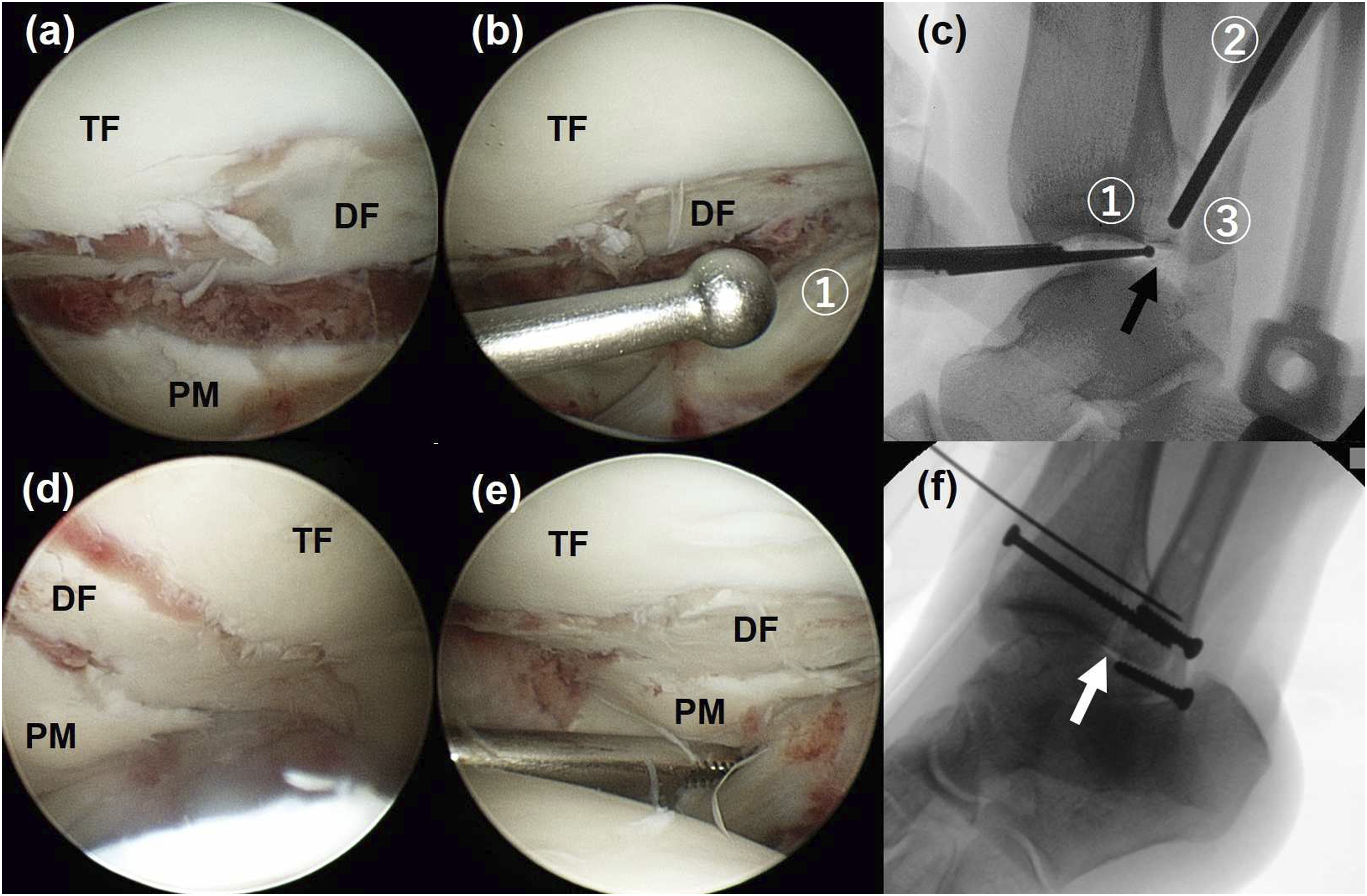
Patients were placed in the lateral decubitus position with a thigh tourniquet. An arthroscope was inserted into the ankle joint to visualize and assess the fracture and remove hematoma or debris inside the ankle joint. A posterolateral skin incision was made on the lateral malleolus to allow for conversion to an open approach for the posterior malleolus if reduction using the closed technique was inadequate. The lateral malleolar fracture was exposed and widened to approach the depressed articular surface by displacing the distal fragment posteriorly (Figure 2).7,8 A freer dissector was inserted through the lateral malleolar fracture into the posterior malleolar fracture and used as a lever to further widen the fracture gap for the approach. An aiming drill guide was positioned at the ankle joint with the ball tip inserted through the anterolateral arthroscopic portal. The bone ejector was inserted into the cannula connected to the device, through the lateral malleolar fracture and into the posterior malleolar fracture (Figures 3 and 4). Connecting joints of the aiming drill guide were first set loose to ease the insertion. Under arthroscopic visualization, the ball tip was positioned at the depressed articular surface (Figure 5). After fastening the connecting joints of the device, a bone ejector was inserted into the cannula connected to the device and guided toward the depressed fragment. The bone ejector was further pushed downward to reduce the depressed surface under arthroscopic visualization (Figure 5). When the ball tip was held firm at the depressed fragment, the device could guide the bone ejector to the fragment at any angle. We set the insertion angle of the bone ejector as vertical as possible to the fragment to ease reduction. However, when reduction was not satisfactory, the joints of the device were loosened and adjusted while holding the ball tip at the fragment. As long as the bone ejector was connected to the device, it could target the fragment at different angle for better reduction. The reduced fragment was temporarily fixed with K-wires. The posterior malleolar fracture was then reduced using ligamentotaxis through the intact posteroinferior tibiofibular ligament (PITFL) after anatomic reduction of the lateral malleolar fracture.
9
A percutaneous reduction and screw fixation technique was used (Figure 6). When the depressed articular fragment could not be approached through the lateral malleolar fracture, it was directly approached through the posterior malleolar fracture using the posterolateral approach between the peroneus brevis and the flexor hallucis muscles. Instead of opening the posterior malleolar fracture fragment as described by Weber,
6
the aiming guide was applied and the bone ejector was inserted into the posterior malleolar fracture. Under arthroscopic visualization, the bone ejector was pushed downward to reduce the fragment. When the posterior malleolar fracture was extended to the medial malleolus and the depressed articular fragment was located between the posterior tibia and the posteromedial fragment, the depressed articular fragment was approached from the posteromedial fracture. The ball tip connected to the aiming guide was inserted through the anteromedial arthroscopic portal and the bone ejector was inserted into the posteromedial fracture from the medial side. Small rotated fragments within the fracture gap that could not be reduced by the present technique were pushed downward into the joint by the bone ejector and removed using an arthroscopic grasper (Figure 7). Postoperatively, the patients were restricted from weight-bearing for 6 weeks in a posterior splint. When a syndesmotic screw was fixed for syndesmotic injury, weight-bearing was delayed for 8–10 weeks. The syndesmotic screw was removed at 10–12 postoperative weeks. An aiming drill guide, which was developed to guide the K-wire to the precise position toward the ball tip ① for multiple drilling or retrograde drilling for osteochondral lesions of the talus, was prepared. A large cannula ② was connected to the device and a bone ejector ③ from a bone biopsy set, which corresponds to the cannula, was inserted. The distal tip of the bone ejector ③ could be guided toward the ball tip ①. An aiming drill guide was positioned at the ankle with the ball tip inserted through the anterolateral portal and the bone ejector inserted through the lateral malleolar fracture and into the posterior malleolar fracture. Connecting joints were first set loose to ease insertion. An arthroscope was inserted through the anteromedial portal to view the depressed osteochondral fragment. (a) Arthroscopic images show the posterior malleolar (PM) fracture and the depressed fragment (DF). (b) The ball tip ① was inserted through the anterolateral portal and positioned at the depressed articular surface. (c) A fluoroscopic image shows the ball tip ① positioned at the depressed articular surface (black arrow). A bone ejector ③ was inserted into the cannula ② and guided toward the depressed fragment. The bone ejector was pushed further downward to reduce the depressed fragment under arthroscopic view. (d, e) Arthroscopic images show the reduced depressed articular surface and the posterior malleolus. (f) A fluoroscopic image shows anatomic reduction of the depressed fragment (white arrow) and the posterior malleolus. TF = tibia fragment, DF = depressed fragment, PM = posterior malleolus. Simple radiographs (a, c) and computed tomography scans (b, d) show anatomic reduction of the depressed fragment and the posterior malleolus. (a) A simple radiograph and (b, c) computed tomography (CT) scans show a displaced posterior malleolus fracture with a small fragment (white circle) between the tibia and the posterior malleolus, blocking the closure of the fracture gap. The aiming drill guide was applied, and the bone ejector was inserted through the fibular fracture (dotted arrow) and pushed downward to plunge the fragment into the ankle joint. The fragment was removed using an arthroscopic grasper. (d, e, f) A simple radiograph and CT scans show closure of the fracture gap with reduction of the posterior malleolus.



Postoperative Assessment
The quality of fracture reduction was assessed using postoperative CT scans obtained at 12 months postoperatively. The joint congruity was assessed on sagittal images. Articular depression less than 2 mm was considered acceptable. Syndesmosis congruity was assessed on axial images at the tibial plafond. An anterior-to-posterior difference of less than 2 mm was considered acceptable. 10 At the final follow-up, standard weight-bearing radiographs of both ankles were obtained. Radiologic parameters (tibiofibular clear space, tibiofibular overlap, and medial clear space) between the affected ankle and the contralateral uninjured ankle were compared. The tibiofibular clear space was defined as the distance between the lateral border of the posterior malleolus and the lateral border of the lateral malleolus on lines parallel to and 10 mm above the tibial plafond. The tibiofibular overlap was defined as the distance between the anterolateral border of the distal tibia and the medial border of the lateral malleolus 10 mm above the tibial plafond. The medial clear space was defined as the distance between the medial border of the talus and the lateral border of the medial malleolus on lines parallel to and 5 mm below the talar dome. 11 The radiologic parameters were measured by a single orthopedic surgeon blinded to the study details. Clinical outcome scores were assessed using the 100-mm visual analog scale (VAS) and Olerud-Molander ankle scores (OMAS).12,13 The 100-mm VAS is a validated self-assessment tool for evaluating pain after fracture. 13 The 100-point nine-category OMAS is a validated scoring system that includes aspects of the outcome that are considered useful: pain, stiffness, swelling, stair climbing, running, jumping, squatting, use of supports and ability to work, and activities of daily living. 12 Patients were followed up for a minimum of 1 year at regular intervals and invited for a final follow-up office visit for the study. For patients who could not visit the clinic for a final follow-up evaluation, the clinical and radiologic outcomes assessed at 1 year postoperatively were considered as the final outcome.
Data normality was assessed using the Shapiro–Wilk test. The Wilcoxon signed rank test was used to compare the radiologic parameters between the affected and contralateral uninjured ankles using the SPSS version 21.0 (SPSS, SPSS Inc., Chicago, IL, USA). Statistical significance was defined at the 5% (p < .05) level.
Results
Details and results for the 11 patients.

Preop = preoperative, Postop = postoperative, FU = follow-up, VAS = visual analog scale, OMAS = Olerud-Molander ankle score, M = male, F = female, SER = supination-external rotation, PER = pronation-external rotation, TF = transfibular, PL = posterolateral, PM = posteromedial.
aLauge-Hansen classification.
bPosterior malleolar fracture was classified as type I (posterolateral-oblique fracture), type II (medial-extension fracture), and type III (small-shell fracture). 14
cApproach to the depressed articular fragment.
dValues were measured on sagittal images of the computed tomography scans.
Postoperative radiologic outcomes.

Values are given as mean ± standard deviation.
Discussion
Incongruity of the joint surface after ankle fracture can cause morbidity and lead to ankle arthrosis. 12 The decreased articular surface area secondary to fracture can lead to increased peak stresses and alter joint biomechanics.16,17 As the posterior malleolus plays an important role in load transfer between the distal tibia and the talar dome as well as in posterior stability, most surgeons agree on reduction and internal fixation of posterior malleolar fracture involving more than 25% of the distal tibial articular surface.16–21 However, the posterior malleolar fracture is sometimes associated with a depressed articular fragment between the posterior tibia and the fractured posterior malleolus, which is difficult to approach and reduce.2,4–6 Accurate intraoperative evaluation of the joint surface using fluoroscopic radiographs may sometimes be limited because of the overlap between the posterior malleolus and the lateral malleolus on lateral radiographs.16,22,23 The use of intraoperative cone-beam CT can significantly improve intraoperative assessment of the fractured fragment and joint surface.24–26 However, not every operation room is equipped with this system.
Arthroscopy can offer direct visualization of the articular surface and greater precision for anatomic reduction of the depressed articular surface.1,2,27
Ankle arthroscopy has been introduced to directly visualize the tibial plafond articular surface during posterior malleolar fracture fixation.28–30 The benefits of arthroscopy-assisted fracture reduction include the possibility of not only direct visualization of the articular surface without extensive dissection but also evaluation of the entire cartilage and debridement of the damaged cartilage or removal of free fragments inside the joint.1,2,31 The application of arthroscopy for treating certain articular fractures, such as tibial plateau or humeral glenoid fractures, has made it possible to decrease the risk of joint stiffness and complications associated with the open surgical approach.32–35 Arthroscopy may offer the advantages of reduced pain and a more rapid, complete, and functional recovery.35–40
Another benefit of arthroscopy-assisted fracture surgery is that a targeting device can be used to approach the depressed fragment and elevate and reduce the depressed articular surface.33–35 In an arthroscopy-assisted tibial plateau fracture surgery, an anterior cruciate ligament (ACL) tunnel guide developed to target the footprint of ACL was applied to approach the depressed fragment. 33 Under arthroscopic guidance, the targeting tip was placed at the center of the depressed articular surface, a tunnel was created underneath the depressed articular surface, and a bone plunger was pushed through the tunnel to elevate the depressed fragment.33–35 A similar technique was applied to reduce the depressed articular surface associated with posterior malleolar fracture in the present study. The difference was that instead of making a bone tunnel to approach the depressed fragment, we used the fracture gap to approach the fragment. Using this technique, the fractured posterior malleolus and the posterior ankle joint did not need to be opened to approach the depressed articular fragment, which would have increased soft tissue dissection. We believe that a more accurate reduction of the depressed articular surface is possible with direct visualization under arthroscopy compared to using only intraoperative fluoroscopy. However, this could not be confirmed without a comparative study.
There are limitations to this technique. The use of arthroscopy and the aiming drill guide during fracture reduction may be technically demanding. The surgeon performing the procedure should be experienced at ankle arthroscopy. There may be times when the bone plunger may not advance smoothly through the posterior malleolar fracture and may need to be drilled through the fracture gap to approach the depressed articular fragment. When the fragment is rotated or inverted, it would be difficult to reduce the fragment only by pushing the fragment downward. However, rotated or inverted fragments are usually smaller ones that could be removed. The present technique is best indicated for depressed articular fragments of a substantial size. Small fragments were removed using arthroscopy and large fragments that were rotated or inverted were reduced by open technique as previously described. 6
The main limitations of this study were the small number of subjects, short follow-up period, absence of a comparative group, and lack of power analysis. However, the indication for this technique, that is, posterior malleolar fracture associated with a depressed articular fragment of a substantial size, is not often encountered, making this limitation inevitable. Furthermore, without a comparative analysis, it cannot be concluded if the use of this approach improved the clinical outcome compared with the conventional approach. Although we cannot recommend the procedure as a preferred method for reduction and fixation of depressed articular surface of the posterior malleolar fracture, the outcomes of the procedure in this study are encouraging. A further study with a larger population and a comparative group may further confirm these findings
Conclusion
Posterior malleolar fractures associated with depressed articular fragments between the posterior tibia and the posterior malleolar fracture can be treated using an aiming drill guide and ankle arthroscopy. Ankle arthroscopy is used for direct visualization of the depressed articular surface, and the aiming drill guide could guide the bone plunger exactly to the depressed articular surface for reduction. This technique requires less soft tissue dissection than conventional techniques to visualize and reduce the depressed articular surface.
Footnotes
Declaration of conflicting of interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics,consent and permissions
This study was approved by Hallym University Kangnam Sacred Heart Hospital Institutional Review Board (IRB number: 2017-11-009). Informed consent was received from all the patients of this study.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.