
Abstract
Introduction
Compound soft tissue defects of the skin and tendons of the dorsum of the hand, caused by open hand injuries, are common in clinical practice due to the thinness of the dorsal skin and the superficial position of the extensor tendons. 1 In the past, pedicled or free flap grafts were used for wound closure in the first stage, and tendon grafts or artificial tendon grafts were used for functional recovery in the second stage.2,3 However, these methods were associated with long hospitalization periods, more pain and indefinite efficacy. 4 Between January 2018 and January 2020, ten cases of skin and soft tissue defects of the digits accompanied by extensor tendon defects underwent surgical repair using dorsal digital cutaneous branch flap with partial extensor tendon at the same time. In addition, the donor site was repaired using a dorsal metacarpal artery relay flap. This study aimed to evaluate the clinical efficacy of this method.
Materials and methods
Patients
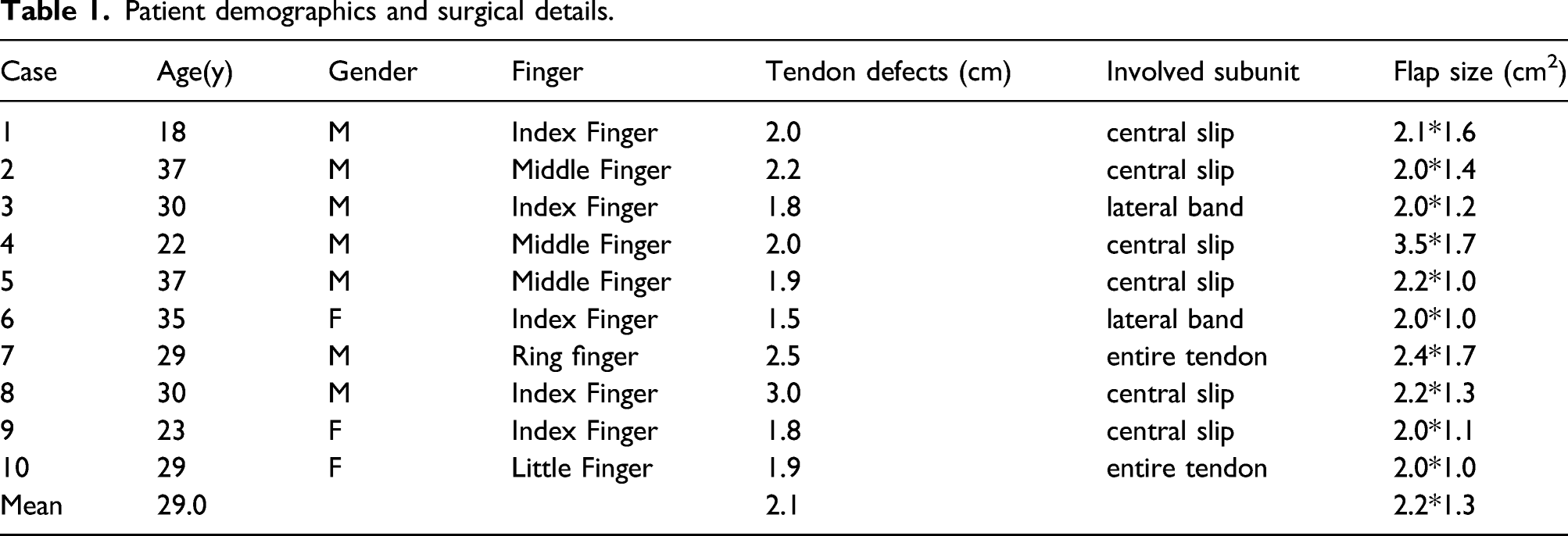
Patient demographics and surgical details.
After surgery, viability of flaps, presence of infection, and appearance of flaps were assessed. Flap sensation was measured using the static 2-point discrimination (2PD) test. The visual analogue scores (VAS) were used to evaluate aesthetic appearance of the recipient site. The Michigan Hand Outcome Questionnaire (MHOQ) score was used to evaluate the hand function. The finger range of motion (ROM) was measured by a goniometer. Cold intolerance of the flap was measured using the self-administered Cold Intolerance Severity Score questionnaire.
The clinical study was approved by the Ethical Committee of our institution, and all participants provided written informed consent after weighing the potential benefits and risks of the procedure.
Surgical procedure
Contraindications include patient’s preference to not preserve the functional ability of the finger, injury to the vascular pedicle, peripheral vascular disease, and life-threatening associated injuries. The operation was performed under brachial plexus block anaesthesia using a pneumatic tourniquet. First, the wound was thoroughly debrided. During surgery, the constant cutaneous branches of the digital artery with different diameters on the dorsal side were used based on the wound condition in the dorsal digit and extensor tendon defect. A point 5 mm from the proximal end of the wound was used as the point of rotation. The two edges did not exceed the two sides of the centre of the digit. The skin was incised layer by layer to reveal the superficial subcutaneous fascia layer, and the dorsal digital nerve was lifted. After exposing the superficial surface of the extensor aponeurosis, we usually choose the central slip under the flap, and the width of the central slip of the extensor tendon was about half the width of the central slip of the extensor tendon which could retain blood supply and with a length of approximately twice that of the tendon defect in the wound. The flap was lifted retrogradely from the proximal to the distal end. Fascia at the pedicle of the flap with a width of 0.5 cm or more was preserved. The free length of the pedicle was ensured so that the flap could rotate and cover the wound without tension. Care was taken to preserve the fascial tissue connecting the flap and tendon during the harvesting process. The tourniquet was loosened, and after flap blood flow was successfully re-established, the tendon was folded over and transplanted to repair the extensor tendon in the wound. The tension in the tendon was adjusted, and Kirschner wires were used for fixation of the distal interphalangeal joints. If residual nerves were found in the recipient site, the nerves in the flap were anastomosed with the cutaneous nerves in the recipient site with micro-sutures. Finally, the flap was moved to the recipient site and loosely sutured. If direct suturing of the donor site was not possible, a dorsal metacarpal artery relay flap was designed as previously described,
5
and the dorsal metacarpal artery flap donor site was directly sutured. (Figure 1(a)–(d)) In general, the flap can be designed from the distal 1/3 plane of the metacarpal bone to the distal 1/3 plane of the middle phalanx. Since the skin perforator chain of the dorsal cutaneous branch of the digital artery has a wide range of vascular communications, the flap can be designed according to the wound at any level of the axis. The length of tendon defect is usually less than or equal to the length of skin defect. Therefore, the tendon reconstruction length can be determined according to the flap design. (a) The compound tissue defects of the middle finger. (b) Blood supply to the tendon. (c) The tendon was transplanted to reconstruct the defect. (d) The defects and the donor site were resurfaced without tension. (e), (f) The shape and function of the affected sites recovered well by the time of follow-up.
Postoperatively, all patients were administered adequate dosage of intravenous antibiotics (broad-spectrum cephalosporin), subcutaneous heparin (4000 IU, once daily for 3–5 days), and analgesics (oral or intramuscular) if necessary. The involved forearms were immobilized postoperatively in a plaster back slab and remained in the extended position for a week. About 2 weeks after the wound healed, the stitches were removed and a dynamic splint was used, as the wrist joint was dorsiflexed about 30–40°, the active flexion and passive extension training was carried out under the protection of the braces. The Kirschner wires were removed after 3 weeks, and dynamic splint was removed after 4 weeks. After 6 weeks, an active straightening training was carried out. Resistance training was started at 8 weeks.
Of note, several surgical points would be highlighted. First, when cutting the dorsal finger flap, care should be taken to avoid the separation of the tendon from the flap to ensure that the tendon is connected to the deep fascia of the flap and it provides a good source of blood supply to the tendon. Second, after the dorsal digital flap carries the extensor tendon to cover the wound, tension in the tendon should be controlled when suturing to ensure that the resting position of the hand is close to normal. Third, when designing the dorsal palm flap, the pedicle should retain fascia that should be more than 0.5 cm in width, as well as the accompanying veins, which facilitate venous return in the flap. Fourth, after the skin flap is harvested, bleeding must be completely stopped to prevent bleeding under the skin flap and haematoma formation. After surgery, conventional anti-inflammatory, anticoagulant, and antispasmodic treatments should be administered, and blood flow in the flap should be observed. If there are regions of excessive tension, medication should be altered immediately, and if this is ineffective, the sutures should be cut and the wound re-sutured.
Results
The patients were followed up for 12–18 months, with an average of 15.4 months without of vascular insufficiency or venous congestion and donor site healing was achieved in all cases. In addition, donor site healing was achieved in all cases. No infectious complications occurred. All the flaps displayed warmth; good texture and contour matching; and pink colour 3 weeks after surgery. After flap repair, the digits had satisfactory shape and appearance and soft texture. The phalangeal joints exhibited good movement (Figure 1(e) and (f)).
Follow-up outcomes.

2PD, 2-point discrimination; MHOQ, Michigan Hand Outcome Questionnaire; ROM, range of motion MCP, metacarpophalangeal joint; PIP, proximal interphalangeal joint; DIP, distal interphalangeal joint; TAM, total active motion; RTW, return-to-work; VAS, visual analogue scores; CI, cold intolerance.
Discussion
The soft tissue of the dorsal digits is thin and susceptible to soft tissue defects accompanied with extensor tendon defects. 6 Regarding repairing these defects, functional repair and reconstruction of the extensor tendons should be considered. Many surgical procedures for tendon reconstruction are available in the clinical setting, including direct tendon repair; tendon transplantation; tendon transfer; and soft tissue reconstruction with local and free flaps.7,8 Selecting the best reconstruction plan based on the precise nature of patient’s hand defect is essential. In the past, flap transplantation was used to repair wounds in the first stage, while palmaris longus tendon transplantation was used to reconstruct extensor tendon function in the second stage. 9 Although this procedure has shown good clinical efficacy, staged avascular tendon transplantation has a higher rate of tendon adhesion and longer rehabilitation period. Currently, compound tissue flap transplantation is recommended, and a number of other surgical procedures have been reported.10,11 The compound-free dorsal digital tissue flap is a complicated operation, and recipient and donor sites are not in the same surgical region, which could increase the requirements for surgical teams and involve many disadvantages such as donor-site morbidity. 11 Several studies reported composite tissue flaps, consisting of a vascularized extensor indicts tendon and bone within distally based dorsal metacarpal artery can be used to repair composite tissue defects in a single stage. And it provides us a novel idea. 12 Although this flap is not suitable for defects of the dorsal finger reconstruction, it provides us a novel way of repair.
In the present study, dorsal digital cutaneous branch flap with partial extensor tendon was used to repair compound tissue defects, which solved the problems of skin coverage and tendon reconstruction at the same time. Shape of the skin flap was similar to that of the recipient site, and blood supply of the tendon was preserved as much as possible, thereby providing an anatomical basis for functional recovery.
There are many advantages of this procedure. First, the dorsum of the hand has several blood vessels, good skin texture, and moderate thickness. Therefore, this could assist in making flaps anatomically easy to harvest and classifying it as a perforator flap that does not damage the principal blood vessels of the digits. Second, the dorsal palmar nerve, extensor tendon, and other components can be used in a variety of tissue transplants, with a large harvesting range and flexible design. This way, problems of skin coverage and tendon defects are solved at the same time in a single stage. In addition, blood supply of the transplanted tendons is preserved as much as possible with relatively few postoperative adhesions, leading to better functional recovery. Third, texture, thickness, and colour of the flap are similar to these of the recipient site, giving it a good postoperative appearance. Finally, there is relatively little donor-site morbidity. Harvesting the extensor tendon has little effect on finger extension. Moreover, the donor site is covered by a dorsal metacarpal artery skin branch relay flap to avoid undesirable postoperative sequelae of skin grafts, such as contractures and hyperpigmentation. However, the potential disadvantages of this procedure are as follows: (i) two flaps need to be designed on the hand, which is more traumatic, and results in more obvious and linear scars and (ii) after rotating the flap pedicle, a small amount of the skin and soft tissue does not conform well.
In summary, dorsal digital cutaneous branch flap with partial extensor tendon can be used for simultaneous repair of skin and tendon defects. Appearance, sensation, and functional recovery of the flap were found to be satisfactory. The flap was simple in design and easy to harvest. This could be a safe and effective method for composite tissue defects of the dorsal digits.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
List of abbreviations
2-point discrimination (2PD); visual analogue scores (VAS); range of motion (ROM); Michigan Hand Outcome Questionnaire (MHOQ)