
Abstract
Keywords
Introduction
Chronic lateral ankle instability has been traditionally divided into mechanical ankle instability (MAI) and functional ankle instability (FAI). 1 Mechanical ankle instability, which is caused by the laxity or tear of the lateral ankle ligaments, generally needs ankle ligament repair or reconstructive surgery, and FAI is mainly treated by physiotherapeutic rehabilitation.2,3 Although the interactions between MAI and FAI and the relationships between the specific insufficiencies have not been completely clarified, a recent consensus in much of the published literature is that chronic lateral ankle instability is a multifaceted pathology caused by a combination of MAI and FAI.4–6
Residual FAI, regardless of the recovery of MAI after the lateral ligament repair or reconstruction procedure, is a risk factor for recurrent sprain.7,8 However, the importance of persistent postoperative evaluation of FAI is likely to be underestimated compared to the MAI. Except for subjective complaints of an unreliable ankle (giving way) by patients, the main components contributing to FAI, which include the impairment in neuromuscular control, deficit of dynamic muscle balance, deficit of postural control, insufficient proprioception, and strength deficits, can be evaluated objectively and quantitatively with instrumental tests.5,9–15
Although a few studies have reported improvement of FAI after the lateral ligament repair or reconstruction,11,12 there are few clinical reports identifying the period for the recovery of individual components contributing to FAI or the recovery rate compared to the unaffected ankle. Such information can help both physicians and patients to form more effective rehabilitation strategies following the operative treatments. We hypothesized that functional ankle stability may not be sufficiently restored, even after successful return to daily and sport activities following the repair of attenuated lateral ligaments. The purpose of this study was to identify the sequential changes of joint-position sense, peroneal strength, postural control, and functional performance ability after the modified Broström procedure (MBP) for chronic lateral ankle instability.
Materials and methods
Study subjects
Between August 2017 and November 2018, 56 patients (58 ankles) with chronic lateral ankle instability consecutively underwent the MBP using suture anchors. Among these, 48 patients (48 ankles) compatible with the inclusion and exclusion criteria were enrolled in the current study. Eventually, 46 patients (46 ankles) who could be followed up for 1 year postoperatively were analyzed (Figure 1). The reasons of loss to follow-up included one case of moving out to abroad and one case of femur fracture by traffic accident. Consort flowchart of the current study.
The inclusion criteria for the current study were as follows: (1) patients with subjective ankle instability including giving way (the regular occurrence of uncontrolled and unpredictable episodes of excessive inversion of the ankle), (2) patients with repeated sprain injuries for at least 6 months, (3) patients with marked ankle instability confirmed by the manual varus and anterior drawer stress test as compared to the contralateral ankle, (4) patients with at least 3 months of failed rehabilitation before surgery, (5) patients with less than 24 points based on the Cumberland Ankle Instability Tool,6,16 and (6) patients with scores below 90% on the daily living subscale and below 80% on the sports activity subscale of the Foot and Ankle Ability Measure 17 (FAAM). We selected the patients according to the standard inclusion criteria 6 by the International Ankle Consortium. The exclusion criteria were as follows: (1) patients with bilateral ankle instability, (2) patients with a previous surgical history involving lateral ankle ligaments, (3) patients with pathology of the peroneal tendons confirmed by magnetic resonance imaging (MRI), and (4) patients with generalized ligamentous laxity. The study protocol and investigation were conducted with Institutional Review Board approval (number 2017-05-016), and informed consent to participate was obtained.
The mean age of the patients was 31.6 ± 6.2 (range 20–45) years, and the mean duration of symptoms was 38.4 ± 15.5 (range 11–73) months. The current study included 27 male and 19 female patients. Thirty-five patients were participants in recreational sports activity more than twice a month. In addition, there were six heavy laborers and three high-demand athletes (two basketball and one soccer). The causes of initial injury included 25 cases of sports-associated injuries, 20 cases of slip and fall injuries during ambulation, and one case of traffic accident.
Rehabilitation protocol following the operation
All operations were performed by a single senior surgeon. The anatomical lateral ligament (anterior talofibular and calcaneofibular ligaments) repair was performed using two metallic suture anchors (CorkscrewTM, 3.5 mm in diameter; Arthrex, Naples, Florida, USA) and nonabsorbable suture (No. 2-0 Ethibond), and the inferior extensor retinaculum was imbricated. For 3 weeks postoperatively, cast immobilization and partial weight-bearing ambulation with crutches were prescribed. A range of motion (ROM) exercise consisting of ankle dorsiflexion and plantarflexion was encouraged following cast removal, and tolerable weight-bearing ambulation with walking boots were prescribed. Full weight-bearing ambulation without a brace was permitted from postoperative week 6, followed by circular ROM exercise including inversion and eversion. Thereafter, isometric and isotonic muscle strengthening exercises and proprioceptive balance training supervised by physical therapists twice a week were maintained for at least 6 weeks. Balance training progressed from static tandem standing (with eyes open and closed) to single-limb standing on an unstable surface (wobble board), and to dynamic balance training (single-leg standing with ball toss). Functional performance training included stationary bicycling, bilateral jumping, and slow-speed jogging. A return to exercise at the preinjury level was permitted after 3 months postoperatively.
Patient-reported functional outcome measure
Two validated self-assessed disability scales were used to evaluate the periodic changes of functional outcomes every 3 months. The Foot and Ankle Outcome Score 18 (FAOS) consists of 42 questions (five subscales) evaluating pain, other symptoms, activities of daily living, sports activities, and quality of life. The FAAM 17 is composed of 29 questions (two subscales) evaluating activities of daily living and sports activities.
Joint-position sense (proprioception) evaluation
The changes of joint-position sense were evaluated every 3 months using the continuous passive-motion mode of the Biodex-II isokinetic dynamometer (Biodex medical systems, Shirley, NY, USA) at 1°/sec angular velocity. The isokinetic device moved the ankle joint passively into the target position of 20° inversion and maintained a static position for 5 sec. Then the ankle joint was moved back passively to the neutral position. When the isokinetic device moved continuously from the neutral position to inversion at 1°/sec angular velocity, the patients were asked to reproduce the target angle of 20° inversion by stopping the device using a handheld on–off switch. To prevent the compensation by visual sense, all subjects used a blindfold during the test. Angular displacement was recorded as the error in degrees between the target angle and replicated angle. The average deficit ratio of joint-position sense compared to the unaffected side was analyzed and multiplied by 100 to give a percentage (%).
Peroneal strength evaluation
The eccentric peak torque normalized to body weight, total work, and deficit ratio were evaluated every 3 months using the Biodex-II isokinetic dynamometer at 60°/sec angular velocity. All measurements were performed under a consistent testing protocol, in the same position, and by the same examiner. Peak torque represented the maximal force applied at any time during five successive repetitions at 60°/sec angular velocity. Total work represented the average amount of force produced during repetitive motions. The average deficit ratio of peroneal strength compared to the unaffected side was analyzed and multiplied by 100 to give a percentage (%).
Postural control ability evaluation
Static postural control ability was evaluated every 3 months using the modified Romberg test 19 (one-leg stance test with eyes closed). All patients were asked to stand on one leg (barefoot) and remain as still as possible with arms outspread. An examiner measured the balance retention time before patients placed their non-stance limb on the ground when feeling unable to maintain this position. This test was repeated twice on each leg, and the measurements were averaged.
Functional performance ability evaluation
The functional performance test consisted of a one-leg hop test, a six-meter hop test, and a cross three-meter hop test. In the one-leg hop test, patients were asked to hop forward on one foot as far as possible, and the distance from the starting line was measured. Ability to maintain landing control without a loss of balance or touch of the contralateral foot was judged to be a successful hop. In the six-meter hop test, patients were asked to hop consecutively for a distance of 6 m as quickly as possible, and the time to complete the task was measured. In the cross three-meter hop test, patients were asked to perform cross-over hops consecutively on three meters of central line as quickly as possible, and the time to complete the task was measured. All tests were performed twice, and the measurements were averaged.
Statistical analysis
Data were presented as mean and standard deviation. The statistical analysis was performed using the SPSS program (version 20.0; SPSS Inc, Chicago, IL, USA), and p value ≤0.05 with a confidence interval of 95% was considered statistically significant. The Kolmogorov–Smirnov test was used to examine whether the data were normally distributed. We applied the Student t test for normal data and the Mann–Whitney test for nonnormal continuous data. Differences in all evaluations (joint-position sense, peroneal strength, postural control ability, and functional performance ability) for FAI between before and after operative treatment in the same individual were analyzed using the Wilcoxon signed-rank test. Side-to-side comparison with the unaffected ankle was done using the Mann–Whitney test. The changes of the patient-reported functional outcome measure (FAOS and FAAM) between preoperative and postoperative evaluation were analyzed with the Wilcoxon signed-rank test.
Results
The changes of functional outcome measure and complications
Functional outcomes evaluated with the FAOS and the FAAM (Wilcoxon signed-rank test, N = 46 ankles in 46 patients).

Abbreviation: FAAM, foot and ankle ability measure; FAOS, foot and ankle outcome score; PO, postoperative.
aComparison between preoperative and follow-up at 1 year postoperatively.
bDatas are represented as scores (mean ± standard deviation) changed on the basis of 100 points.
Complications included three wound problems (two with superficial infection and one with marginal necrosis). Two patients had skin irritation due to nonabsorbable suture material. One had a superficial peroneal nerve injury with temporary paresthesia. Although seven patients had a further sprain of the ankle within 1 year postoperatively; none had a recurrence of subjective and mechanical instability.
The changes of joint-position sense
Ankle joint-position sense (proprioceptive ability) evaluated with isokinetic dynamometer (N = 46 ankles in 46 patients).

Abbreviation: PO, postoperative.
aThe values are given as the mean and the standard deviation.
bSide-to-side comparison (Mann-Whitney test).
The changes of peroneal strength
Peroneal strength evaluated with isokinetic dynamometer (N = 46 ankles in 46 patients).
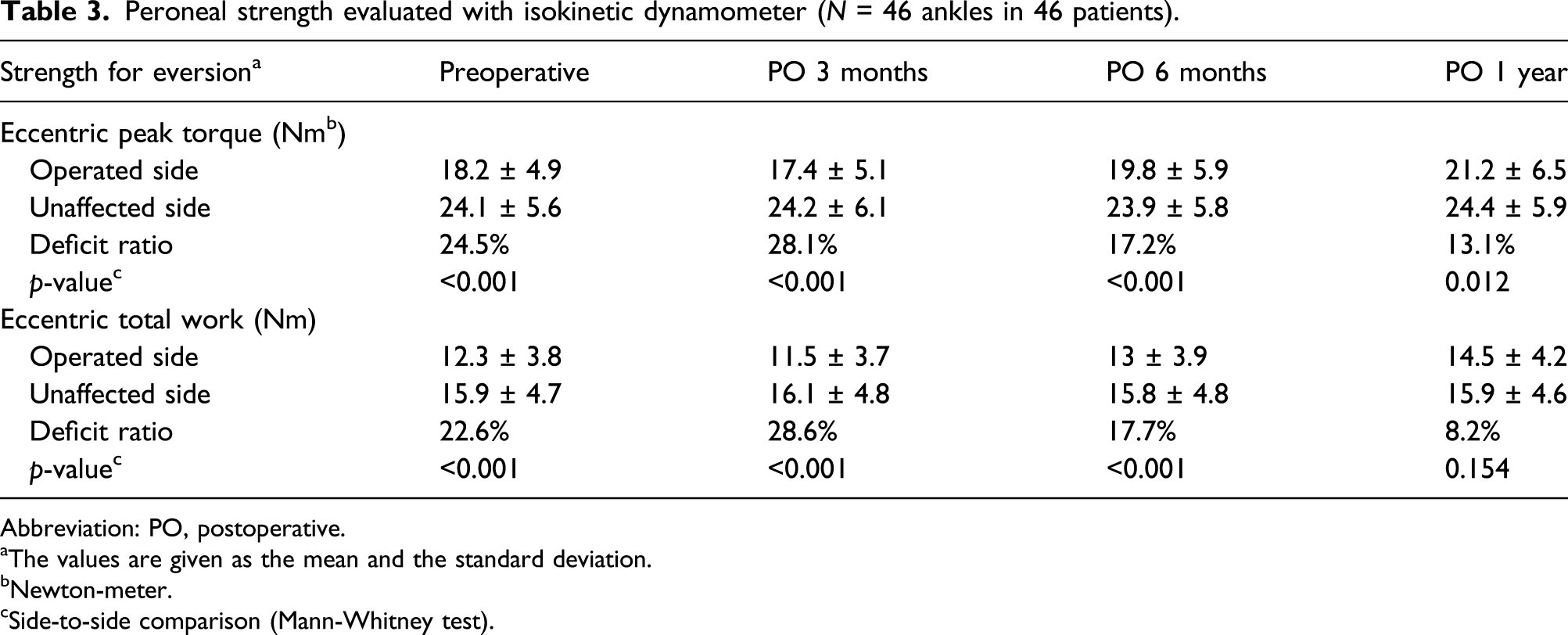
Abbreviation: PO, postoperative.
aThe values are given as the mean and the standard deviation.
bNewton-meter.
cSide-to-side comparison (Mann-Whitney test).
The changes of postural control ability
Postural control ability evaluated with the modified Romberg test (N = 46 ankles in 46 patients).

Abbreviation: PO, postoperative.
aThe values are given as the mean and the standard deviation.
bSide-to-side comparison (Mann–Whitney test).
The changes of functional performance ability
Evaluation of the functional performance ability (N = 46 ankles in 46 patients).

Abbreviation: PO, postoperative.
aThe values are given as the mean and the standard deviation.
bComparison between preoperative and follow-up at 1 year postoperatively (Wilcoxon signed-rank test).
Discussion
This prospective study reports the sequential changes of FAI in 46 patients who underwent the MBP for chronic lateral ankle instability. The most important finding of this study was that joint-position sense, peroneal strength, postural control, and functional performance ability were significantly improved after the MBP and supervised rehabilitation. However, the recovery ratio compared to the unaffected ankle was insufficient up to 1 year postoperatively with significant side-to-side differences, independently patient-reported functional outcomes in daily and sport activities.
As a primary anatomic repair procedure for chronic lateral ankle instability, the MBP has proven to provide acceptable long-term outcomes in conjunction with a low complication rate. 2 A longevity of mechanical ankle stability over a long-term follow-up has also been reported to be satisfactory, with a recurrence rate of 5–15%.7,20,21 Compared to many studies on recovery from MAI, comments reporting the changes of FAI after lateral ligament repair or reconstructive surgery are still insufficient. In addition, there are few clinical reports identifying the period to full recovery of individual components that contribute to FAI and the recovery rate compared to the unaffected ankle. In a study to document the effects of anatomical reconstruction of the anterolateral capsuloligamentous complex on proprioception, Halasi et al. 11 reported that the differences in joint-position sense evaluated with the slope-box test between the healthy and injured ankles disappeared as the result of surgery. They suggested that anatomical reconstruction contributes to improving decreased mechanoreceptor activity by retensioning attenuated lateral structures of the ankle joint. Chen et al. 4 also demonstrated that patients with the MAI suffered deficits in postural control, indicating that structural damage of the lateral ankle ligaments may produce a balance deficit. In a recent study to identify whether lateral ligaments reconstruction (MBP) could improve postural control ability in patients with MAI, Li et al. 12 reported that postural control ability assessed with single-limb postural sway tests was improved by reconstructing the lateral ankle ligaments. However, it was unclear whether a difference in postural control compared to the unaffected side disappeared postoperatively. For the effects of the MBP on peroneal strength, Cho et al. 22 reported that the deficit ratio (compared to the normal side) of peak torque for eversion significantly improved from a mean 38.6%–17.4%, and a significant side-to-side difference was found on the intermediate-term follow-up. These results were consistent with the findings from the current study.
In preoperative examination for patients with chronic lateral ankle instability, most physicians focus on evaluating MAI using a manual stress test and stress radiographs, evaluating the condition of the residual ligaments by using magnetic resonance imaging (MRI) or ultrasonography (USG), identifying concomitant intra-articular pathologies and malalignment of the ankle joint,23,24 and investigating the risk factors (generalized ligamentous laxity, severe obesity, failed previous surgery, long duration of ankle instability, high-demand work, and cavovarus deformity) associated with poor clinical outcomes.2,25,26 Evaluation of FAI tends to be relatively overlooked and mainly depends on a subjective complaint including giving way. Residual functional instability, regardless of a restoration of mechanical ankle stability, can be a risk factor for recurrent ankle instability after the MBP.7,8 Even after successful return to daily and sport activities, ongoing deficits in neuromuscular control may contribute to a higher risk of a recurrent injury. 27 Therefore, the precise pre- and postoperative evaluation of FAI is necessary to improve clinical outcomes and to prevent a recurrence of ankle instability. Except for subjective complaints of an unreliable ankle (giving way) by patients, individual components (impairment in neuromuscular control, deficits of dynamic muscle balance, deficits of postural control, insufficient proprioception, and peroneal weakness) contributing to FAI can be evaluated objectively and quantitatively with instrumental tests.5,9–15 The practical ways to evaluate FAI include the star excursion balance test,5,10 the single-limb postural sway test, 12 the modified Romberg test, 19 the slope-box test, 11 the isokinetic strength test, 22 the joint-position sense test, 28 and the patient-reported functional outcome measures.6,29 Because there is no definitive consensus on the best method to evaluate patients with FAI, we have attempted a global assessment of FAI through a combination of the clinically applicable examination tools.
The isokinetic dynamometer is frequently used to assess the muscle performance with the quantification of muscle strength.22,28 A recent critical review has reported that testing with this instrument is performed isokinetically (concentric or eccentric) at various angular velocities reflecting daily and sport activities. 3 In a preliminary test for the current study, many patients (especially most of the female patients) could not perform a task under 30°/sec angular velocity. In addition, peak torque and total work at 120°/sec angular velocity to represent light daily activities demonstrated no significant side-to-side difference in most patients. Based on these results in the preliminary test, we chose 60°/sec angular velocity as a standard protocol to measure the peroneal strength using an isokinetic dynamometer. Isokinetic dynamometer also can be used to evaluate the proprioception of the ankle joint. Proprioception contributes to both sensorimotor control and the muscle reflex to maintain dynamic stability. 30 The neural inputs provided by ankle mechanoreceptors, visual sense, and the vestibular organ are integrated in the central nervous system to generate a motor response. 31 Joint-position sense (proprioceptive ability) during ankle inversion movement is important for maintaining stability because most ankle sprains occur in the inversion direction. In the current study, a proprioception test using an isokinetic dynamometer was performed with the target position of 20° inversion because this target angle demonstrated more distinct errors in joint-position sense than the target position of 10° inversion as compared to the unaffected side. The validity of a functional examination using an isokinetic dynamometer has been proven to be reliable in many previous studies.3,13,30 Sekir et al. 30 reported that isokinetic inversion and eversion strength measurements represented good to high reliability with an intraclass correlation coefficient (ICC) between 0.82 and 0.98. Intraclass correlation coefficient for the proprioception test was reported to show high reliability (between 0.94 and 0.98).
The functional performance test has been reported to be a dynamic measure reflecting the various components, such as sensorimotor coordination, muscular strength, and postural control. 30 In the last stage of rehabilitation after operative treatment, this testing can be used as a criterion to decide on return to a preinjury level of activities. In the current study, the functional performance test consisted of a one-leg hop test, six-meter hop test, and cross three-meter hop test. All tests were performed at intervals of 3 months up to 1 year after operative treatment. This interval was considered to be appropriate to prevent both learning and fatigue effects on the reproducibility of the tests. Although continuous peroneal strengthening, proprioceptive training, and functional performance exercises were recommended, we could not be certain of individual compliance after 3 months of supervised rehabilitation. In addition, the use of a manual stop-watch might induce a measurement error that was not detectable by an examiner’s eye. We used a manual stop-watch to measure the balance retention time during the postural control ability test, and the time to complete a task during the functional performance test (six-meter hop test and cross three-meter hop test).
Interestingly, patient-reported functional outcome measures after the MBP showed no statistically significant correlation with individual components related to FAI. Like our finding in the current study, Sekir et al. 28 reported no correlation between the significant improvements in peroneal strength, proprioception, and functional performance after isokinetic exercise treatment for FAI. Cho et al. 22 reported that postoperative isokinetic strength of the peroneals demonstrated no statistically significant effects on the patient-reported functional outcome measures after the MBP. These results may indicate the need for more reliable and disease-specific outcome measures for chronic ankle instability. Brodsky et al. 32 reported a lack of sensitivity in the AOFAS ankle and hindfoot scores to evaluate the patients with chronic ankle instability. Based on significant side-to-side differences in various components of FAI after the MBP, continuous proprioception-oriented rehabilitation for more than 3 months may be needed for full recovery of functional ankle stability, independently of patient-reported functional outcomes in daily and sport activities. Further investigation on the long-term follow-up can help develop more effective rehabilitation strategies.
The present study has some limitations. First, this study included no evaluation of the dynamic postural control of the ankle. We used only the modified Romberg test (single-leg stance test with eyes closed) to evaluate the static postural control ability. Other instrumental tests (star excursion balance test, single-leg landing test, or postural sway test on a force platform) to analyze dynamic stability can help identify the effects of the MBP on postural control ability. Second, this study included only the patients who underwent the MBP using suture anchors. Although no clear difference in mechanical or functional ankle stability between the various ligament reattachment techniques of the MBP has been identified, the changes of joint-position sense, peroneal strength, postural control, and functional performance ability after the bone tunnel or arthroscopic technique may be different from the results of the current study.
Conclusion
The recovery ratio compared to the unaffected ankle was insufficient up to 1 year postoperatively although joint-position sense, peroneal strength, postural control, and functional performance ability were significantly improved after the MBP. This finding supports the need for continuous peroneal strengthening and proprioception-oriented rehabilitation after the MBP, independently of patient-reported functional outcomes in daily and sport activities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was granted by the Institutional Review Board.