
Abstract
Keywords
Introduction
Biplanar OWHTO (open-wedge high tibial osteotomy) is one of the most effective surgical procedures in the treatment of isolated medial compartment KOA (knee osteoarthritis) with varus. 1 Many favorable results for OWHTO have recently been reported.2–4 The main aim of OWHTO is redistribution of load from the medial compartment to the central and lateral areas by correcting the varus deformity of the knee.5,6 Thus, the pressure in medial compartment is decompressed, resulting in pain relieving and delaying of cartilage damage, even partial cartilage regeneration can be observed.7,8
Compared with other types of osteotomy surgery, OWHTO has absolute advantages, such as allowing subtle adjustment in the sagittal and coronal planes and avoiding compromising the peroneal nerve.9,10 However, some frequently reported problems associated with OWHTO are unintended increasing PTS (posterior tibial slope) and lowering PH (patellar height).11–13 Changes of the PH and PTS may result in patellofemoral osteoarthritis and ACL (anterior cruciate ligament) injuries due to increased retropatellar cartilage pressure and higher anteroposterior translation, respectively.14,15
Factors influencing PTS and PH in OWHTO are thought as follows: the amount of osteotomy opening, degree of knee flexion, ratio between anterior and posterior gap, status of the lateral hinge, and the severity of osteoarthritis present in the knee. Despite numerous studies analyze PH and PTS changes after OWHTO,1,2,16–18 only a few studies have briefly claimed effect of the amount of osteotomy opening on PTS and PH in OWHTO through cadaveric model.19,20 Also, data on PTS and PH changes and thus resulted clinical outcomes consequent on various osteotomy opening gap are rare.
To the best of our knowledge, there has been no comparative analysis of PH and PTS changes and knee function between different opening gap after OWHTO in clinic. Therefore, this study aimed to elucidate the influence of different amount of corrections on the changes of PTS, PH, and clinical outcomes in vivo after OWHTO for the first time. It was hypothesized that the amount of correction angle is a significant factor affecting the PTS and PH in OWHTO. With increased correction in the coronal plane, the likelihood of increasing the PTS and decreasing the PH increases.
Materials and methods
Between November 2015 to June 2019, 86 patients undergoing OWHTO were enrolled in this single-center, retrospective study. The study protocol was approved by the ethics committee of hospital institutional review board. The inclusion criteria were as follows: (1) patients with symptomatic varus medial joint OA, (2) range of motion <15° of flexion contracture, (3) varus aligned knee with >5° of mechanical tibiofemoral angle, and (4) medium-to-high level of activity. The exclusion criteria included the following: (1) lateral and patellofemoral compartments symptoms, (2) previous knee surgery, (3) anterior or posterior cruciate ligament insufficiency with intended slope correction, (4) the presence of rheumatoid arthritis or infectious arthritis, and (5) incomplete or insufficient radiographs.
Surgical procedure
All osteotomies were performed by one senior orthopedist (Y.R.Z.). Preoperative planning (correction angle and amount of opening gap) was determined as previously described by using the Fujisawa point and Miniaci method.21–23
An oblique skin incision was made from the insertion of the pes anserinus ascending posterocranially aiming at the posteromedial corner of the tibial head. After soft tissue dissection, the superficial portion of the medial collateral ligament was detached distally. A Hohmann retractor was inserted behind the tibial ridge to protect the neurovascular structure. With the leg fully extended, an exact AP view (one third of the fibular head is covered by tibia) of the knee joint was taken under fluoroscopy. Next, the horizontal osteotomy level was defined by two parallel K-wires, which aim toward the proximal tibiofibular joint, approximately 3.5 cm–4 cm below the medial joint line. The intraosseous lengths of two wires were measured, and the depth of the saw cut is 10 mm less than the value measured against the wires in order to leave a lateral bone hinge. It is important to ensure that there is sufficient space cranial for the locking bolts of the plate fixator. And, special attention should be paid to osteotomize the complete posterior cortex and to release posterior soft tissue in case of hinge fracture.
Afterward, with knee flexed to 90°, the anterior ascending osteotomy runs at an angle of 110° to the horizontal saw cut ending behind the patellar tendon insertion. This tuberosity segment should be at least 1.5 cm–2 cm wide. Using the three-chisel technique, the horizontal osteotomy was gradually opened to desired correction angle. 24
The medial tibia was fixed with TomoFix™ Medial High Tibial Plate (Synthes, Solothurn, Switzerland). To minimize tibial slope alteration, the spreader was placed as close to the posterior cortex as possible and the height of the anterior gap of the osteotomy was 60%–70%.25,26 The appropriate mechanical axis of the lower extremity was checked with a long alignment rod.
Radiographic and knee function assessments
Preoperative weight-bearing anteroposterior and lateral whole-leg radiographs were obtained to measure PTS and PH and to determine desired correction angle. Also, a skyline view of the knee was taken to evaluate the position changes of patella in coronal plane. The correction angle is defined as angle formed by two lines drawn from the center of the femoral head and tibiotalar joint to the 62.5% of the tibial width, respectively.
17
According to correction angle, patients were divided into three groups: LCA (large correction angle) group (>14°), MCA (medium correction angle) group (10°–14°), and SCA (small correction angle) group (<10°). PTS was defined as the narrow angle between the proximal tibial anatomic axis and the line tangent to the joint line (Figure 1). The Insall-Salvati index (the ratio between the length of the deep surface of the patellar tendon and the diagonal length of the patella, ISI) and the Blackburne-Peel index (the ratio between perpendicular distance from the inferior tip of patellar articular surface to proximal tibial articular surface and length of the patellar articular surface, BPI) were used to determine the patellar height.27,28 The pre-post difference of PTS, ISI, and BPI was calculated by subtracting the post-OWHTO value to the pre-OWHTO value in three groups, respectively. Furthermore, the preoperative, postoperative, and difference of PTS, ISI, and BPI values were analyzed according to the correction angle. Lateral radiographs obtained (A) preoperative and (B) at 36-month follow-up after OWHTO for medial gonarthrosis of the right knee in a 58-year-old female patient with correction angle of 20°. The PTS is the smaller of the two angles shown and is calculated as 90° minus the angle created by the proximal tibial anatomic axis and a line tangent to the joint line (medial tibial plateau).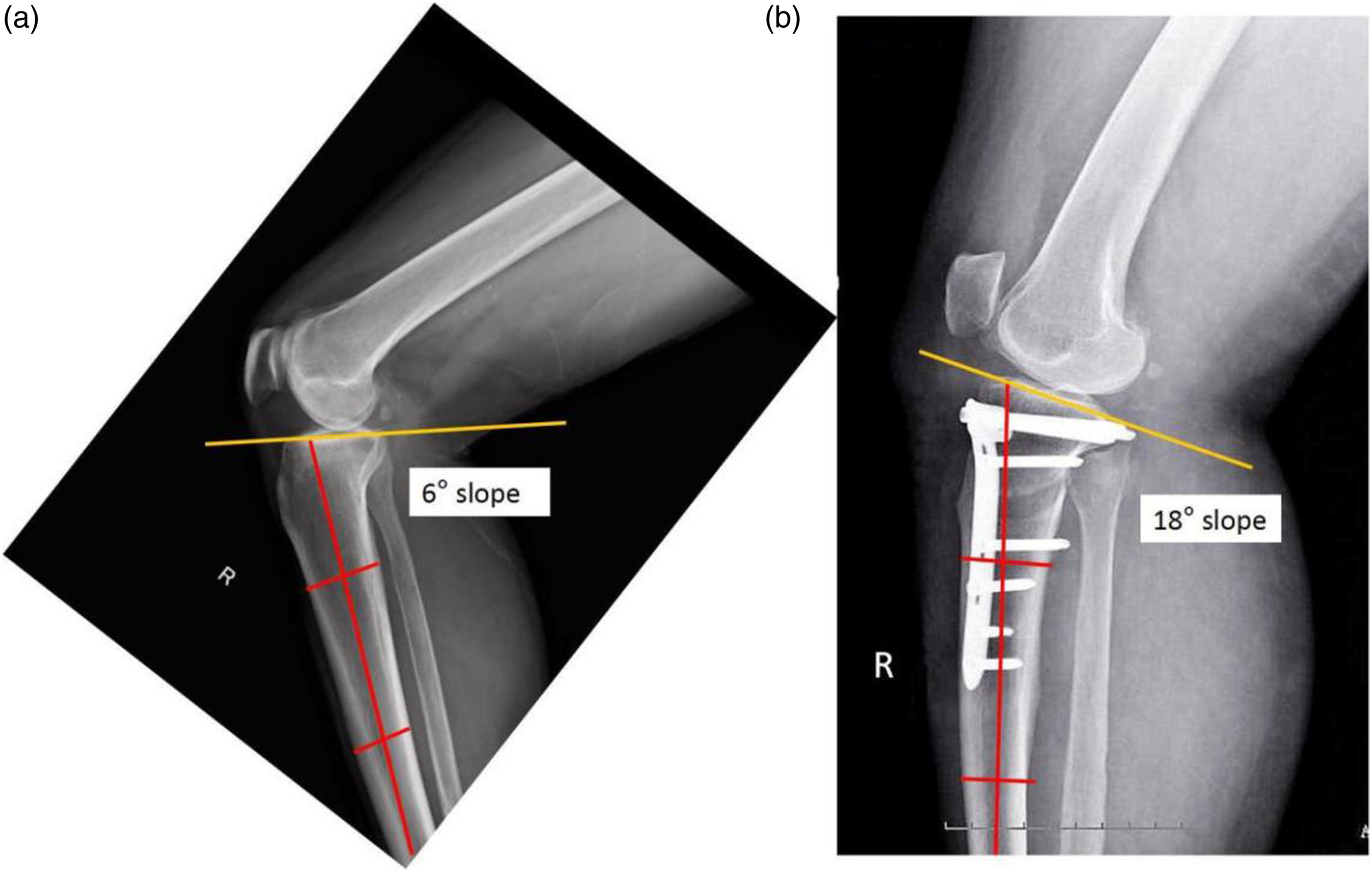
All patients’ knee condition was clinically evaluated preoperatively and at final follow-up using the Lysholm score, HSS (hospital for special surgery knee score), and KSS (knee society score) through clinical follow-up or telephone follow-up. These measurements were performed by a physician independent of the surgical team and blinded to the radiographic findings. The mean follow-up period was 28.5 months (SD, 4.9; range 18–52 months).
Statistical analysis
All radiographic parameters were collected by two experienced orthopaedic surgeons and repeatedly assessed in a blinded fashion 1 month after the first measurement in order to reduce bias. The interclass correlation coefficients for the intra- and inter-observer agreements were calculated. Statistical evaluation was performed using SPSS 22.0 (IBM Corp., Armonk, NY, USA). The continuous data are presented as mean values ± SD. Student’s t test was used to analyze quantitative data, and the chi-squared test was used to analyze qualitative data. We adopted the ANVOA and paired t-tests to compare the differences among three cohorts. The p values of < .05 were considered statistically significant.
Results
Demographics characteristics.

LCA: large correction angle; MCA: medium correction angle; SCA: small correction angle; BMI: body mass index; mo: month; K-L grade: the Kellgren and Lawrence grade; ▲p values are from one-way ANOVA for continuous variables and from chi-square test for categorical variables.
Intraclass correlation coefficients for intraobserver and interobserver of PTS, ISI, and BPI.

PTS: posterior tibial slope; PH: patellar height.
Mean desired correction angle was 12.19°(range 6°–20°); measured postoperative correction angle was 11.95°(range 5.6°–19.7°). The LCA group yielded tibial slopes that were significantly different from the SCA group and MCA group. The mean difference of PTS for the LCA group was 3.12 ± 0.87. The difference from baseline PTS is smallest for the SCA group (0.37 ± 0.15) and greatest for the LCA group. In terms of PH, the LCA group yielded ISI and BPI that were significantly different from baseline for the SCA group and MCA group. The mean difference of ISI and BPI for the LCA group were 0.23 ± 0.089 and 0.16 ± 0.096, respectively. The difference from baseline ISI and BPI are all smallest for the SCA group (0.042 ± 0.014 and 0.012 ± 0.0089, respectively) and greatest for the LCA group.
The effect of amount of correction on change in PTS was analyzed. The relationship between amount of correction and slope is significant (p < .001). The pairwise difference between the LCA group and the SCA group and the MCA group was significant (p < .05). However, the difference in the SCA group and MCA group had no significance (p = .435) (Figure 2). The mean change and 95% CI for the PTS before and after surgery in each of the three groups are shown.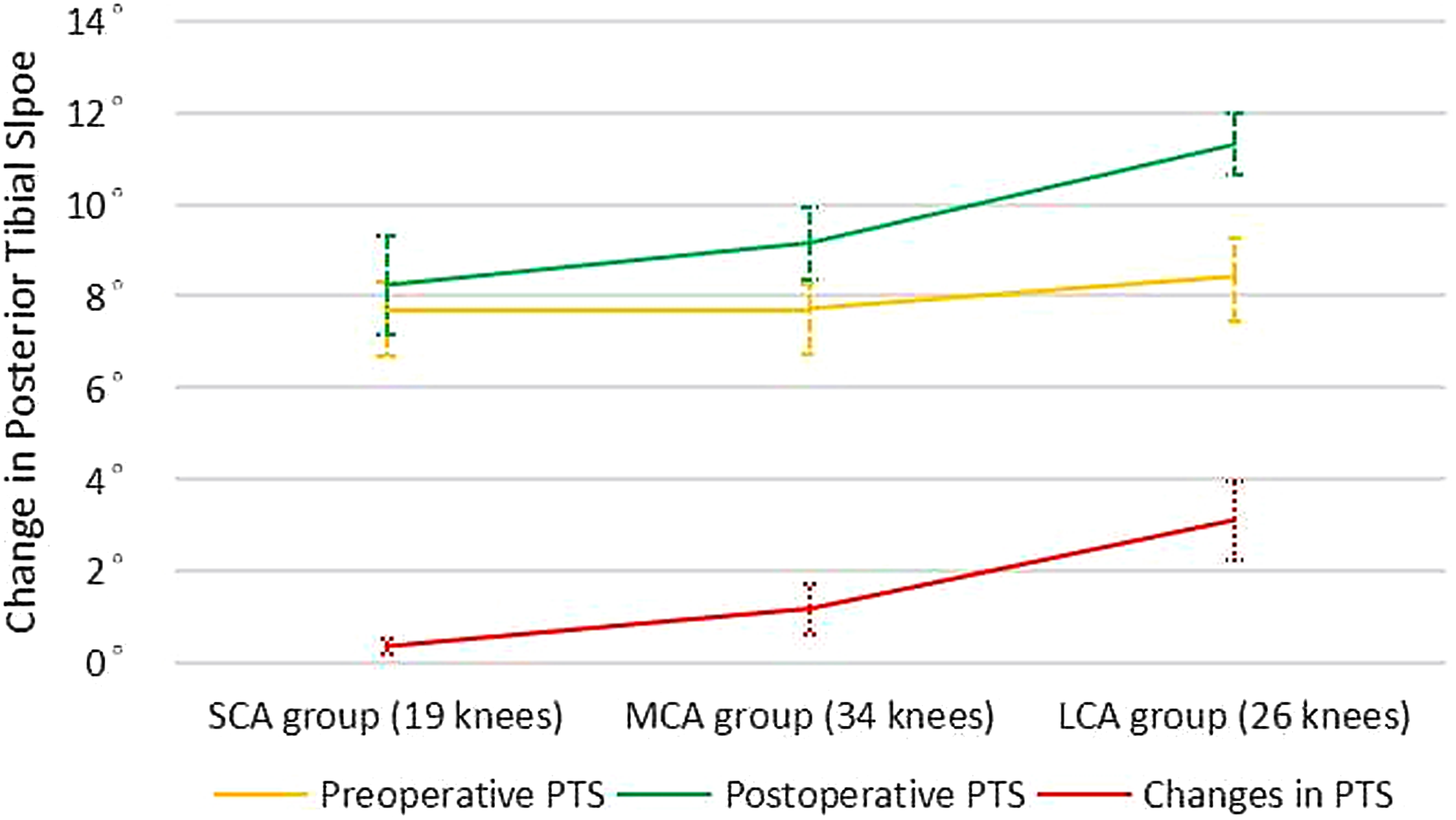
The effect of amount of correction on change in PH was also analyzed. The relationship between amount of correction and ISI and BPI was significant respectively (p = .03, p = .031). The pairwise difference between the SCA group and LCA group in ISI and BPI is significant (p = .031); however, the pairwise difference between the SCA group and MCA group and between MCA group and LCA group had no significance in ISI and BPI, respectively (p < .05) (Figures 3 and 4). The patellar height of ISI before and after surgery in the three groups with 95% CI is shown. The patellar height of BPI before and after surgery in the three groups with 95% CI is shown.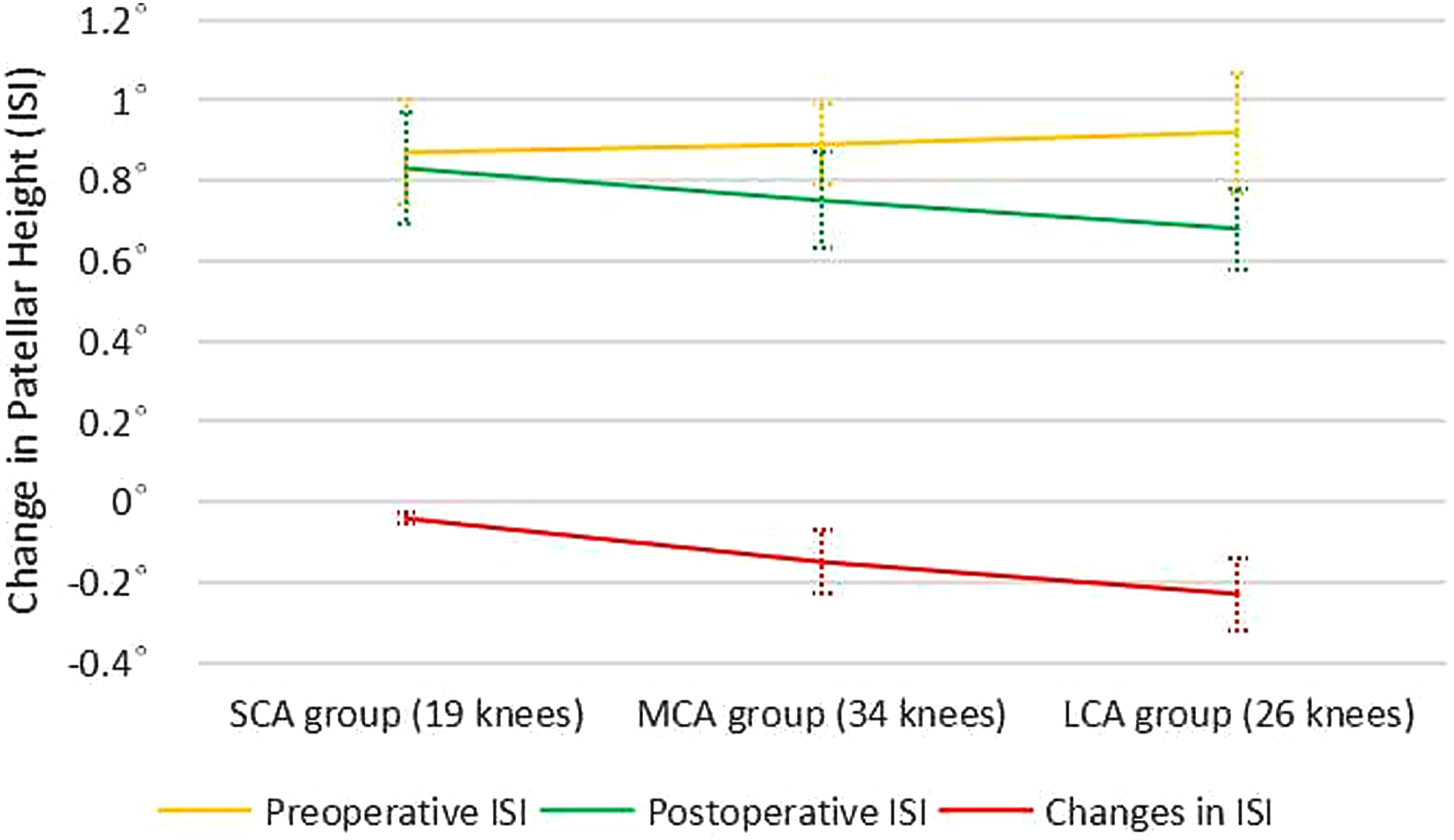

Clinically, the preoperative mean Lysholm score, HSS score, and KSS score of the knees had improved substantially after surgery (Figure 5). Furthermore, there were significant improvements of knee scores in each of the three groups, respectively, which corresponded to functional results that were excellent in 41 knees, good in 18 knees, fair in 16 knees, and poor in 4 knees. No correlation was found between changes in PTS and PH with postoperative Lysholm score, HSS score, and KSS score. Seventy-four patients (93.67%) reported satisfaction with surgery. Preoperative and postoperative clinical evaluations. HSS: hospital for special surgery knee score; KSS: knee society score; ▲p values for comparing the three treatment groups at the same times are from ANOVA, p < .001.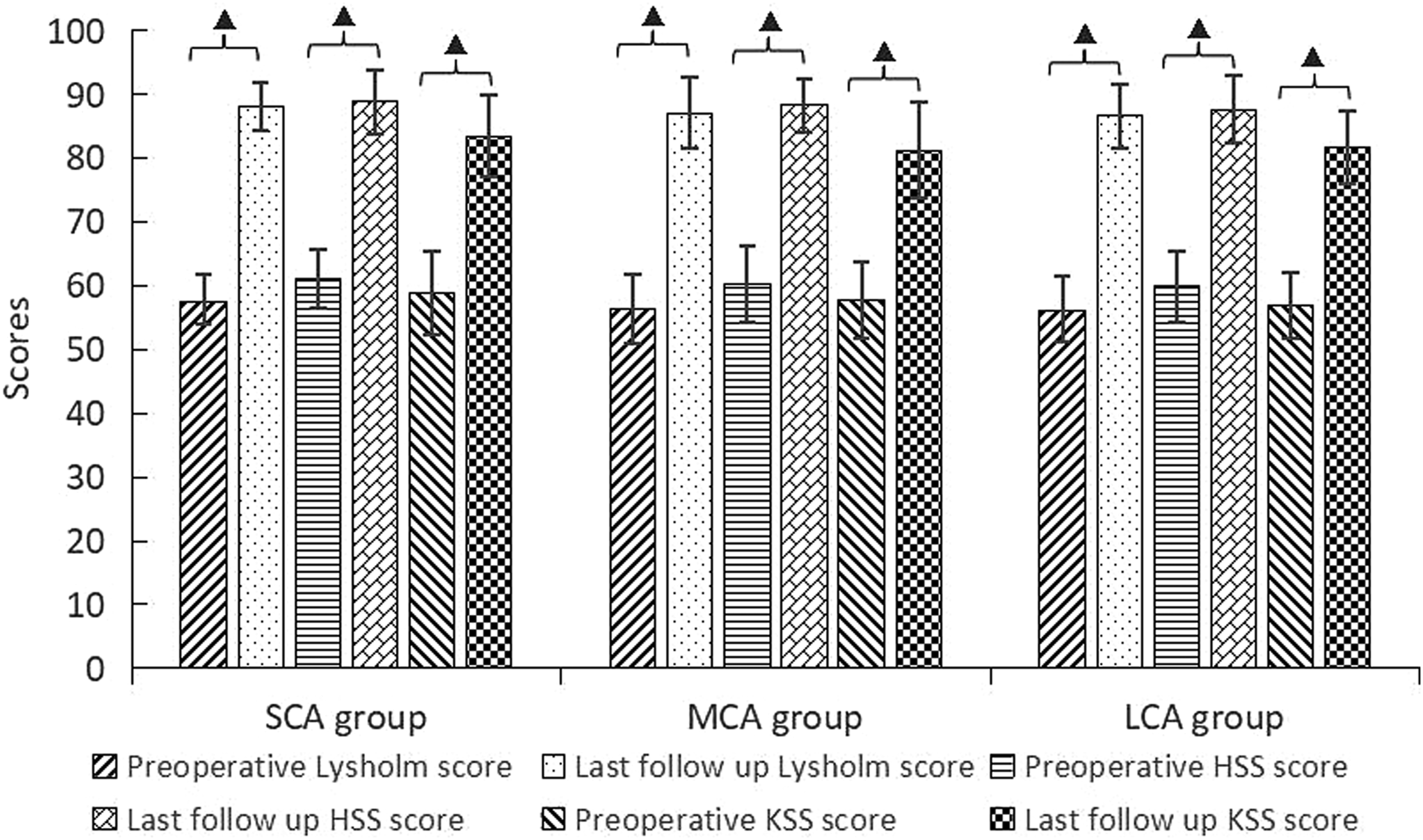
With regard to complications, five patients developed non-displaced fractures within the tibiofibular joint intraoperatively (type I, according to Takeuchi’s classification 29 ). Fixation was performed with long metaphyseal cancellous bone screws followed by 4 weeks of delayed postoperative mobilization exercises. Finally, these patients were observed without obvious functional deficit. Two other patients developed superficial infections, which resolved completely with intravenous antibiotics therapy and wound dressing change.
Discussion
The most important finding of the present study is that correction angle was a significant factor affecting the PTS and PH in patients who underwent OWHTO. The changes are highly variable and often the amount of change is too small to be clinically significant; however, the maximum assessed changes during this study (maximal PTS change 12°, maximal ISI change 0.9, and maximal BPI change 0.75) highlight the need to be vigilant for these problems.
To our knowledge, this is the first clinical study evaluating the effect of different amount of correction on PTS and PH in OWHTO to date. PTS is important for knee extension and flexion, the correct function of the cruciate ligaments, and normal knee kinematics. 30 In OWHTO, several factors could influence PTS, including the amount of correction, 20 optimal gap ratio in the sagittal plane,31–33 hinge position,31,32 hinge fracture, insufficient posterior osteotomy, and release of soft tissue.31,34 Many studies have demonstrated an increased PTS after OWHTO.7,17,20,35–37
In our study, we observed that the mean postoperative PTS increased. The change of PTS in the MCA group and LCA group showed a significant difference compared with preoperative PTS. And, the LCA group yielded tibial slopes that were significantly different from the SCA group and MCA group, which indicates that the amount of correction performed is one of the key factors affecting the PTS after OWHTO. It is clear that the larger the correction, the more freedom is present for PTS or PH. Matthias et al. 20 evaluated the influence of certain intraoperative factors of the degree of PTS change observed during OWHTO through a cadaveric model. They found that larger corrections yielded not only increased mean values for PTS but also increased variability in the observed values. The changes noted in small corrections were generally below clinical significance; however, in cases with concomitant ACL deficiency, even small changes may be important. This result is consistent with another cadaveric study conducted by Rubino et al. 19 El-Azab et al. 38 found that PTS increased after OWHTO because of the geometry of the proximal tibial, which dictates corresponding sagittal plane changes in coronal plane osteotomies. In a recent meta-analysis, an unintentional mean postoperative slope increase of 2.02° has been detected in OWHTO. 39
It has been suggested that increased PTS may result in knee instability and tibial translation including increased ACL strain and posteriorly shifted intra-articular cartilage peak pressure. In addition, those patients with increased PTS often underwent more bone loss of the tibial plateau posteriorly, which could make it more difficult to possible future total knee arthroplasty (TKA). 40 However, the incorporation of specific surgical techniques such as controlling anterior/posterior osteotomy opening gap ratio between 2:3, 41 a complete osteotomy of the posterior cortex, 42 putting the plate as far posteriorly as possible, 43 using reference K-wires for intra-operative PTS orientation, 44 applying a bicortical screw to fix the distal tuberosity to the tibia, 45 and avoiding larger corrections 43 may helpful in minimizing PTS change. Nevertheless, of course, such an increased PTS can be beneficial in cases of posterior cruciate ligament deficiency as it can lead to anterior translation of the tibial relative to the femur, especially if ACL deficiency is present. 46
Ideally, any surgery on the knee should not significantly worsen the position of the patella and more attention should be paid to avoid patellofemoral issues. A normal PH is an important determinant for knee function, which otherwise may result in anterior knee pain, decreased range of motion, patellofemoral arthrosis, and potentially complicated future TKA.9,35 However, we observed that the mean postoperative patellar height decreased after OWHTO in our study. The mean change in ISI and BPI between the SCA group and LCA group is significant (p < .05); thus, we speculated that larger correction angle seems to decrease the patellar position and may have a negative impact on patellar height. In OWHTO, due to the attachment of the tuberosity to the distal fragment, the tibial insertion of the patellar is distalized. Also, a potential postoperative tendon shortening caused by scarring may occur.
Hence, in order to avoid a PH decrease, Gaasbeek et al. 47 introduced a biplanar descending OWHTO, of which sagittal osteotomy line was below the tibial tuberosity. Krause et al. 2 conducted a study to gain insight into geometric changes of the PH and PTS after biplanar ascending OWHTO compared to descending OWHTO in patients with KOA. They found that descending OWHTO has proven useful to control PH and PTS, which is in line with other previous results.44,48–50 However, these techniques are technically demanding and could lead to the potential for fracture of tibial tubercle fragment. Park et al. 51 found two tibial tuberosity fractures with descending OWHTO in 33 patients, but they noted that this complication is preventable by leaving more than 1 cm thickness on the proximal tuberosity fragment.
There was a significant increase in the clinical score after OWHTO. Overall, OWHTO is an effective treatment for isolated medial compartment KOA in varus knees. Patients reported pain relief, improvement in whole-knee function, and satisfaction with the clinical outcome. No patellofemoral joint symptoms or other uncomfortable symptoms were observed. Although increased PTS and descent of the patella were observed, postoperative knee scores showed improvement compared with preoperative values, indicating changes of PTS and PH had no meaningful effect on clinical result in short term. In addition, there were no significant difference in terms of postoperative knee scores among three groups, suggesting the effect of different correction angles on knee function and pain was limited.
This study was not without limitations. First, the sample was relatively small and the follow-up was relatively short. Large sample size research and long-term follow-up were required to further evaluate the effect of correction angles on knee joint. Second, the slope was measured only with plain radiographs, and this may predispose to measurement error. But, two experienced observers evaluated radiographic parameters twice in a blinded fashion, which could possibly minimize potential bias from this limitation. Third, no single method of measuring PH has been accepted as the gold standard so far. Each method has its own particular limitations, which is probably why numerous previous studies have used two or three methods.
Conclusion
OWHTO is an effective procedure to unload the medial compartment of knee joint. The amount of correction angle is a significant factor affecting the PTS and PH in OWHTO clinically, although no association was found between those unintended changes and worsening knee clinical symptoms in short term. With increased correction in the coronal plane, the likelihood of increasing the PTS and decreasing the PH increases. We conclude that special attention should be paid to keep PTS and PH unchanged in cases where large corrections are required. Otherwise, closing wedge osteotomy or other intraoperative effective measures are supposed to be adopted.
Footnotes
Acknowledgments
This study was supported by the Third Department of Orthopedics, The First Affiliated Hospital of Guangzhou University of Chinese Medicine. However, the interpretation and conclusions contained in this study are those of the authors alone.
Author Contributions
Yirong Zeng conceived the study.Keliang Wu acquired the data.Jianchun Zeng, Linjing Han, Wenjun Feng, and Xiaosheng Lin developed the analysis plan.Xiaosheng Lin and JLC analyzed the data.Jianchun Zeng and Keliang Wu drafted the manuscript.Keliang Wu, Jianchun Zeng, Linjing Han, Xiaosheng Lin, Wenjun Feng, and Yirong Zeng revised the manuscript.All authors contributed intellectually to the interpretation of the data, participated in manuscript development, and approved the final version.
Ethics approval and consent to participate
Approval was granted by the First Affiliated Hospital of Guangzhou University of Chinese Medicine.
Guarantor
YRZ.
Declaration of conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.