
Abstract
Level of evidence: I
Introduction
Numerous minor hand surgeries are performed under local anesthesia (LA) given its convenience. Compared with general anesthesia, LA allows patients to avoid preoperative evaluation, prolonged admission for recovery, and side effects of anesthetic drugs.1–3
The hand surgeries which usually take less than 30 min such as A1 pulley release, extensor retinaculum release, and carpal tunnel release, which are defined as “minor hand surgery,” have been performed under LA. For a successful hand surgery under LA, preventing pain in the patient and controlling bleeding to optimize visualization of the surgical field are necessary. In conventional LA, these are achieved by injecting pure lidocaine and using a pneumatic tourniquet. However, tourniquet use is associated with significant intraoperative discomfort due to pain and complications such as nerve injury and pressure sore. 4 A previous study reported that the mean tolerance time for arm tourniquet was 18–25 min 5 Moreover, injecting 1% lidocaine in hand surgery has been shown to induce extreme pain (about 6–7 on the visual analog scale, VAS). 6
Recently, a novel technique (wide awake local anesthesia no tourniquet, WALANT) has become popular for eliminating tourniquet and reducing injection pain. In this technique, the surgeon administers a local injection of a mixture of lidocaine, epinephrine, and sodium bicarbonate (NaHCO3). The vasoconstriction effect of epinephrine achieves hemostasis, and the NaHCO3 reduces injection pain by altering the pH of the solution close to that of normal tissue.1–3
Since tourniquet is only tolerable for about 20 min, by eliminating tourniquet use, WALANT allows for longer surgeries, including distal radius fracture plating, finger and hand fractures, tendon transfer, and cubital tunnel release. It is a good alternative to general anesthesia and can be used for patients with numerous medical comorbidities. 1
However, in WALANT, the solution must be injected 25–30 min before incision for maximum hemostatic effect. 7 During the waiting period, patients might have increased anxiety and discomfort from strange place. Surgeon may require additional resources for pre-injection and being on standby to monitor the patient.
The tourniquet has the advantage of achieving an immediate hemostatic effect without any waiting time. Additionally, a recent study reported that LA injection was more painful compared than pneumatic tourniquet during minor hand surgery. 8 Injection pain can be reduced using a buffered solution: a mixture of lidocaine and NaHCO3. 9 Therefore, using a tourniquet and buffered solution could be an alternative method that could reduce the overall operation time and pain during minor hand surgery. Therefore, this study aimed to compare CTB, WALANT, and conventional LA to answer the following questions: (1) Does CTB have an advantage with respect to injection and tourniquet pain? (2) How much time is saved with CTB compared with WALANT? (3) What is the patient satisfaction with CTB compared with other methods? And (4) does the chosen local anesthetic method affect the postoperative clinical outcome?
Materials and methods
Study design
This study was approved by our Institutional Review Board. Data from all the patients treated during the study period are available for review and analysis. All the participants provided informed consent before data collection. This study used a convenience sample of individuals attending clinics at our university hospital with patients who met the inclusion criteria being invited to participate in the study.
Patients and evaluation
We conducted a randomized prospective cohort single-center study on patients who underwent minor hand surgery. The inclusion criteria included patients diagnosed with trigger finger, carpal tunnel syndrome (CTS), and de Quervain’s disease by a hand specialist in the orthopedic clinic. We excluded patients with peripheral neurovascular disease, allergy to lidocaine or epinephrine, hematologic disorders, arteriovenous shunt for hemodialysis, and previous LA hand surgery history, and those who could not cooperate with the description of the surgery experience.
From March 2017 to October 2020, we included 193 patients who met the eligibility criteria. The patients were randomly allocated to the CTB, WALANT, or conventional groups. The randomization process was performed using a computer-generated random allocation; moreover, a researcher blinded to the study allocated the patients using the permuted block randomization method. Consequently, 64 patients were assigned to the CTB and WALANT groups while 65 patients were allocated to the conventional group (Figure 1). Flow diagram of the progress through the phases of a parallel randomized trial of each group.
Operative procedure
Patients in the CTB group underwent surgery with buffered lidocaine solution and tourniquet. The buffered solution was a mixture of 1% lidocaine and 8.5% sodium bicarbonate at a 10:1 ratio to make it close to the pH of normal tissue (7.2). 10 In the conventional group, pure 1% lidocaine was used for local injection with a pneumatic tourniquet. In both groups, an upper arm tourniquet was applied for hemostasis. In the WALANT group, we used a cocktail solution that included 100 mL of 1% lidocaine, 1 mL of epinephrine (1:1000), and 10 mL of 8.4% sodium bicarbonate without a tourniquet. We prepared phentolamine (phentolamine mesylate, Reyon Pharm Co, Ltd, Seoul, Korea) as a reversal agent for emergency cases of digital ischemia. All injections were administered at room temperature.
All the patients underwent surgery in the same operation room that was specially assigned for LA. An upper arm tourniquet was applied in the CTB and conventional groups, approximately 10 cm above the medial epicondyle in the preparation room. The patients were immediately transferred to the operation room, and the standard draping procedure was followed. Subsequently, a tourniquet cuff was applied with 250 mmHg after elevating the arm for 5 min. Before the procedure, buffered and plain lidocaine was administered to the CTB and conventional groups.
Patients in the WALANT group received the cocktail solution in the preparation room about 30 min before surgery since it takes approximately 26 min to allow for maximal vasoconstrictive effects of epinephrine. 11 The patients were monitored by the assigned nurse while waiting in the preparation room in case of emergencies, including digital ischemia, allergic reaction, and falling accident. Five minutes before surgery, the patients were brought into the operation room for surgery.
An adequate amount of solution was administered for each procedure: 4 mL, 10 mL, and 20 mL for A1 pulley release, extensor retinaculum release, and carpal tunnel release (CTR), respectively.
1
The amount of lidocaine with epinephrine used for the procedure was lesser than the safe dose (7 mg/kg).
12
To minimize injection pain, we used the “hole-in-one” injection technique for all patients. The steps involved in this technique are as follows: (1) use a long 25-gauge needle for injection to minimize insertion pain, (2) stabilize the needle with the thumb to avoid needle wobble during the initial injection, (3) to distract the injection site using sensory noise, pinch or press the area proximal to the insertion site, (4) insert needle perpendicular to the skin until it reaches under the dermis, and (5) inject 2–3 ml of the solution before moving the needle and always inject proximal to distal with respect to the nerve passage (Figure 2).
13
A “hole-in-one” technique for local anesthesia (LA) injections using a long needle. (Left) the initial needle insertion is perpendicular to the skin and reaches the subdermal. The proximal site of needle injection is pinched or pressed for sensory noise. (Middle) Enough LA injection is spread before the advancement of the needle tip. (Right) An adequate LA amount is injected into a wide area using one injection site.
Assessments
Before surgery, the assigned nurse recorded the preparation time (time from tourniquet application to skin incision in the CTB and conventional groups, and as the time from injection to skin incision in the WALANT group).
During the surgery, the start time (first skin incision time) and end time (completed last suture) were recorded. For the CTB and conventional groups, the tourniquet time was also recorded.
Immediately after the surgery, the patients were asked to complete a questionnaire. For the CTB and conventional groups, tourniquet pain was quantified using a VAS. For all patients, injection pain was assessed using the VAS. Surgery-related anxiety was assessed using the Hamilton Anxiety Rating Scale (HAM-A). 14 The HAM-A comprises 14 items that measure both psychic anxiety (mental agitation and psychological distress) and somatic anxiety (anxiety-related physical complaints). However, not all 14 questions are appropriate for short-term anxiety measurement; accordingly, we selected 10 HAM-A items to assess the patients. Each item is scored on a scale of 0 (not present) to 4 (severe), with a total score range of 0–40. Surgery-related anxiety was defined as “anxiety during the period from admission and leaving the operating room”. The patients were asked to write down factors that made them anxious. To assess for postoperative pain, the patients were asked about surgical site pain at six postoperative hours. To distinguish surgical site pain from tourniquet-related pain, we asked if the pain was limited to surgical site or extended to the upper arm, and if there was any numbness in the operated arm.
The patients were discharged on the day of surgery and were reviewed at the clinic days after the operation. Patient satisfaction with the procedure was assessed using a 5-point Likert scale (very dissatisfied, 1 point; dissatisfied, 2 points; neither, 3 points; satisfied, 4 points; and very satisfied, 5 points). 15 Patients were also asked whether they would choose to undergo the same LA procedure (strongly disagree, 1 point; disagree, 2 points; neither, 3 points; agree, 4 points; and strongly agree, 5 points). The next follow-up appointment was 2 weeks postoperation to assess for complications.
The patients were asked to visit the clinic at three and six postoperative months to assess the clinical outcome. The Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire was used to evaluate hand function. In patients with trigger finger, the Quinnell grade was used to evaluate clinical symptoms; 0, normal digit movement; 1, uneven movement; 2, actively correctable locking of the digit; 3, passively correctible locking; and 4, fixed deformity. 16 In the CTS group, the historical-objective (Hi-Ob) scale was used to evaluate clinical symptoms; stage 0, no CTS-suggestive symptoms; stage 1, only nocturnal paresthesia; stage 2, diurnal paresthesia; stage 3, sensory deficit; stage 4, hypotrophy and/or motor deficit of the median innervated thenar muscles; and stage 5, complete atrophy or plegia of the median-innervated thenar muscles. 17
Statistical analysis
Continuous data are presented as mean and standard deviation while categorical data are presented as percentage and frequency. Continuous variables were compared using one-way analysis of variance, while categorical data were compared using the × 2 test and Fisher’s z-test. Statistical significance was set at p-value < 0.05. Statistical analyses were performed using SPSS version 23 software (IBM, Armonk, NY, USA).
Results
Demographic data and diagnosis of the patients.
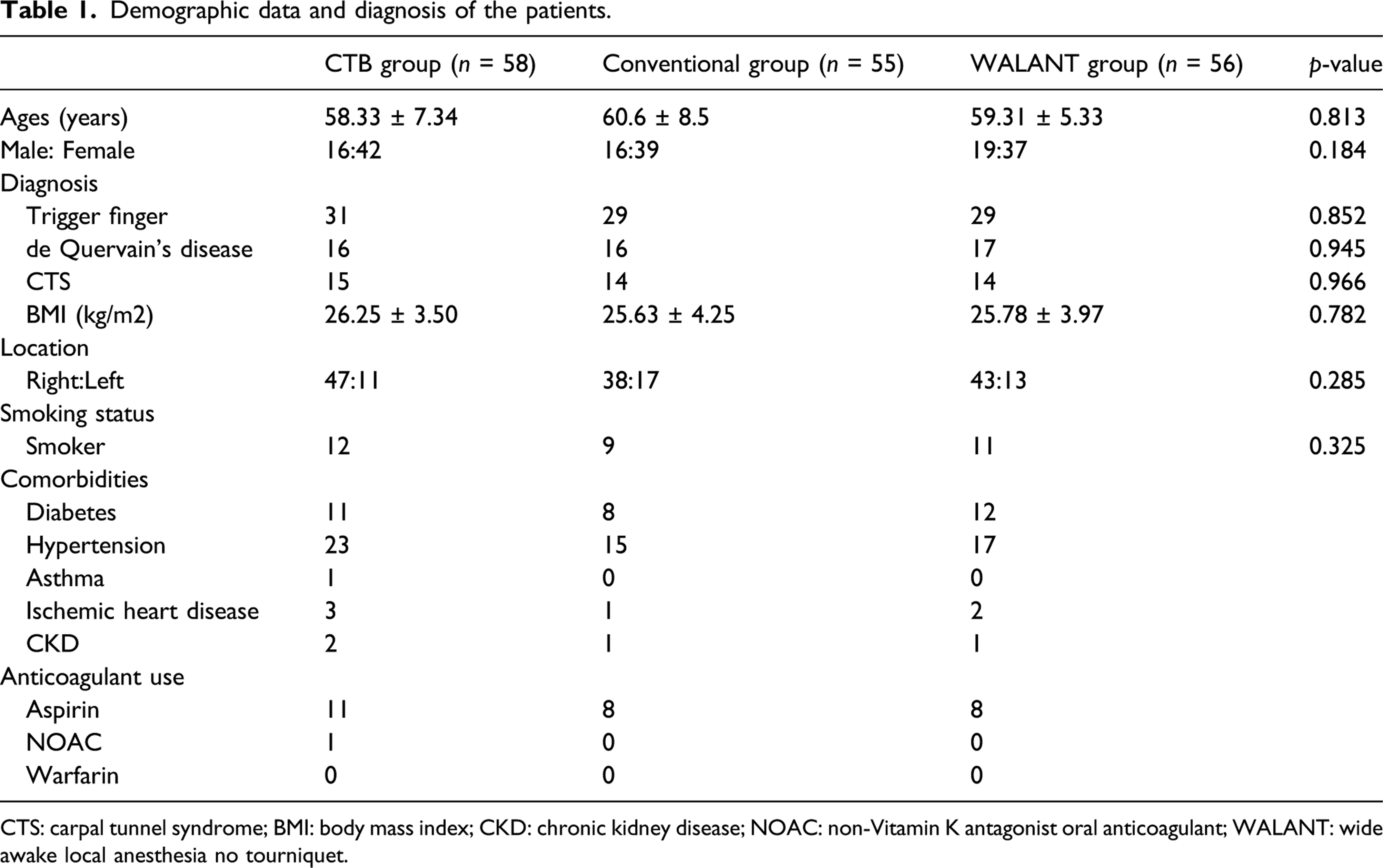
CTS: carpal tunnel syndrome; BMI: body mass index; CKD: chronic kidney disease; NOAC: non-Vitamin K antagonist oral anticoagulant; WALANT: wide awake local anesthesia no tourniquet.
In each procedure, there was no significant group difference in the operation time. The preparation time was significantly longer in the WALANT group (by approximately 30 min) than in the CTB and conventional groups (p < 0.001).
Operation time and preoperative preparation time.

CTR: carpal tunnel release; WALANT: wide awake local anesthesia no tourniquet.
The injection pain was significantly higher in the conventional group than in the CTB and WALANT groups (5.87 ± 1.45 vs 3.85 ± 1.03 vs 3.90 ± 1.03, p < 0.001). The mean tourniquet pain was 2.93 ± 1.09 and 3.08 ± 0.87 in the CTB and conventional groups, respectively, without a significant between-group difference. However, tourniquet pain in both groups was significantly lower than injection pain (p < 0.001). Six-hour postoperative pain was significantly low in the WALANT group than in the CTB and conventional groups (1.38 ± 0.56 vs 2.45 ± 0.88 vs 2.25 ± 0.92, p < 0.001) (Figure 3). The intraoperative anxiety score was significantly higher in the conventional group than in the CTB and WALANT groups (21.15 ± 6.53 vs 13.42 ± 5.35 vs 17.32 ± 5.96, p < 0.001) (Figure 4). A bar graph showing the mean visual analog scale (VAS) scores for injection, tourniquet, and postoperative pain in each group. A box and whisker plot showing the intraoperative anxiety score (HAM-A) in each group.

Administered LA was adequate for all groups, without intraoperative administration of an additional injection. No patient required tourniquet deflation. Furthermore, there was no evidence of epinephrine-related complications, including white finger, digital skin, and necrosis.
The mean satisfaction scores on the 5-point Likert scale were significantly higher in the WALANT and CTB groups than in the conventional group (4.12 ± 0.75 vs 3.95 ± 0.69 vs 1.95 ± 1.03, p < 0.001). The satisfaction score in the CTB group was not significantly higher than that in the WALANT group (p = 0.265).
Patients in the CTB and WALANT groups were more likely to choose the same method than patients in the conventional group (3.75 ± 0.83 vs 3.65 ± 1.12 vs 2.02 ± 0.75, p < 0.001). There was no significant difference between the CTB and WALANT groups (p = 0.415) (Figure 5). A cumulative bar graph showing the satisfaction score and willingness to re-undergo the same procedure (5-point Likert scale) for each procedure.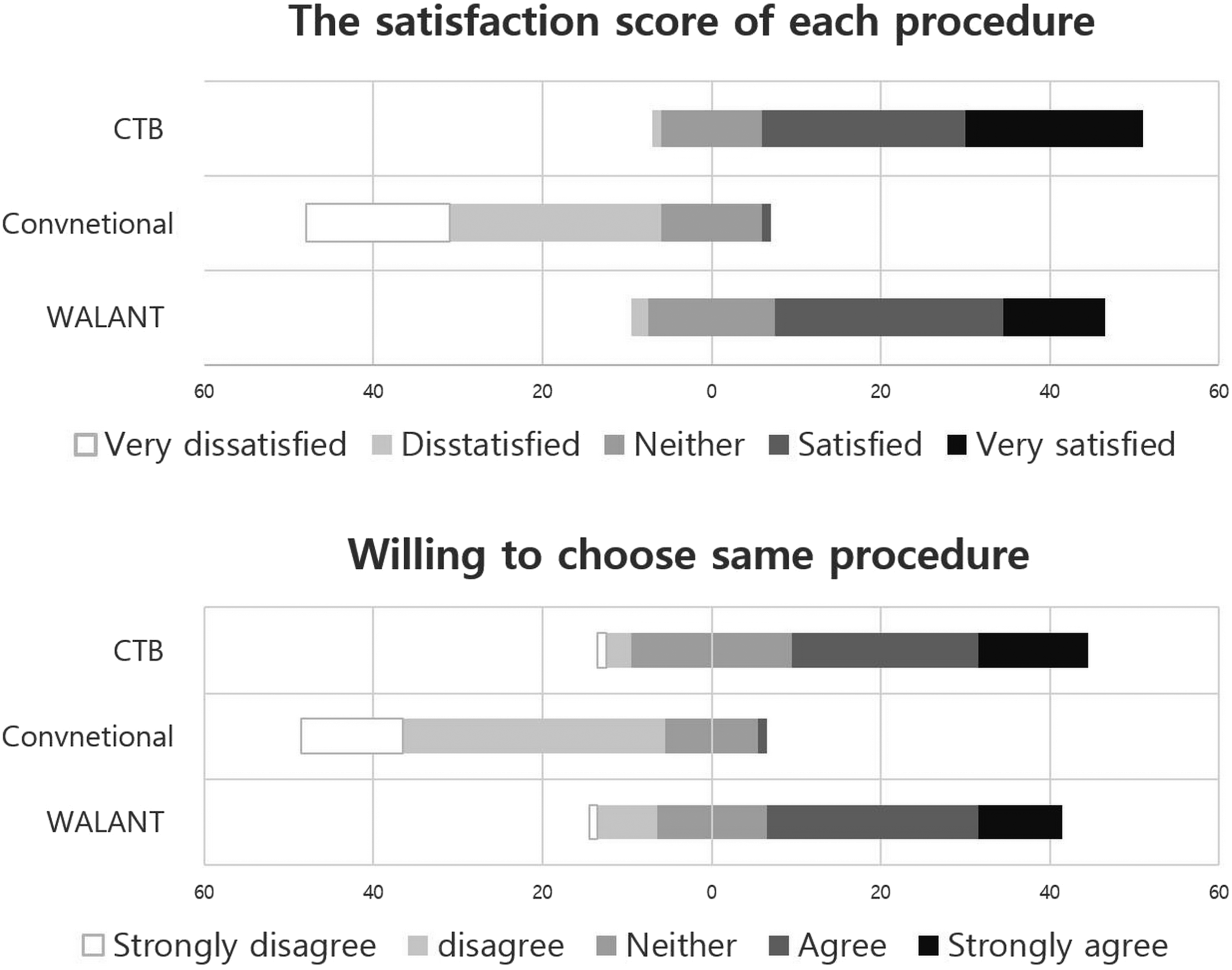
There was no significant difference in the clinical outcome for the DASH score’s pre/postoperative functional ratio in all groups. Moreover, there was no significant difference between the Quinnell and Hi-Ob scores of patients with trigger finger and CTS for all LA methods. On the 2 weeks postoperative review, two patients (one underwent CTR with the WALANT technique, and the other underwent CTR with the conventional method) had superficial wound infection. Both patients were successfully treated with extra wound dressing and oral antibiotics.
Discussion
This study showed that LA using buffered lidocaine solution and tourniquet had better outcomes with respect to pain and patient satisfaction than conventional methods; furthermore, it involved lower anxiety than WALANT and conventional methods.
Conventionally, hemostasis during hand surgery has been achieved by a pneumatic tourniquet. However, pain related to the tourniquet has been a persistent issue. One study reported similar findings and introduced a new technique, WALANT. 18 The WALANT technique has expanded the number of surgical procedures under LA by eliminating the need for a tourniquet. However, for minor hand surgery, which can be performed within 20 min, the tourniquet can be employed without much pain. A recent study assessed pain and patient experience for minor hand surgery using a tourniquet. It reported that compared with pneumatic tourniquet use, LA injection was more painful. 8 Therefore, minimizing injection pain is a more important issue in minor hand surgery. Therefore, the present study examined three LA methods with differences in hemostasis and anesthesia. To evaluate them from various perspectives, we performed comparisons of not only pain but also the patients’ anxiety and satisfaction of the three methods. Our findings confirmed the hypothesis that tourniquet is well tolerated in minor hand surgery. Specifically, a local anesthetic injection was more painful than tourniquet use. The mean operation time for patients with trigger finger, CTS, and de Quervain’s disease was approximately 10 min, with the most protracted case being less than 20 min. Therefore, the mean tourniquet time was even lesser than 20 min. Many studies have shown that arm tourniquet was tolerable for 20 min.5,19,20,21 However, these previous studies were limited, in that only time was measured, and quantitative pain measurement was not undertaken. The present study measured tourniquet pain using a VAS, which was significantly lower than pain during injection of pure lidocaine, buffered, and WALANT solution. The tourniquet was well tolerated, and none of the patients demanded tourniquet deflation. Injection pain also results from needle insertion which causes sudden and sharp pain regardless of the subsequently injected solution. Therefore, injection was more painful than tourniquet in minor hand surgery.
The CTB group had the lowest anxiety score. The result could be attributed to lower injection pain given that many patients in the conventional group indicated that extreme pre-injection pain made them anxious even when they did not feel postinjection pain. Compared with WALANT, CTB significantly shortened overall operation time (preparation time + operation time). Several patients in the WALANT group reported that the long preoperative waiting time made them anxious. Specifically, in the WALANT group, one patient with irritable bowel syndrome indicated that waiting 30 min before the procedure was a very nervous experience due to abdominal discomfort and the fear of defecation.
Among the three groups, the CTB group had the highest patient satisfaction score and many patients would choose to undergo the same procedure again. This high patient satisfaction score could be attributed to less injection and tourniquet pain, short operation time, and low anxiety score.
Although the CTB group showed the lowest anxiety and highest satisfaction scores, a few patients reported similar complaints to patients in the conventional LA group. Specifically, they complained that inserting the needle before the procedure startled them even with a previous warning. None of the patients in the WALANT group reported such a complaint. This could be attributed to differences in the environment during the injection. The WALANT group received injections in the preparation room with eye-to-eye contact, communication, and the ability to watch the injection process. Contrastingly, the patients in the other groups received injections in the operation room after draping; their sight was blocked, which made them very sensitive to slight stimulation. Therefore, we recommend injecting LA solution in more comfortable settings and maintain eye contact with the patient before surgery. This could contribute to a stronger doctor–patient rapport and better satisfaction.
Despite the low risk of epinephrine-related complications, five reported cases of digital necrosis related to epinephrine use have been reported.22–26 In one of the cases, the patient underwent trigger finger surgery using the WALANT technique and presented to the emergency room the following morning with complaints of severe pain in the operated fingertips. There was apparent tissue necrosis, which resulted in amputation of the index and middle finger tip. 23 Although numerous hand surgeries have been successfully performed using the WALANT technique, there is a need for careful epinephrine injection in the most peripheral end with small vessels. For surgical case involving the wrist, elbow, arm, and ankle, which have larger vessels and adequate collateral circulation, there is a relatively low risk of the vasoconstriction effect of epinephrine. However, most peripheral body parts, including the fingers, are vulnerable to ischemia upon small vessel constriction. Therefore, the surgeon should always be aware of the epinephrine-related risk; moreover, they should carefully perform intra-tendinous and high-volume injection, as well as phentolamine preparation. Epinephrine use should be avoided in patients with peripheral vascular disease, ischemic heart disease, diabetes, and heavy smoking history. When performing the WALANT technique, the surgeon should be aware of the need for extra postoperative monitoring. The patient should be informed about the risk of complications.
The WALANT technique has numerous advantages for hand surgery under LA. Hemostasis without a tourniquet allows surgeons to perform numerous types of long hand surgery under LA. However, the CTB has an advantage in minor hand surgery regarding its shorter preparation time, which leads to lesser intraoperative anxiety. Therefore, the CTB could be a good alternative option for minor hand surgery.
This study has several limitations. First, this was not a double-blinded study. Since the tourniquet was only used for the CTB and conventional groups, it was difficult to blind the surgeon and observer. Second, we performed a subjective evaluation of pain, anxiety, and satisfaction since each individual has a unique threshold for each object.
However, the limitations are mentioned above counterbalanced by the strengths of the study. First, since we based our analyses on prospective studies, we effectively avoided recall bias and reduced the likelihood of selection bias. Moreover, we attempted to maintain objectivity and eliminate detection bias since data collection and analysis were conducted by individuals not involved in the study.
Conclusion
CTB for minor hand surgery under LA is associated with less injection pain and patient anxiety. The tourniquet is tolerable without much pain and waiting time since operation time was short. Thus, CTB in minor hand surgery is a viable alternative to WALANT and conventional LA.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.