
Abstract
Purpose
This study aimed to evaluate the relationship between talofibular impingement and increased talar tilt in incongruent varus ankle osteoarthritis.
Introduction
The prevalence of ankle arthritis worldwide is about 1%. 1 Unlike other large joints, majority of ankle arthritis is posttraumatic such as those caused by fracture and ankle instability.1–3
Varus ankle osteoarthritis (OA) seems to be more frequently observed in Asians. Although there is a lack of studies comparing the prevalence between races and analyzing the cause, Kim et al. presumed that this predominance is probably due to their lifestyle, in which people tend to sit cross-legged in a lotus position or kneel in ankle plantar flexed and inverted position. 4 Takakura et al. classified ankle OA into several stages, especially 2 and 3a involving the medial ankle compartment. 5 In other perspectives, medial ankle OA could be classified into two subtypes: translation type and tilt type.6,7 The translation type was described as the shifting of the talus to the medial side, further narrowing the medial ankle joint space.6–9 On the contrary, the tilt type could be characterized as the tilting of the talus in an incongruent varus position, which was defined as incongruent varus ankle OA in this study. The main surgical treatment options for end-stage ankle OA might be ankle arthrodesis or total ankle replacement arthroplasty. 10 Although, in an earlier stage of OA, promising results have been reported after a realignment surgery such as a supramalleolar osteotomy,11–13 incongruent varus ankle OA with a large talar tilt is difficult to salvage.12,14
Recently, talofibular bony impingement has been postulated to be a source of ankle pain. 15 The impingement caused the limitation of ankle dorsiflexion, and only after removal of the bony impingement did the range of dorsiflexion increase and functional score improve. In addition, bony impingement between the talus and fibula has been considered as one of the causes of a block to the stable reduction of the ankle joint during ankle replacement surgery.16,17 As such, not only is preoperative evaluation of the osteophytes at the lateral gutter important, but also the resection of any obstruction is the key to successful operation. In our experience, it was interesting to observe unilateral varus ankle OA patients with a different talar tilt on each side and that the lateral gutter was more crowded with osteophytes on the affected side. However, the reason the talar tilt is increased and its association with concomitant talofibular space narrowing has not been sufficiently documented.
Thanks to the development of weightbearing computed tomography (CT) examination, a variety of foot and ankle alignments have been evaluated in a more physiologic situation, leading to the addition of some clinical perspectives on the malalignment of the foot and ankle. 18 Therefore, we thought that the relationship between increased talar tilt and talofibular space narrowing could be investigated by comparing weightbearing CT images with normal controls. To reduce the variations in individuals, setting the contralateral side as a reference would be the best option for comparison. To the best of our knowledge, no previous studies have performed bilateral weightbearing CT in patients with unilateral varus ankle OA with control of the contralateral ankle with normal alignment.
This study aimed to evaluate the relationship between talofibular impingement and increased talar tilt in incongruent varus ankle OA patients using bilateral weightbearing CT.
Materials and methods
This study was designed as a retrospective, level IV case series. This research was approved by our institutional review board. Informed consent was waived because of the retrospective nature of the study.
A total of 81 patients who visited our outpatient clinic with unilateral varus ankle OA between May 2015 and April 2019 were included. Patients (1) who had undergone any previous surgery, (2) already had non-weightbearing CT scans, and (3) refused to undergo a weightbearing CT were excluded. As a result, 30 patients who underwent bilateral weightbearing CT scans and plain radiographs were included in this study. Of the total patients, 11 were males and 19 were females. The mean age of the study patients was 63.8 (range: 47–76 years). Incongruent varus ankle OA was defined as a talar tilt of more than 4° in a standard weightbearing ankle anteroposterior (AP) radiograph, as described in previous studies.7,19 A talar tilt of more than 10° was regarded as severe, while a talar tilt of less than 10° was considered as mild to moderate for analyzing the relationship between an impingement and the degree of talar tilt. The side with normal alignment was used as the control.
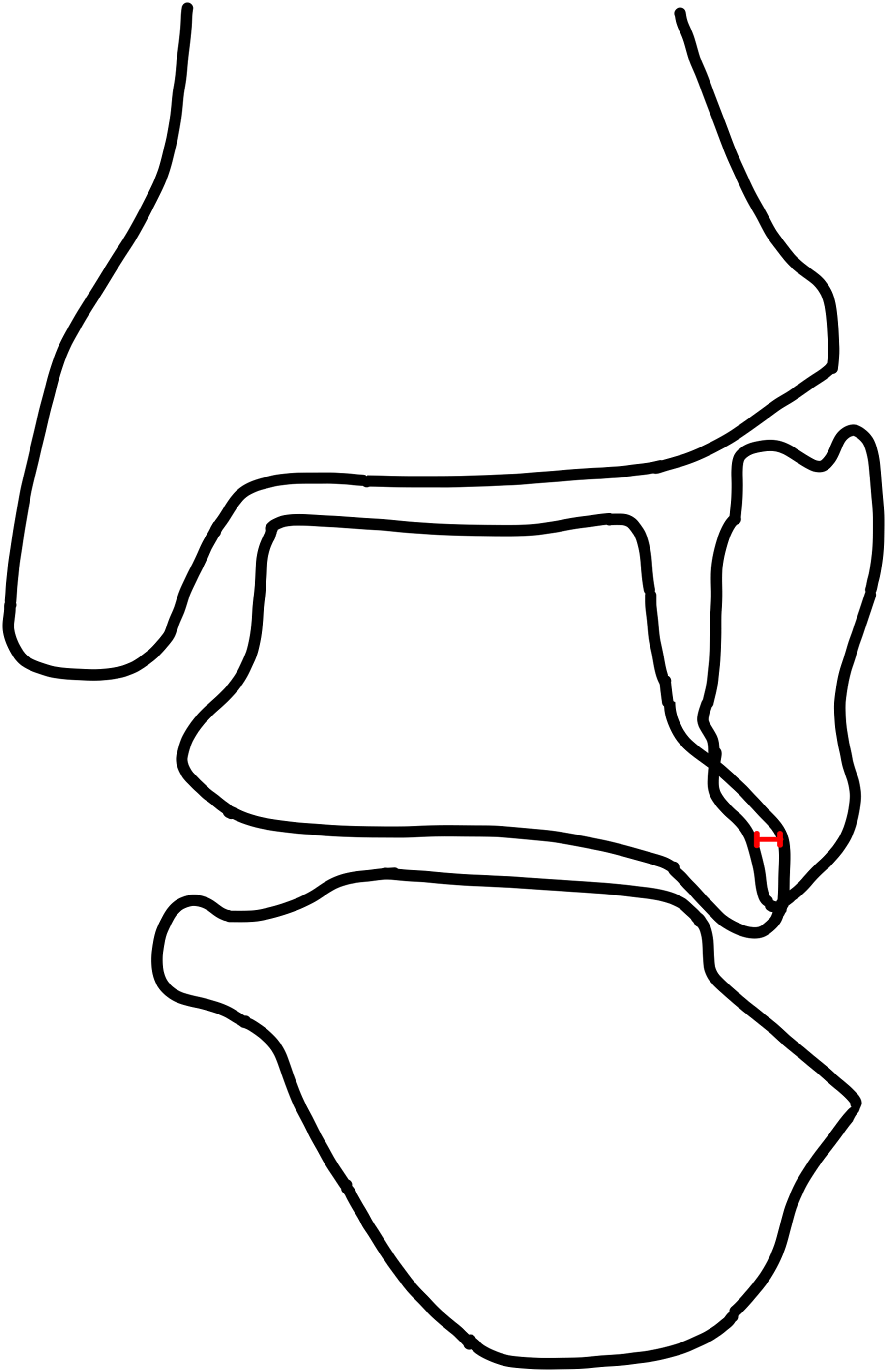
Talar tilt (Figure 1) and the closest distance between the talar lateral process and lateral malleolar tip (Figure 2) were measured from a plain standing ankle AP radiograph on both sides. On the coronal view of a weightbearing CT, the presence of spur at the lateral malleolar tip and talar lateral process was assessed (Figure 3). On the axial view of a weightbearing CT, the presence of spur at the talar lateral process was assessed, and spur protrusion length was measured (Figure 4).20,21 Measurement of the talar tilt angle. Unilateral varus ankle osteoarthritis with a talar tilt. We measured the closest distance between the talar lateral process and the fibular tip on both sides. Coronal view of weightbearing CT shows a spur on the talar lateral process and the tip of the fibula (arrows). Axial view of weightbearing CT shows the length of talar spur protrusion.



To assess for the presence of talofibular bony impingement and prove its role in hindering talus reduction, talofibular overlap was simulated using coronal images of weightbearing CT with Photoshop CC (Adobe, California, USA) software. The measurement of the talar tilt in the control side was set as a reference, and the simulation was performed by rotating the varus side’s talus to the talar tilt of the contralateral side. The length of the talofibular overlap was calculated using Image J software (National Institutes of Health, Maryland, USA) (Figures 5–7). Coronal view of weightbearing CT shows unilateral varus ankle OA with increased talar tilt. This illustration shows talofibular configuration before the simulation (left). The representative simulated image (right) was made by rotating the varus side’s talus in amount to the contralateral side’s talar tilt. This illustration shows the talofibular overlap of which the length was calculated.

The radiographic parameters were evaluated by two orthopedic surgeons with experience of minimum 4 years, and intraobserver and interobserver reliabilities were obtained.
Statistical analyses were performed using SPSS Statistics 25 (IBM, New York, USA). The Shapiro–Wilk test was used to determine the normal distribution of the data. Fisher’s exact test was used to compare categorical data between the varus and control sides. An independent t-test was used to compare the differences in continuous data between the two sides. Statistical significance was set at p < .05. For interobserver and intraobserver reliabilities, Cohen’s kappa coefficient was used to determine the frequency of categorical data, while the intraclass correlation coefficient was used to analyze continuous data.
Results
Interobserver and intraobserver reliabilities of radiographic measurements of both sides.

Values are presented as intraclass correlation coefficients (95% confidence interval).
Interobserver and intraobserver reliabilities of frequency of spur of both sides.

Values are presented as kappa (coefficient of agreement for chance).
Comparison of radiographic parameters between the varus and control sides.

On the axial images of weightbearing CT, talar spur was present on the varus side in all 30 patients. Spur protrusion length was significantly greater on the varus side with 2.98 mm (range: 1.33–4.37) compared with 1.67 mm (range: 0.87–2.58) of the contralateral side (p < .001). On the coronal images of weightbearing CT, the spur of the talar lateral process and lateral malleolar tip was present on the varus side in 29 and 28 patients, and on the contralateral side in eight and three patients, respectively.
Number of patients in each subgroup according to talofibular overlap length on the varus side.

Discussion
In this study, we analyzed the relationship between talofibular impingement and increased talar tilt and found that increased talar tilt in varus ankle arthritis might be related to possible impingement of the talofibular joint space, contrary to the contralateral ankle with normal alignment.
Varus ankle OA is not infrequent and, in some reports, half of the patients had varus malalignment at the time of end-stage ankle OA. 22 Varus ankle OA has two kinds of morphological features: translation and tilt. 6 While varus ankle arthritis with large varus talar tilt is thought to be difficult to treat, the cause and proper correction method has not yet been elucidated.12,14 Possible reasons for this include subtalar orientation, lateral ankle instability, and abnormal talar internal rotation. 23 Krähenbühl et al. reported that the subtalar joint orientation may be a risk factor for the development of ankle OA. 24 They evaluated the orientation of the posterior facet of the subtalar joint using subtalar vertical angle, which was significantly low in varus ankle OA. In contrast, Hayashi et al. reported that valgus inclination of the subtalar joint as a compensatory function increased progressively until stage 3a and then decreased to stage 4. 25 According to Kim et al., the abnormal internal rotation of the talus generates a stretching force acting on the anterior talofibular ligament, leading to aggravation of varus ankle OA and reduction of the contact area of the ankle. 19
Recently, the concept of talofibular impingement in patients with limited ankle dorsiflexion has been reported. 15 Other studies have reported that the distance between the talar lateral process and fibular tip was significantly shorter in the impingement group, and talofibular articular impingement was associated with an increased demand for operative treatment in patients with ankle instability.15,26 From our results, we hypothesized that the lateral bump of the talus to be overlooked in the radiographs may prevent the talus from being reduced in an ankle mortise as a cause of talofibular impingement in patients with incongruent varus ankle OA. In a previous study by Lee et al., impingement of the talofibular space by the ossicle resulted in chronic pain and functional varus instability in patients with os subfibulare. 26
The most important finding in this study is that incongruent varus ankle OA, which is over 4 degrees of talar tilt, is frequently associated with concomitant talofibular impingement at the lateral gutter. Moreover, the extent of simulated talofibular overlap tended to be larger in the severe talar tilt subgroup. When we think of a possible mechanism of lateral talofibular osteophyte formation, a lateral spur may develop from stretching or traction as a result of chronic varus tilt. 15 However, according to Tol and van Dijk, stretching of the ligament as a cause of spur development may not be plausible. 27 Although a definite causative relationship, whether chronic varus tilt leads to the formation of lateral osteophytes or vice versa, is still unknown and further study would be needed; in this study, we focused on the “presence” of possible impingement (if the talus is reduced from increased tilted position) of talofibular joint in incongruent varus ankle OA patients.
The bony impingement between the talus and fibula is thought to be one of the causes of obstruction to the stable reduction of the ankle joint during total ankle replacement arthroplasty.16,17 The lateral gutter of the ankle joint should be inspected, and aggressive gutter debridement is required to achieve neutral ankle mortise; otherwise, osteophytes will prevent the complete reduction of the talus. According to Saiga et al., when performing arthroscopic ankle arthrodesis in patients with varus ankle OA, lateral gutter osteophyte resection led to the correction of the varus ankle deformity. 28 Therefore, the simulation performed in our study supports the idea that talofibular impingement is closely related to increased talar tilt, and lateral gutter clearing is important.
This study has several strengths. First, even with a small retrospective cohort of 30 patients, the study data included weightbearing CT images of both ankles of the respective individuals. In this method, the contralateral side was used as an age- and sex-matched reference, reducing inter-individual variations and making this a well-designed study. A similar method of setting the non-OA side as a baseline and comparing each other in unilateral varus ankle OA has been described in a recent study. 29 This method of comparison was also regarded as a way of eliminating large inter-individual variabilities. Second, together with simple radiographs, weightbearing CT images provided sufficient data on the characteristics of a bony spur. Weightbearing CT scanners provide images of patients in physiologic standing situations. This powerful technology has improved sensitivity for assessment of bony impingement, forefoot and hindfoot alignment, and joint space narrowing. 18 With the advancement of technology, this study was able to assess the length of an axial spur protrusion and provide simulation data with the coronal images of the patients’ physiologic condition.
This study also has several limitations. First, the methodology we used could only be applied to patients with unilateral varus ankle OA, wherein the unaffected side is used as a reference for simulation. However, aside from the methodology, the overall results of our study would provide a basic rationale to clear lateral gutter osteophytes for correction of an incongruent talar tilt during corrective osteotomy or ankle replacement surgery in incongruent varus ankle OA cases. Second, our study simulated the talofibular overlap in two dimensions. A previous study showed that the talus tends to be internally rotated in patients with severe varus ankle OA. 19 This factor needs to be taken into consideration in calculating the actual talofibular overlap area. However, our study sufficiently showed significant overlap on the varus side in all patients. We believe that the talofibular overlap will be greater in three dimensions. Lastly, the clinical implications of talofibular impingement on increased talar tilt remain unclear. Further follow-up studies are needed to clinically elucidate whether excision of bony impingement results in good alignment.
Conclusion
Talofibular impingement by lateral gutter osteophytes is closely related to increased talar tilt in patients with incongruent varus ankle OA. This impingement may prevent the correction of the talar tilt and hinder the talus from maintaining a neutral position. Therefore, lateral gutter osteophytes should be resected to stabilize mortise and improve clinical outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (NRF-2017M3A9E2063104) from the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Ministry of Science & ICT, Republic of Korea.
Ethical approval
The research ethics was approved by the Seoul National University Hospital Institutional Review Board (IRB number: H-2012-019-1177).