
Abstract
Background
Strayer’s gastrocnemius recession is a common technique in treating ankle equinus of gastrocnemius origin. Nevertheless, this technique is associated with a few flaws. We aim to introduce a novel technique of isolated gastrocnemius recession and perform a cadaveric study to evaluate its safety and at the same time compare this novel technique with the existing Strayer procedure biomechanically.
Methods
Eight fresh cadaveric models of gastrocnemius tightness were established by isolated traction of the gastrocnemius muscles. Gastrocnemius recession was performed on all eight models with Strayer method and the novel method randomized equally. The safety of both the techniques was evaluated by identifying any iatrogenic injury to the surrounding structures. The lengthening and improvement of the ankle dorsiflexion was measured and compared between the two techniques.
Results
There was no iatrogenic sural nerve or saphenous vein injury in all eight models. There was no significant difference between the two techniques in terms of lengthening (24.25 mm vs 21.00 mm; p = 0.838) and improvement of ankle dorsiflexion (26.5° vs 26°; p = .829).
Conclusions
Both Strayer technique and the novel technique of gastrocnemius recession lengthened the gastrocnemius and improved the ankle dorsiflexion in this cadaver trial. Both procedures were safe with proper techniques, and there was no significant difference in efficacy between them.
Level of Evidence
Level II, randomized controlled trial.
Introduction
Since human has adapted to a bipedal gait evolutionally, the foot serves as a paramount tool, allowing human to walk, run, and jump. 1 The ankle joint, serving as an intermediate between the leg and the foot, facilitates the distribution of weight evenly to the foot by active and passive dorsi- and plantar-flexion during different phases of gait. 2 Problems arise when the foot is fixed in an equinus position, owing to a variety of etiologies, including congenital anomaly, neurological problems, fractures, soft tissue injuries, or joint diseases.3–9 Ankle equinus of soft tissue origin, specifically of the superficial posterior compartment of the leg, has been extensively studied for the past three decades, leading to more understanding of the cause and effect of the equinus, and subsequently development of newer surgical techniques to correct it.8,10–13
Soft tissue ankle equinus can be precipitated by tightness of the gastrocnemius muscle, soleus muscle, Achilles tendon, or a combination of all.10,13,14 Surgical treatment should be individualized to the underlying pathology to obtain the best functional outcome. Equinus secondary to Achilles tendon stiffness can be remedied by performing Achilles tendon lengthening, while a gastrocnemius recession can be utilized to treat an equinus due to isolated gastrocnemius tightness.15–20 Gastrocnemius recession can be performed via an open technique, as well as endoscopically at multiple levels.16,20 The levels of gastrocnemius recession are normally named after the authors who have invented the techniques, such as Silverskoild, Barouk, Abbassian, Baumann, Strayer, Vulpius, Baker, Hoke, and White, each having their own pros and cons (Figure 1).21–25 On top of treating the ankle equinus, gastrocnemius recession has been used with success in treating other conditions such as pes planus, plantar fasciitis, metatarsalgia, Haglund’s deformity, and foot ulcers.7,10,18,26 Despite showing good outcomes in correcting isolated gastrocnemius tightness, gastrocnemius recession is sometimes associated with iatrogenic sural nerve injury, weakness of plantar flexion and overlengthening, leading to excessive dorsiflexion of the ankle.17,27,28 Diagram shows anatomical landmarks on the gastrocnemius–soleus complex and different lengthening procedures in each zone.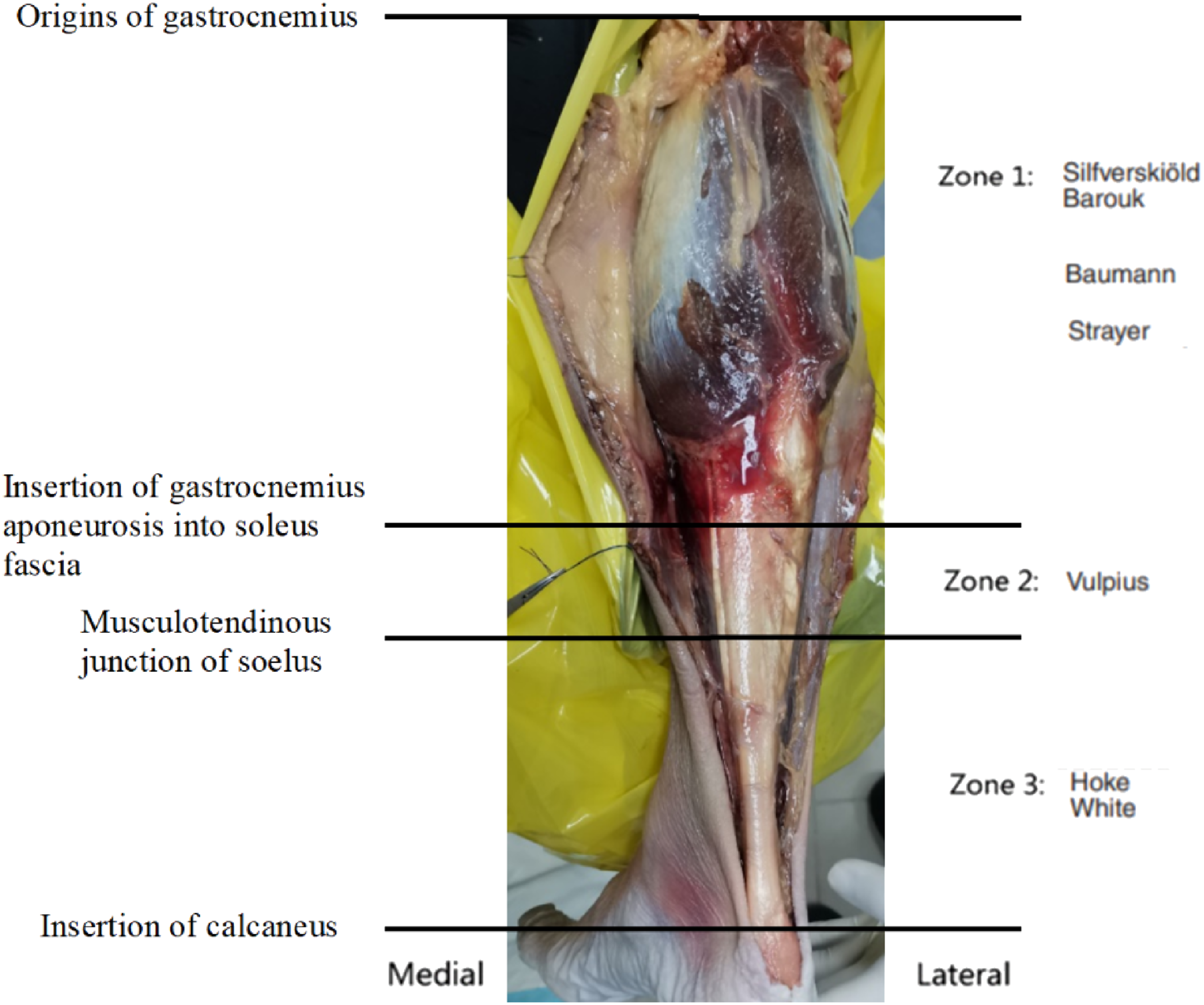
Realizing these complications behind the technique of gastrocnemius recession, we introduce a novel technique of gastrocnemius recession, modifying the existing Strayer procedure to overcome the complication of plantar flexion weakness and overlengthening. We perform a cadaveric study to determine the safety of this procedure, as well as to compare this novel technique with the existing Strayer procedure biomechanically.
Materials and methods
In this study, a novel gastrocnemius recession technique was developed, and its safety and effectiveness were evaluated and compared with the Strayer technique. This study was approved by the Kulliyah of Medicine Research Committee (KRC) (IIUM/305/20/4/1/7).
Sample size calculation
Sample size calculation was done by using Power and Sample Size Calculation version 3.1.6, October 2018. Based on the study by Rong et al., gastrocnemius recession via the Strayer procedure significantly improved (p < .05) the dorsiflexion angle of the ankle compared with the Barouk procedure and Bauman procedure with one cut. 29
In our study, we aimed to conduct a study to identify the outcome of ankle dorsiflexion improvement from the novel technique with the Strayer procedure acting as a control for each experiment subject. In the study by Rong et al., the improvement of the ankle dorsiflexion was normally distributed with a standard deviation of three and the ankle dorsiflexion improvement were 14.8°, 11.6°, and 22.4° for Barouk procedure, Baumann procedure with one cut and Strayer procedure, respectively. 29 With the minimal difference of 7.6° (22.4° vs 14.8°), a study containing four experimental subjects (novel technique) and four control subjects (Strayer procedure) was needed to be able to reject the null hypothesis that the mean of the ankle dorsiflexion angle of the experimental and control groups was equal to the probability (power) of 0.8 (80%). 29 The type I error probability associated with this test of the null hypothesis was 0.05.
Specimens’ Preparation and Biomechanic Setting
Eight through-knee–amputated lower limb cadaveric samples were procured. All these fresh-frozen cadavers were thawed at 4–7° for 72 h prior to the biomechanical study. Steps of preparation and setting of the cadaveric model are demonstrated in Figure 2. In order to simulate isolated gastrocnemius tightness, the gastrocnemius was separated from the soleus at the knee region. After isolating the gastrocnemius muscle, two-fold sutures were applied to evenly distribute the pulling force across the gastrocnemius muscle. First, both the medial and lateral heads of gastrocnemius were sutured continuously with an Ethibond one suture, thus ensuring the pulling force to be evenly distributed along the sutures to the muscle bellies. Next, three thick threads were anchored to the medial head, lateral head, and both medial and lateral heads of the gastrocnemius, with ends of the treads tied to the base of the model. The threads were then pulled until an ankle equinus of 20° was achieved, and the threads were then fixed at a proximal metal plate. In contrast to a formaldehyde-induced ankle equinus, our technique was more superior as the ankle equinus can be standardized to eliminate the confounding factor of varying starting equinus, while preserving the original muscle composition and stiffness. Preparation and setting of specimens. (a) Fresh-frozen through-knee lower leg cadaver is thawed over 72 h. (b) The skin and subcutaneous tissue are carefully incised to reveal the superficial posterior compartment of the leg. (c) Gastrocnemius muscle bellies (anchored with suture) are separated from the soleus muscle. (d) The isolated gastrocnemius muscles are then fixed to the metal plate proximally with three threads. Pulling forces are applied proximally to induce gastrocnemius equinus. (e) The ankle equinus is checked after the fixation of proximal threads to ensure a minimum of 20-degree ankle equinus is achieved.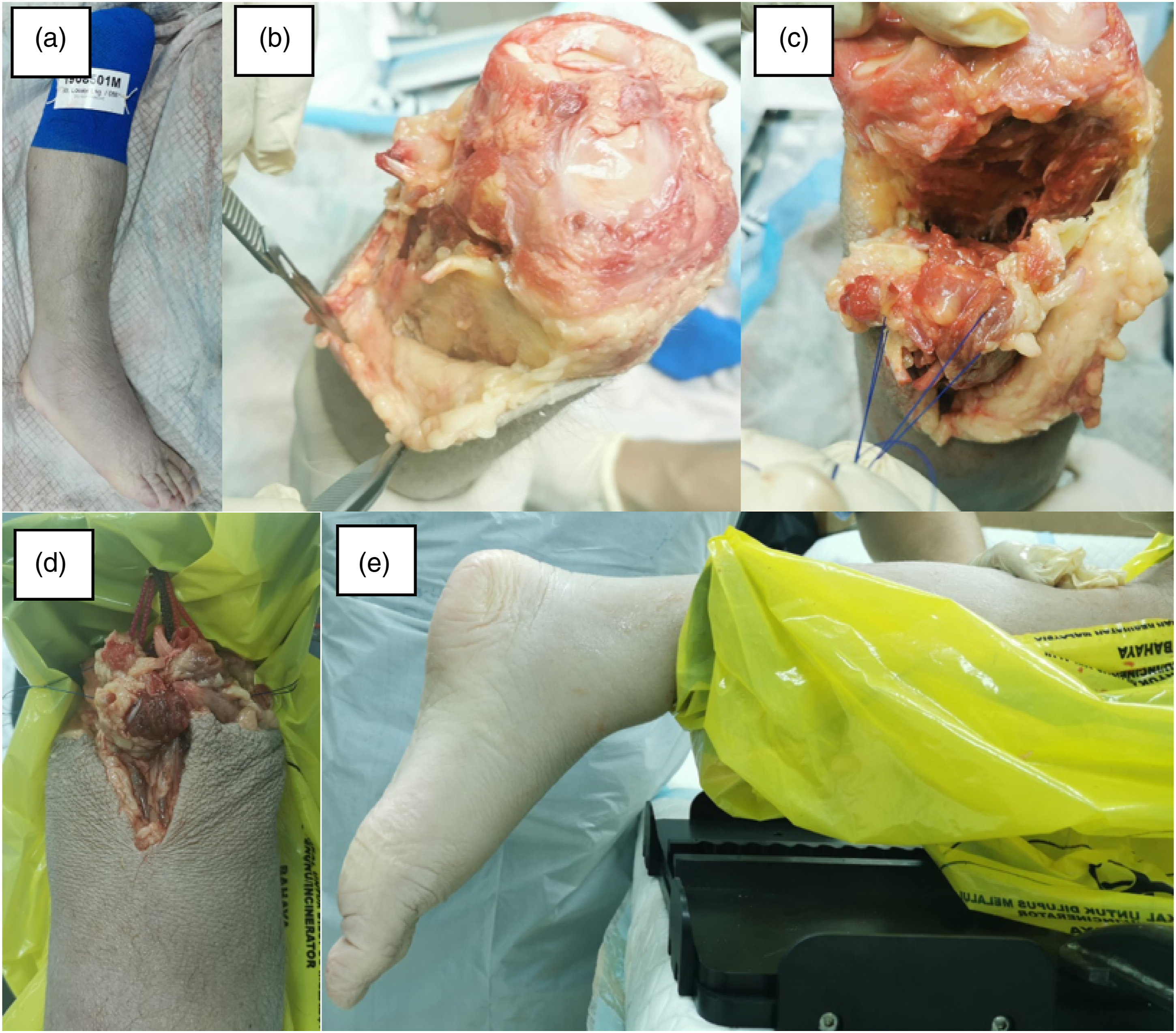
In order to compare the effectiveness of the novel technique with the original Strayer gastrocnemius recession, a validated biomechanical testing protocol was needed. The tried and tested protocol used by Rong et al., Firth et al., and Tinney et al. was employed.22,29,30 In their studies, both Firth et al. and Tinney et al. applied increasing dorsiflexion forces to the metatarsal head using a torque dynamometer at 10 kg increments from 0 to 40 kg on the embalmed cadavers and the lengthening of the gastrocnemius measured (Figure 3(a) and (b)).22,30 A maximum of 40 kg dorsiflexion force was applied, as a force higher than 40 kg would lead to tibial fracture.
30
Meanwhile, by using a similar method, Rong et al. only administered 2 kg increments from 0 to 10 kg on fresh frozen cadavers.
29
By using fresh frozen cadavers, soft tissue condition was best preserved, thus preventing up to five-fold increase in stiffness secondary to cross-linking of collagens in the embalmed cadavers.
29
Biomechanical testing protocol. (a) The ankle is set at equinus position. (b) A dorsiflexion force is applied by using a handheld digital dynamometer by an assistant. (c) A 3 cm skin incision is made at the medial side of the midpoint of the fibula. (d) Upon blunt dissection of the subcutaneous tissue, the gastrocnemius fascia is identified and incised to reach the gastrocnemius muscle.
In our study, with all the cadavers set at a minimum of 20-degree ankle equinus, both the novel technique and Strayer gastrocnemius recession were done from a medial approach. By using the midpoint of the fibula as a guide, a 3 cm longitudinal skin incision was made at the medial side. The subcutaneous fat was bluntly dissected to reveal the underlying gastrocnemius fascia. The gastrocnemius fascia was incised with a pair of scissors to identify the gastrocnemius–soleus complex. The gastrocnemius bellies were separated from the soleus by finger dissection. Upon separation of the soleus muscle, gastrocnemius recession was made from the medial to the lateral aspect.
After performing either the novel technique or the Strayer gastrocnemius recession, the dorsiflexion force applied onto the metatarsal heads was increased from 0 kg to 10 kg with an interval increment of 2 kg, measured by using a handheld digital dynamometer. The range of motion of the ankle and the gastrocnemius lengthening were measured at each 2 kg increment and the same protocol was used for both the novel technique and the Strayer gastrocnemius recession. In order to reduce bias, the measurements were collected by an independent radiology registrar. All the readings were recorded for analysis.
Upon achieving the maximum dorsiflexion force of 10 kg or the maximum dorsiflexion of 20°, the lengthening distance of the gastrocnemius muscle and the dorsiflexion improvement angle were documented. The mean of the four tests, each from the novel technique and the Strayer technique, were documented and compared using Student t-test, provided they were normally distributed.
Results
In both the novel and Strayer techniques of gastrocnemius recession, a mini-open approach was adopted, in which a 3–4 cm vertical skin incision was made at the medial part of the leg, corresponding to the fibula bisecting line (Figure 3(c) and (d)). As the sural nerve is in close proximity, there is a theoretical risk of sural nerve injury by using this approach.
31
Taking into consideration that the sural nerve is a subcutaneous nerve, we minimized sural nerve injury by blunt dissection and by subcutaneous tissue retraction after the skin incision. We did not routinely search for the sural nerve as it might be invariably injured when it was identified. Instead, the bulk of subcutaneous tissue was retracted away from the surgical field using retractors to avoid its injury. Aside from retracting with the retractor, we kept the scissors closed to the gastrocnemius muscle belly during the gastrocnemius recession, thereby avoiding cutting the sural nerve which traversed within the subcutaneous tissue. Indeed, in all eight gastrocnemius recessions using this mini-open technique, we encountered no sural nerve or small saphenous vein injury (Figure 4(c)). (a) The posterior compartment of the leg is explored prior to application of dorsiflexion force. (b) The lengthening of the gastrocnemius and ankle range of movement is measured at different dorsiflexion forces up to 10 kg. (c) The sural nerve (yellow arrow) and small saphenous vein (blue arrow) are checked to determine their patency.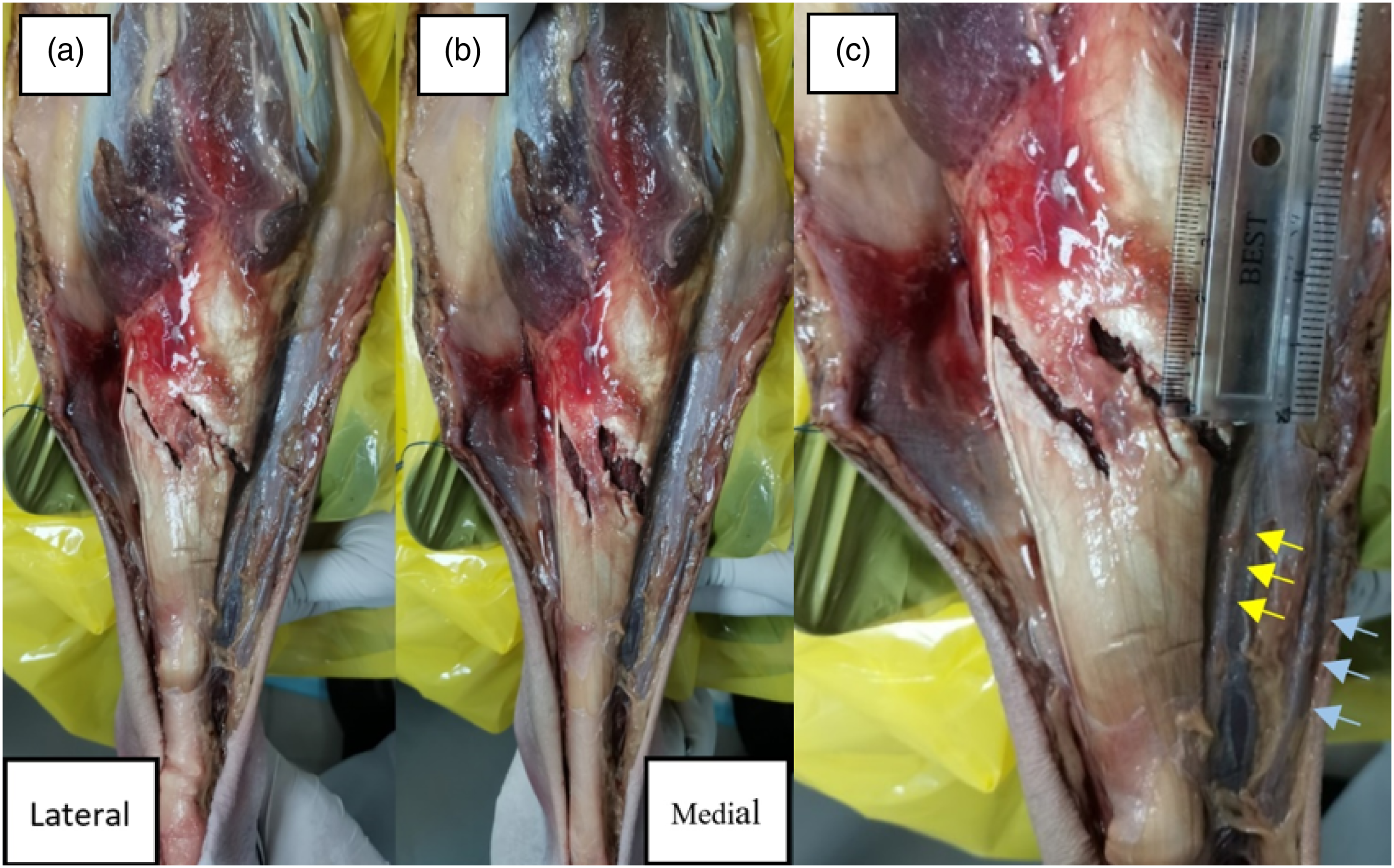
In consistent with previous study by Rong et al., gastrocnemius recession with Strayer technique was stable and progressive with increasing dorsiflexion forces (Figure 5).
29
Lengthening of the gastrocnemius muscle started at 4 kg dorsiflexion force onward and achieved maximum lengthening at 10 kg dorsiflexion force. Similarly, gastrocnemius lengthening after the novel technique of gastrocnemius recession exhibited the same pattern as the Strayer technique. Next, the mean of lengthening and ankle range of movement improvement with both Strayer technique and novel technique of gastrocnemius recession were assessed to determine the existence of any difference. Lengthening-force table of both Strayer and novel techniques of gastrocnemius recession shows progressive lengthening of gastrocnemius muscles with increasing dorsiflexion forces at 4 kg force onward.
The data obtained was assessed to determine data normality, a pre-requisite for independent t-test. The Shapiro–Wilk test was selected due to the small sample size (<50 samples). All the Sig values were more than 0.05, demonstrating that the data was normally distributed.
The improvement of ankle range of motion and lengthening after gastrocnemius recession, both using Strayer technique and the novel technique, were progressive until dorsiflexion force of 10 kg (Figures 6 and 7). The mean gastrocnemius lengthening of 24.25 mm (SD = 3.304) was achieved at 10 kg force and ankle dorsiflexion increased by 26.5° (SD = 2.828), with a ratio of 1.09° per mm. By utilizing the novel technique of gastrocnemius recession, we obtained a mean gastrocnemius lengthening of 21 mm (SD = 2.582) and 26° (SD = 2.828) of ankle dorsiflexion improvement, with a ratio of 1.24° per mm. There was no significant difference between the Strayer procedure and the novel technique of gastrocnemius recession for both muscle lengthening (p = .838) and dorsiflexion improvement (p = .829). Comparison between the Strayer procedure and the novel technique of gastrocnemius recession. At 10 kg dorsiflexion force, the improvement of ankle range of movement is 26.5° (SD = 2.517) and 26° (SD = 2.828) for Strayer procedure and the novel technique respectively. There is no significant difference between the two techniques (p = .829). Comparison between Strayer procedure and the novel technique of gastrocnemius recession. At 10 kg dorsiflexion force, the gastrocnemius lengthening is 24.25 mm (SD = 3.304) and 21 mm (SD = 2.582) for Strayer procedure and the novel technique, respectively. There is no significant difference between the two techniques (p = .838).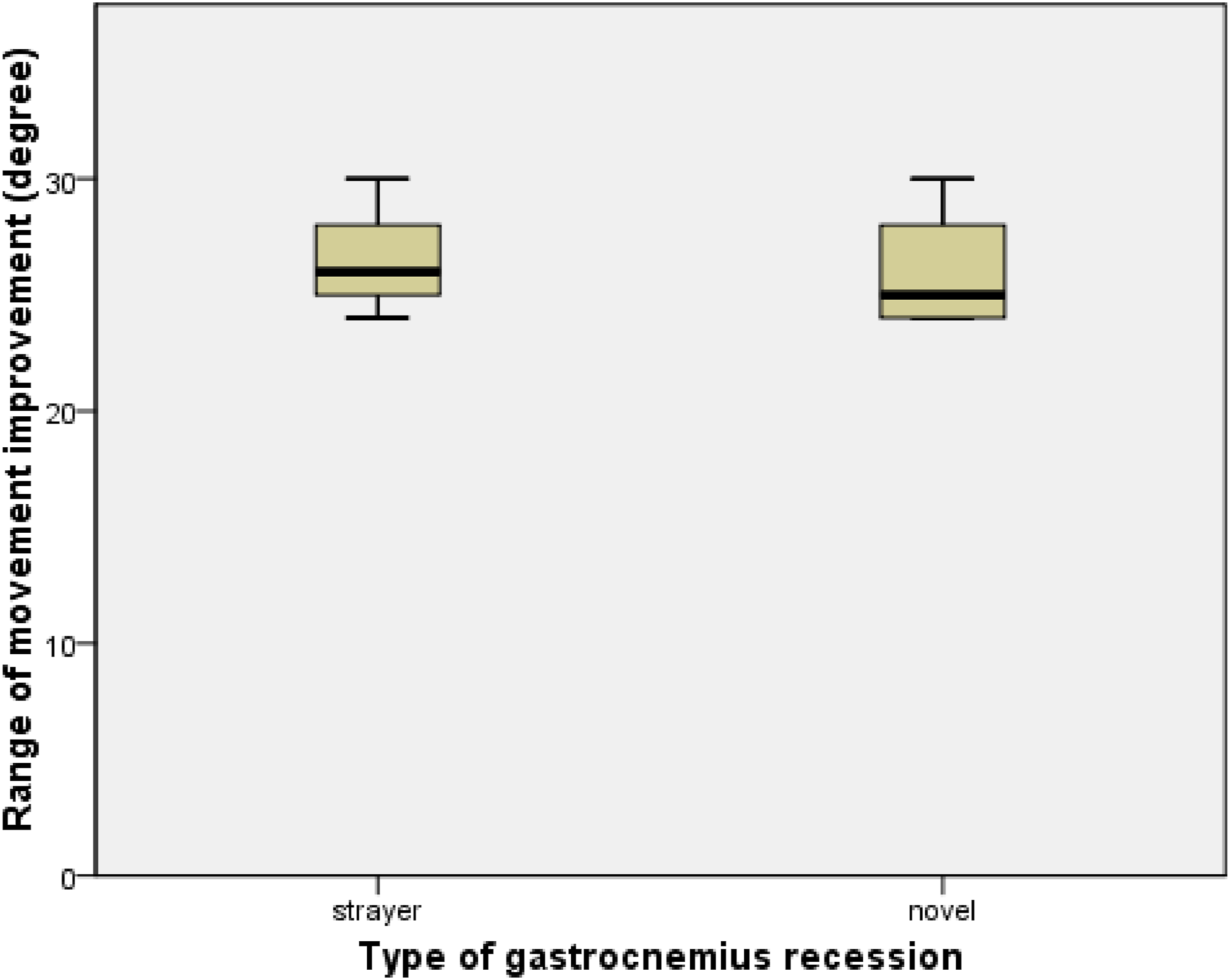

Discussion
Cadaveric preparation and biomechanical setting
Cadavers are classified based on the method of preservation, namely embalmed and fresh-frozen cadavers. 32 A study by Wilke et al. mentions that soft tissues of embalmed cadavers are hardened in the formaldehyde solution. 33 There is five-fold increase in stiffness of cadaveric soft tissues in these embalmed specimens, indicating that they are not ideal in replicating an in-vivo condition. 33 Furthermore, the thickness of soft tissue specimens, time of diffusion and time of fixation will all directly affect the diffusion and distribution of the formalin solution, leading to variable soft tissue stiffness. 34 Although embalmed cadavers are suitable for bony procedure studies in view of the unchanged histological structure, mineral composition, and bone density, they are not suitable for soft tissue biomechanical studies as the soft tissue composition is changed owing to cross-linking of proteoglycans monomers. 33 Some authors utilize formaldehyde to induce soft tissue equinus in the cadavers, but this technique is not feasible in emulating an isolated gastrocnemius stiffness as the whole gastrocnemius–soleus complex will be shortened in embalmed specimens.22,29,30 Therefore, taking into consideration the aforementioned reasons, fresh-frozen cadavers are chosen for this study.
In order to emulate an isolated gastrocnemius contracture, Rong et al. capitalize the benefit of gastrocnemius’ two joint-spanning anatomical structure and apply a spacer at the knee region to elevate and tighten the gastrocnemius without affecting the soleus muscle. 29 This is not feasible in our study as cadavers that we have procured are all through-knee specimens, with medial and lateral gastrocnemius heads being severed. We manage to simulate isolated gastrocnemius contracture by applying traction force through isolated medial and lateral gastrocnemius proximal bellies. In contrast to a formaldehyde-induced ankle equinus, our technique is more superior as the ankle equinus can be standardized to eliminate the confounding factor of varying starting equinus, while preserving the original muscle composition and stiffness.
For the model to produce a consistent level of isolated gastrocnemius tightness, the pulling load of gastrocnemius heads needs to be equal and well-distributed. In our model, we utilize two-fold sutures to evenly distribute the pulling force across the gastrocnemius muscles. By increasing the pulling force via the thread across the base plate, gastrocnemius muscles are being pulled along until a 20-degree ankle equinus is achieved. Our model is comparable to the one developed by Rong et al., as evidenced by similar progressive lengthening with increasing dorsiflexion forces from 4 kg to 10 kg after gastrocnemius recession with Strayer technique. 29 Similar to the model by Rong et al., our model exhibits the advantage of controllable gastrocnemius equinus. 29 By increasing or decreasing the pulling force of the gastrocnemius thread, gastrocnemius equinus can be set at a desirable degree on all cadavers, making this comparative study more reliable. On top of that, our model has avoided drawbacks of the model by Firth et al., as we isolate and separate the soleus muscle from the gastrocnemius muscle, to achieve an isolated gastrocnemius tightness. 30
Gastrocnemius recession
The advantages and disadvantages of different techniques of triceps surae surgical lengthening can be attributed to the anatomic zones of intervention and principles involved. 30 In the aspect of surgical principle, there are intramuscular tenotomy (Baumann), muscular recession with aponeurosis lengthening (Strayer), aponeurosis and fascial lengthening (Vulpius), and multi-level Achilles tendon lengthening (White and Hoke).35,36 Due to the anatomical structure of triceps surae, isolated gastrocnemius tightness of different etiologies is best treated with zone 1 gastrocnemius recession procedures. As the soleus is pathology-free, it will be unwise to perform a zone 3 procedure (Achilles tendon lengthening) and increased risk of tendon rupture or overcorrection. 37 Similarly, a zone 2 procedure is relatively difficult as this zone is characterized by condensation of the gastrocnemius fascia and soleus fascia into the conjoined gastrocnemius aponeurosis-soleus fascia, making it difficult to separate those two fascia at this level. 30 Often, a sharp dissection, rather than a blunt dissection, is needed to separate the two fascia, hence increasing the risk of injury to surrounding vital structures such as the small saphenous vein and sural nerve. 37
Among different zone 1 gastrocnemius recession techniques, Strayer procedure is by far the most popular option, owing to its superiority in equinus correction, ease of the procedure and lower risk of skin-related complications. 38 Nevertheless, Strayer technique is occasionally associated with overcorrection and weak plantar flexion after the surgery, leading to an inefficient gait cycle. 38 The transverse cut at the distal musculotendinous junction of the gastrocnemius completely separates the gastrocnemius muscle from the Achilles tendon, with the proximal stump being anchored to the underlying soleus fascia at a distance (typically about 3 cm) with a suture.
Novel technique of gastrocnemius Recession
A novel technique, where the existing Strayer technique is modified, is introduced to overcome problems associated with the Strayer technique. Instead of a transverse cut at the musculotendinous junction, two 45-degree cuts are made from the medial to lateral aspect to separate the gastrocnemius muscles (Figure 4(a)). Through this technique, part of the gastrocnemius muscle is preserved, enabling retention of partial plantar flexion power. Besides that, with the remaining gastrocnemius muscle acting as a strut to resist excessive dorsiflexion forces, overcorrection of the equinus can be prevented. Despite being an “incomplete” cut, we postulate that it is effective against gastrocnemius-tightness–induced equinus of at least 15°, reasons being the remnant of the gastrocnemius “strut” is relaxed in an oblique manner and it can be stretched longitudinally by applying a dorsiflexion force.
One the complications of gastrocnemius recession is sural nerve injury due to the fact that the sural nerve runs between the two heads of gastrocnemius muscles from proximal to distal up to the mid-fibula where it courses laterally. 31 The site where the sural nerve courses laterally at the mid-fibula level is approximately 10 cm proximal to the calcaneal tuberosity. 39 Hoefnagels et al. propose to do the gastrocnemius recession proximally as the sural nerve is protected by the lateral head of gastrocnemius muscle. 31 Nonetheless, injury to the sural nerve is still possible due to the transverse incision made for gastrocnemius recession.
Our novel technique further reduces the risk of sural nerve injury by performing two oblique incisions instead of a transverse incision. This novel technique spares the area between the two heads of gastrocnemius where the sural nerve is commonly located. Anatomically, sural nerve normally lies close to the superficial fascia of the gastrocnemius muscle. 38 Before the gastrocnemius recession, a finger is inserted to separate the gastrocnemius muscle bellies from the superficial fascia, hence further reducing the risk of sural nerve injury.
Biomechanical study by Rong et al. shows that the Strayer technique of gastrocnemius recession provides the most lengthening and improvement of ankle dorsiflexion compared to other techniques of gastrocnemius recession such as Baumann and Barouk. 29 Therefore, the new technique should be on-par with the Strayer technique of gastrocnemius recession in terms of lengthening and improvement of ankle dorsiflexion. In this study, the lengthening of the gastrocnemius muscle is progressive with increasing dorsiflexion force after both the Strayer and the novel techniques of gastrocnemius recession. This is consistent with findings by Rong et al. 29 At the peak dorsiflexion force (10 kg), both lengthening and ankle dorsiflexion improvement do not have significant difference between the Strayer and the novel techniques of gastrocnemius recession. This result validates the novel technique of gastrocnemius recession as non-inferior to the Strayer technique.
There are several limitations in this study. Despite our best effort, we are not able to obtain paired cadavers to compare both techniques of gastrocnemius recession. Non-modifiable factors such as age and underlying co-morbidities may affect the quality of cadaveric muscles.
Conclusion
In conclusion, this cadaveric biomechanical study of the novel technique of gastrocnemius recession shows that it is safe and effective in the treatment of conditions associated with isolated gastrocnemius tightness.
Footnotes
Declaration of conflicting interests
All authors declare no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Universiti Malaysia Sabah Research Grant (SBK0452-2018).
Ethical approval
This study was approved by the Kulliyah of Medicine Research Committee (KRC) (IIUM/305/20/4/1/7).