
Abstract
Introduction
Venous thromboembolism (VTE) including deep vein thrombosis (DVT) and pulmonary embolism (PE) remains a problem after total hip arthroplasty (THA). 1 The perioperative chemoprophylaxis has been proved to reduce the rates of death and complications associated with VTE after THA.1,2 The careful balancing is advised between the risks of thromboembolism and generalized and local bleeding from pharmacologic prophylaxis, which may lead to reoperation and infection. The recommended pharmacologic therapy options for thromboprophylaxis after THA include low-molecular-weight heparins (LMWHs; e.g., enoxaparin), direct factor-Xa inhibitors (e.g., rivaroxaban), vitamin K antagonists (VKAs; e.g., warfarin), and so on. As a direct, oral anticoagulant, rivaroxaban is commonly prescribed for extended prophylaxis due to its advantage of easier administration, no need for monitoring, and increased or equivalent potency compared to classic anticoagulants. In the National Institute for Health and Clinical Excellence (NICE guidelines, rivaroxaban was recommended for thromboprophylaxis following lower limb arthroplasty for its comparable effectiveness as LMWH in preventing VTE. 3 However, during VTE prophylaxis following lower limb arthroplasty, compared with LMWH, rivaroxaban use was associated with a lower DVT rate at the expense of a higher rate of wound complications. 4 Moreover, a greater risk of surgical site hemorrhage, which can compromise functional outcome and increase the rates of blood transfusion, reoperation, and revision surgery, has also been reported.5,6
Prothrombin time (PT) and activated partial thromboplastin time (aPTT) are commonly used in assessing hemostatic function; however, they are performed on plasma and cannot assess the rate of clot formation, overall clot propagation, or degree of fibrinolysis or clot lysis. Besides, PT and aPTT present high specificity but lack sensitivity. 7 Thromboelastography (TEG) is a point-of-care blood test that measures the viscoelastic properties of the whole blood, and it can reflect a comprehensive overview of the clotting process, starting with fibrin formation, and continue through platelet aggregation and fibrinolysis. TEG is thought to be more sensitive than plasma-based clotting assays (PT or aPTT) for the detection of a hypercoagulable state in nonbleeding, burned, or nonburned trauma patients. 8 TEG can be an additional method of assessing the effectiveness of pharmacologic DVT prophylaxis in a patient population with high risk VTE complications. In Tekkesin et al.’s study, 9 the correlation between anti-Xa and TEG parameters was examined to monitor the anticoagulant activity of LMWHs in patients undergoing unilateral or bilateral total knee replacement. A significant correlation between coagulation index (CI) and plasma anti-Xa activity was demonstrated in these patients treated with enoxaparin.
We hypothesized that rivaroxaban may be more effective than enoxaparin for the prevention of VTE after THA, but comparisons with enoxaparin by means of TEG analysis are still lacking. The purpose of this study was to evaluate the anticoagulant effect by comparing routine coagulation assessment and TEG in patients treated with either rivaroxaban or enoxaparin as thromboprophylaxis after THA and to provide reference data for individualized anticoagulant therapy after the operation.
Materials and methods
Study participants
This prospective study was approved by the hospital’s ethics committee, and informed consent was obtained from each patient. From January 2017 to March 2019, all consecutive patients undergoing cementless unilateral primary THA were recruited in this study. Patients were eligible to participate in the study if they were aged 18 years or older. All patients were diagnosed with osteoarthritis or osteonecrosis of the femoral head. Patients were excluded if they (1) had hemorrhagic disease or a contraindication to anticoagulant prophylaxis, (2) had lower extremity DVT that was confirmed by preoperative color Doppler ultrasonography, (3) had a history of thromboembolic disease, anticoagulant therapy, or antiplatelet treatment, or (4) had a history of severe liver diseases, uncontrolled hypertension, clinically significant impairment of renal function, or any other organ insufficiencies. Two hundred and twenty-eight patients fulfilled the inclusion criteria and were randomly assigned into one of the two study groups according to a computer-generated random sequence. Rivaroxaban group comprised 114 patients (range, 42 males and 72 females) with a mean age of 61.2 years (range, 46–83). Enoxaparin group comprised 114 patients (51 males and 63 females) with a mean age of 61.9 years (43–82).
Perioperative management
All THAs were performed by the same senior surgeon using the posterolateral approach, under general anesthesia. Cementless stems and cups were used for all arthroplasties. Patients received intravenous infusion of 1 g of tranexamic acid 30 min before incision and 1 g of tranexamic acid 3 h later. A drainage tube was routinely placed prior to arthrotomy closure and removed 24 h after surgery. Blood transfusions were administered if the hemoglobin level was <7.0 g/dL or if any symptoms suggestive of anemia such as persistent tachycardia or hypotension in spite of adequate volume replacement. All patients were also managed comprehensive approach to postoperative care while in the hospital, including early mobilization with physical therapy and mechanical prophylaxis. Color Doppler ultrasonography of both lower limbs was performed in all patients 1 day before the surgery and 7 days after the surgery. Patients with DVT were further treated after consultation in the department of vascular surgery.
Patients in the rivaroxaban group received 10 mg of rivaroxaban (Xarelto, Bayer, Leverkusen, Germany) orally once daily. Patients in the enoxaparin group received 4000 AxaIU (0.4 mL) of enoxaparin (Clexane; Sanofi Corp, Paris, France) subcutaneously once daily. Rivaroxaban and enoxaparin were started 6–8 h after surgery. The administration of the anticoagulant prophylaxis lasted for a minimum of 14 days.
Thromboelastography and routine coagulation tests were performed on the day before the operation and 1 day and 7 days after the operation. Routine coagulation indexes include PT, aPTT, international normalized ratio (INR), thrombin time (TT), D-dimer, fibrinogen, and fibrin degradation products (FDP). Standard citrated kaolin-activated TEG tests were performed on a computerized TEG coagulation analyzer (TEG model 5000; Haemoscope Corporation, USA). TEG values include reaction time (R), K, α-angle, maximum amplitude (MA), and CI. R-time represents the time elapsed from the initiation of the test until clot firmness reaches an amplitude of 2 mm, meaning the initiation phase of coagulation and is functionally related to enzymatic clotting factors. K-time is the time from the end of R-time to 20 mm amplitude of clot formation, whereas α-angle is the angle which is formed by the slope of a tangent line traced from the R-time to K-time and horizontal. Both of them denote the speed of fibrin cross-linking and clot forming and were considered to be affected by the activity of the fibrinogen. MA is the greatest amplitude on the TEG tracing, which is a reflection of the platelet aggregation and maximum strength of the fibrin clot. CI is the final parameter calculated from the above parameters, indicating the overall coagulation function of patient. In the present study, normal range values were provided by the manufacturer. Reference ranges of our research were R (4–10 min), K (1–3) min, α-angle (53–72 ˚), MA (50–70), and CI (-3–3).
The primary safety outcome was the incidence of major bleeding beginning after the first dose of the study drug and up to 2 days after the last dose of the study drug. Major bleeding was defined as acute, clinically overt bleeding that was fatal , or occurred in critical organs (e.g., retroperitoneal, pericardial, intracranial, intraocular, and spinal cord bleeding), or required reoperation or significant bleeding in extra-surgical sites and associated with a fall in the hemoglobin level of at least 20 g/L. Minor bleeding events were defined as bruising or ecchymosis, incision hematomas, gastrointestinal bleeding, and other bleeding events that were not major events. The secondary safety outcome was wound complications (a composite of excessive wound hematoma, reported surgical-site bleeding, and postoperative wound infection).
Statistical analysis
The power analysis showed that the required sample size of the present study was 45 cases with a power of 90% at the 0.05 probability.
Continuous variables were expressed as means
Results
Patient baseline characteristics
Baseline characteristics of the two groups.

ASA: the American society of anesthesiologists.
Routine coagulation assessment
Routine coagulation assessment at different time points.

*p < 0.05; Preop: preoperation; POD1: 1day postoperation; POD7: 7days postoperation; FDP: fibrin degradation products; aPTT: activated partial thromboplastin time; PT: prothrombin time ; INR: international normalized ratio; TT: thrombin time.
Assessment of TEG
TEG assessment at different time points.
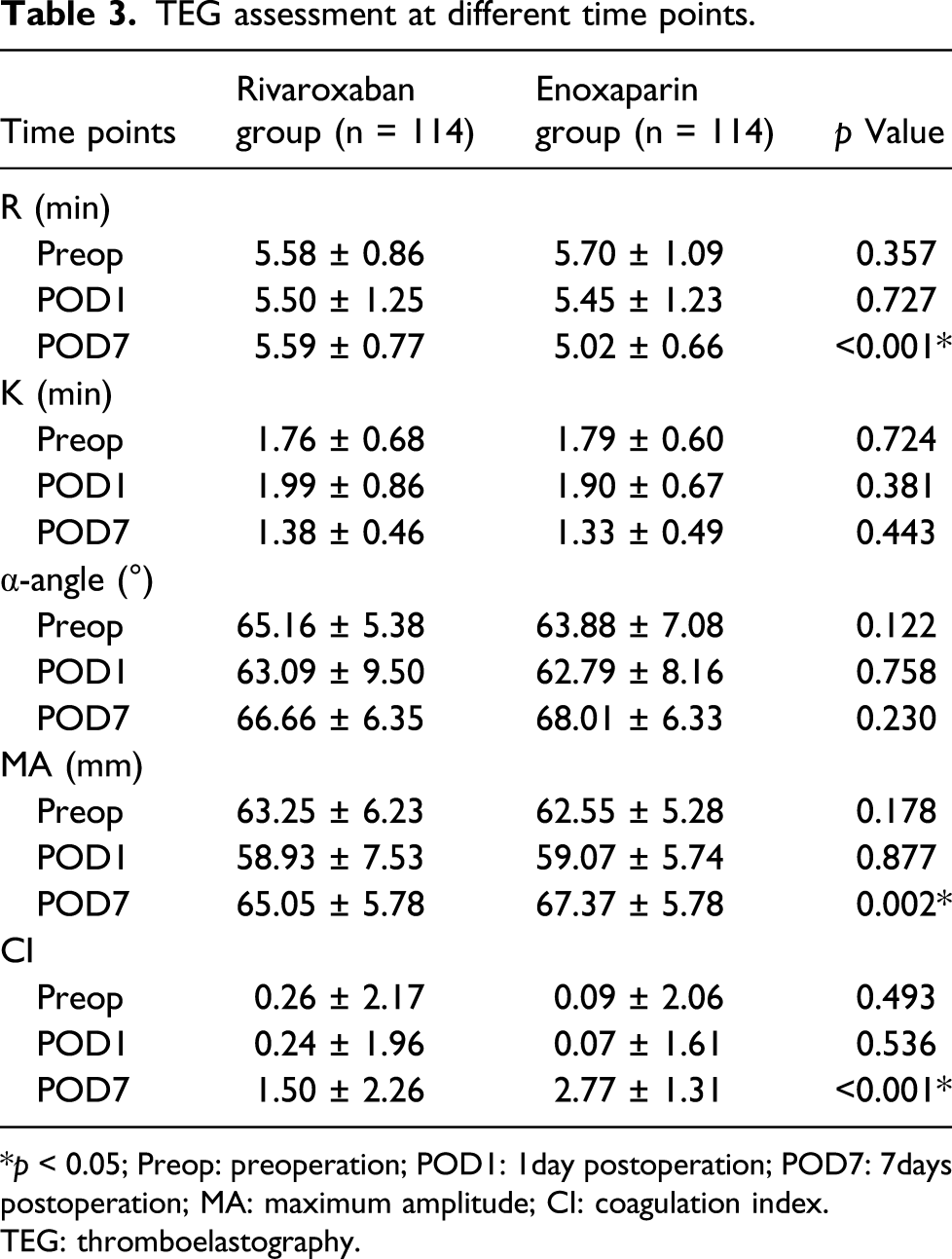
*p < 0.05; Preop: preoperation; POD1: 1day postoperation; POD7: 7days postoperation; MA: maximum amplitude; CI: coagulation index.
TEG: thromboelastography.
Incidence of VTE and complications
In the rivaroxaban group, two patients (1.8%) had a postoperative DVT, while four patients (3.5%) in the enoxaparin group experienced a postoperative DVT. The difference of the incidence of VTE between the groups was not statistically significant (p = 0.683). Only one patient in enoxaparin group who suffered from lower limb swelling developed symptomatic DVT, other five cases of DVT were asymptomatic. No patient in either rivaroxaban or enoxaparin groups experienced a pulmonary thromboembolism. Only one patient in rivaroxaban group developed major bleeding events that resulted in a reduction of hemoglobin of more than 20 g/L, and recovered after red blood cell transfusion. This patient had dark stools for two consecutive days after operation and had no history of ulcer; it is considered that the bleeding of digestive tract was caused by rivaroxaban. Minor bleeding occurred in four patients (3.4%) in the rivaroxaban group and in three patients (2.6%) in the enoxaparin group (p = 1). Wound complications occurred in five patients (4.4%) in the rivaroxaban group and in three patients (2.6%) in the enoxaparin group (p = 0.722).
Discussion
Despite improvements in perioperative management, VTE remains a concern for surgeons performing THA. Our data showed that in comparison with enoxaparin, rivaroxaban was significantly more effective for the prevention of postoperative hypercoagulable tendency. However, no matter thromboprophylaxis with rivaroxaban or enoxaparin, patients undergoing THA remains in a hypercoagulable state at 7 days postoperation.
Rivaroxaban has enjoyed increasing popularity for VTE prophylaxis because of ease of use by oral administration. Many recent studies have attempted to demonstrate the safety of rivaroxaban as appropriate pharmacologic prophylaxis and do not need laboratory monitoring following arthroplasty.10,11 In the RECORD1 trial, the efficacy of rivaroxaban 10 mg once daily was compared with that of enoxaparin 40 mg once daily. 12 Eriksson et al. found that rivaroxaban was significantly more effective in preventing total VTE but was equivalent to enoxaparin regarding the rates of symptomatic VTE and major bleeding complications. 12 However, an increase in wound complication rate and return to surgery was reported in patients who received rivaroxaban after arthroplasty compared to those with LMWH.4,13 In addition, concerns exist for higher risk of bleeding event and the lack of commercially available agents to reverse the action of rivaroxaban if excessive bleeding occurs.14,15 Based on the previous reports, it was indicated that there may be different efficacy between rivaroxaban and enoxaparin for the prevention of VTE, but the hemodynamic evidence is still lacking.
Although routine plasma-based coagulation tests are easily available and cheap, they are not ideal for quantitative comparison between rivaroxaban and enoxaparin due to a discreet variation compared to normal values and a high dependency on the reagent used.16,17 In the present study, as shown in Table 2, despite significant differences observed in D-dimer between the two groups at 7 days after operation, there was no significant difference in the aPTT, PT, INR, and TT between the two groups at all time points. D-dimer was regarded as a high negative predictive value to exclude DVT. 18 Wu et al. 19 reported that D-dimer is not useful in the prediction of DVT after TKA in patients who used rivaroxaban for thromboprophylaxis due to its low sensitivity (58.6%), specificity (76%), and positive predictive value (29.3%). Helen et al. 20 also reported that D-dimer was not affected by rivaroxaban in patients undergoing hip or knee replacement surgery. In the present study, similarly, there were also no significant differences in D-dimer between day 1 and day 7 in rivaroxaban group.
Thromboelastography has been considered as better indicator of hypercoagulable state after injury than plasma PT or aPTT. 8 In Wang’s study, 21 TEG parameters PT, and aPTT were compared in 87 people with hip or knee arthroplasty. It was found that the number of patients with abnormal hemostatic state assessed by TEG parameters was higher than that assessed by PT and aPTT. Based on their results, they thought TEG was more sensitive in detecting abnormal preoperative hemostatic state and can be utilized for individualized prophylaxis therapy. 21 In our study, TEG was used to demonstrate the difference in coagulation function in patients using rivaroxaban or enoxaparin for thrombosis prophylaxis after THA. It was found that the R time of rivaroxaban group was significantly higher than that of enoxaparin group on day 7 after surgery, which may be due to the superior efficacy of rivaroxaban compared with enoxaparin. Rivaroxaban is a direct FXa inhibitor. It binds rapidly and competitively to the active site of both circulating FXa and FXa bound within prothrombinase complex. However, rivaroxaban has no effect on fibrin cross-linking and clot forming, and consequently inducing similar K and α-angle between the two groups on day 7 after surgery. McCrath et al. 22 found that the incidence of postoperative thrombotic complications in patients with MA > 68 (8.4%) was significantly higher than that of patients with MA ≤ 68 (1.4%). Similarly, Gary et al. 23 also showed that rapid TEG MA ≥ 65 and MA ≥ 72 on presentation were independent risk factors for DVT and PE in patients with severe extremity trauma, respectively. In the present study, the MA value in the rivaroxaban group was significantly less than that in the enoxaparin group at 7 days postoperatively. The difference may also be attributed to the different anticoagulant effect between rivaroxaban and enoxaparin. However, MA values of both groups were higher than 65 mm (65.05 ± 5.76 mm for rivaroxaban group, 67.76 ± 5.26 mm for enoxaparin group) at 7 days after operation, which means patients in both groups were still in hypercoagulable state, and had a high probablity of developing VTE. CI is a computer-calculated linear combination of the R, K, MA, and α-angle values and reflects overall coagulation status. Despite statistically significant differences in CI between the two groups on 7 days postoperative, this difference has no clinical relevance because all the mean values were in the normal reference value.
The limitations of the present study should be noted. First, the sample size is relatively small to detect differences in VTE rates between the two groups. However, the different incidence of VTE rates between rivaroxaban and enoxaparin has been demonstrated by several previous reports.11,12 The present study concentrated on the hemostatic changes between the two groups and significant difference was observed according to the thromboelastographic comparison. Second, only patients with length of hospital stay longer than 7 days were enrolled in the study, which may have introduced selection bias (patients discharged before postoperative day 7 were excluded from analysis). The hospital stay was related to individual factors, for example, to avoid return to hospital. Some patients, especially the elderly, were apt to discharge from hospital until the skin staples were removed. Moreover, in our country, the nursing expense and ward costs can be paid by medical insurance while they were still in hospital. Besides, our department also has a rehabilitation therapist, who was responsible for the rehabilitation exercise of patients after surgery. Therefore, the postoperative hospital stay in our study was usually longer than 7 days and significantly longer than that of previous reports. In addition, TEG was only compared between the two groups after 7 days of hospitalization, and the anticoagulant effect of rivaroxaban and enoxaparin could not be further compared. Finally, tranexamic acid was routinely used in both groups, which may have a certain impact on the TEG results. However, the use of tranexamic acid was identical between the two groups.
Conclusions
In conclusion, with regard to TEG analysis, there was coagulation difference in patients with rivaroxaban and those with enoxaparin as thromboprophylaxis after THA. Under recommended dose of rivaroxaban and enoxaparin, patients undergoing THA were in hypercoagulability on 7 days postoperative.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81902244), Research Project of Jiangsu Provincial Health Department (H201528),Jiangsu Provincial Medical Youth Talent (QNRC2016801), and Xuzhou Science and Technology Innovation Project (KC19063).