
Abstract
Purpose:
This study compares the kinematic changes after the procedures for scapholunate interosseous ligament (SLIL) reconstruction—the modified Brunelli technique (MBT) and Mark Henry’s technique (MHT).
Methods:
Ten cadaveric wrists were used. The scapholunate (SL) interval and angle and radiolunate (RL) angle were recorded using the MicroScribe system. The SL interval was measured by dividing the volar and dorsal portions. Four motions of the wrist were performed—neutral, flexion, extension, and clenched fist (CF) positions—and compared among five conditions: (1) intact wrist, (2) volar SLIL resection, (3) whole SLIL resection, (4) MBT reconstruction, and (5) MHT reconstruction.
Results:
Under the whole SLIL resection condition, the dorsal SL intervals were widened in all positions. In all positions, the dorsal SL intervals were restored after MBT and MHT. The volar SL interval widened in the extension position after volar SLIL resection. The volar SL interval was not restored in the extension position after MBT and MHT. The SL angle increased in the neutral and CF positions under the whole SLIL resection condition. The SL angle was not restored in the neutral and CF positions after MBT and MHT. The RL angle increased in the neutral and CF positions under the whole SLIL resection condition. The RL angle was not restored in the neutral and CF positions after MBT and MHT.
Conclusion:
The MBT and MHT may restore the dorsal SL interval. No significant differences in restoration of the SL interval between MBT and MHT were found in the cadaveric models.
Clinical relevance:
No significant differences between MBT and MHT were found in the cadaveric models for SLIL reconstruction. When considering the complications due to volar incision and additional procedures in MHT, MBT may be a more efficient technique in terms of operative time and injury of the anterior structures during surgery, but further research is needed.
Keywords
Introduction
Scapholunate (SL) dissociation is the most common type of carpal instability, which may be unnoticed at the time of injury and cause functional disabilities and arthritis of the wrist joint when left untreated. 1,2 Acute scapholunate interosseous ligament (SLIL) injury may be surgically treated by primary repair of the ruptured ligament with favorable results. 3 However, chronic rupture of the SLIL, which is unable to be primarily repaired, may require several other techniques such as dorsal capsulodesis, reduction and association using a screw to the SL joint (RASL), the scapholunate axis method (SLAM), bone–ligament–bone grafting, and reconstruction of the SL ligament. However, surgical outcomes are still controversial. 1,3 –11
According to Berger’s research, the SLIL can be divided into three components: volar, dorsal, and proximal components. The volar and dorsal components mainly contribute to the stability of the SL joint, and an isolated injury to the volar component does not cause instability. 4 The yield strength of the dorsal component is approximately 300 N, and the yield strength of the volar component is approximately 120 N. 12 Owing to this research, most early SL reconstruction procedures focused on the reconstruction of the dorsal component. Three-ligament tenodesis have been modified from modified brunelli technique (MBT), which is most commonly used for dorsal SL ligament reconstruction. 13 Although the three-ligament tenodesis technique is the most reliable technique with favorable results reported by several authors, reconstruction of only the dorsal component may result in low resistance to torsional force, and many authors have emphasized the importance of the volar component. 14 –17 Surgical techniques reconstructing both the volar and dorsal components were introduced recently. 18 –21 Recent improvements in surgical techniques could aid attempts to reconstruct both the volar and dorsal SL ligaments even though it has a few complication such as bone fracture, avascular necrosis of the lunate. 22 The present study is a comparative biomechanical study of surgical techniques for treating SL dissociation: MBT (dorsal SLIL reconstruction only) versus MHT (volar and dorsal SLIL reconstruction) (Figure 1).

Methods of scapholunate interosseous ligament (SLIL) reconstruction. (A) The modified Brunelli technique (MBT). (B) Mark Henry’s technique (MHT).
Materials and methods
Ten fresh-frozen cadaveric wrists were used for this study (mean age, 69.3 years; range, 61–81 years; eight males; six right-sided). After cutting the specimens off 12 centimeters proximally from the radial styloid process, the skin and subcutaneous fat tissues were dissected off the specimen. To reproduce the motion of the wrist joint, after dissecting FCR, flexor carpi ulnaris (FCU), extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), and flexor digitorum profundus (FDP) tendons, we cut the tendons 10 centimeters proximally from the radial styloid and sutured them using 2-0 FiberWire to put weight on them. We checked for any injuries of the SLIL following excision of the dorsal wrist capsules. Markers (screws) were inserted into the bones (two on the third metacarpal, two on the distal radius, one in each the volar and dorsal sides of the lunate, two on the volar scaphoid, and one on the dorsal scaphoid) using the MicroScribe system. When a specific point is designated, Microscribe device displays the designated location in three-dimensional space using x, y, z axes. With this equipment, the SL interval can be measured, and the SL angle, RL angle also can be measured by formula. The cadaveric specimens were fixed to a 6-cm-long polyvinyl chloride (PVC) pipe using plaster casts (Figure 2). After hanging the specimens on a hand jig, a pilot test was conducted using Pollock’s method in six positions, namely neutral, flexion, extension, ulnar deviation, radial deviation, and clenched fist (CF). 23 Producing consistent results was difficult because of differences in sizes and specimen preservation methods, which led to substantially different angles in each position. In the flexion position, markers of some specimens that were inserted into the volar aspects were covered by the distal radius and unchecked using the MicroScribe system. Accordingly, we decided to change the experimental design. After loading 10 N weights on the FCR, FCU, ECRL and ECRB (fixed together), and ECU tendons, we attached a bar to the third metacarpal bone and adjusted the angles equally (Figure 3). The specimens were fixed at 0° neutral, 60° flexion, 60° extension, and 0° CF. We did not measure the values under the ulnar deviation and radial deviation conditions. Furthermore, we did not determine the locations of the markers inserted into the volar side during flexion and the dorsal side during extension. In fact, one study demonstrated that the volar component had more strain than the dorsal component during wrist extension, whereas the opposite occurred during wrist flexion. 24 We tried to focus on the changes in the volar component during wrist extension and the dorsal component during wrist flexion. The conditions of the cadaveric specimens were in the following order: intact SLIL, volar SLIL resection, whole SLIL resection, MBT reconstruction, and MHT reconstruction. The procedures of the MBT and MHT reconstructions were performed in an arbitrary order after randomization.

(A) Schematic picture and marker location in the MicroScribe system: dorsal and volar aspects. (B) Cadaveric preparation after marker insertion: dorsal and volar aspects.

Testing system (marking position using Hand jig and MicroScribe).
The volar SLIL resection process was added because the dorsal SLIL in the specimens in which only the volar SLIL was resected can be regarded as intact or perfectly reconstructed and can thus be compared with the results of the MBT reconstruction. After all procedures were completed, we measured the thickness of half-slip FCR tendons that were used in the reconstruction process. Tendon thickness was measured twice from the proximal, middle, and distal parts. The average of the two measurements was recorded (Figure 4 and Table 1). 25 We conducted the pilot study before this experiment and used the results to calculate the sample size. The mean values of MBT and MHT groups in the clenched fist position from the pilot study were used as reference values. The calculated sample size was 6. Considering the probability of failure of the experiment, a sample size of 10 was finally considered.

Tendon thickness measurement.
The thickness of the flexor carpi radialis tendon graft.
FCR width: 3 mm (average), FCR graft area = 2.1*3 = 6.3 mm 2 .
Comparison for four wrist motions by five conditions was performed using repeated-measures one factor analysis. If the null hypothesis was statistically significant, the multiple comparison result was obtained by contrast with Bonferroni correction. All analyses were performed using Statistical Package for the Social Sciences (version 21.0; IBM Corp., Armonk, NY, USA). All tests were performed by two sided test and P values of 0.05 less were considered statistically significant.
Results
A statistically significant difference in the dorsal SL interval in the neutral, flexion, and CF positions was found between the whole SLIL resection condition and the intact and volar resection conditions (neutral: p = 0.035 and p = 0.041; flexion: p = 0.003 and p = 0.004; CF: p = 0.012 and p = 0.013). The dorsal SL interval decreased in the neutral position after MBT; however, no significance was found (p = 0.151). However, the intervals were significantly recovered in the flexion and CF positions (p = 0.001 and p = 0.048, respectively). After the MHT, the intervals significantly decreased in the neutral, flexion, and CF positions (p = 0.033, p = 0.004, and p = 0.007, respectively) (Table 2 and Figure 5).
The average of the dorsal scapholunate distance.


The dorsal scapholunate (SL) distance.
No significant difference in the volar SL interval was found between the intact and volar resection conditions and whole SLIL resection condition in both the neutral and CF positions. However, the volar SL interval significantly increased after the SLIL volar resection and whole SLIL resection conditions (p = 0.037 and p = 0.035, respectively) in the extension position compared with that after the intact condition.
The volar interval was not recovered after MBT and MHT in the extension position (p = 1.000, p = 0.126, respectively). The volar interval was not statistically significant difference between MBT and MHT in the neutral, extension and CF position (p = 0.608, p = 1.000, p = 1.000, respectively) (Table 3 and Figure 6).
The average of the volar scapholunate distance.


The volar scapholunate (SL) distance.
The SL angle significantly increased after the whole SLIL resection condition compared with that after the intact and volar resection conditions in the neutral and CF positions (neutral: p = 0.03 and p = 0.011; CF: p = 0.011 and p = 0.006). The SL angle decreased after the MBT in the neutral position compared with that after the whole SLIL resection condition, but without a statistically significant difference. However, the SL angle significantly decreased after the MBT compared with that after the whole SLIL resection condition in the CF position (p = 0.028) (Table 4 and Figure 7). The SL angle after MHT decreased compared with that after the whole SLIL resection condition in the neutral and CF positions, but without a statistically significant difference (p = 0.052).
The average of the scapholunate angle.


The scapholunate (SL) angle.
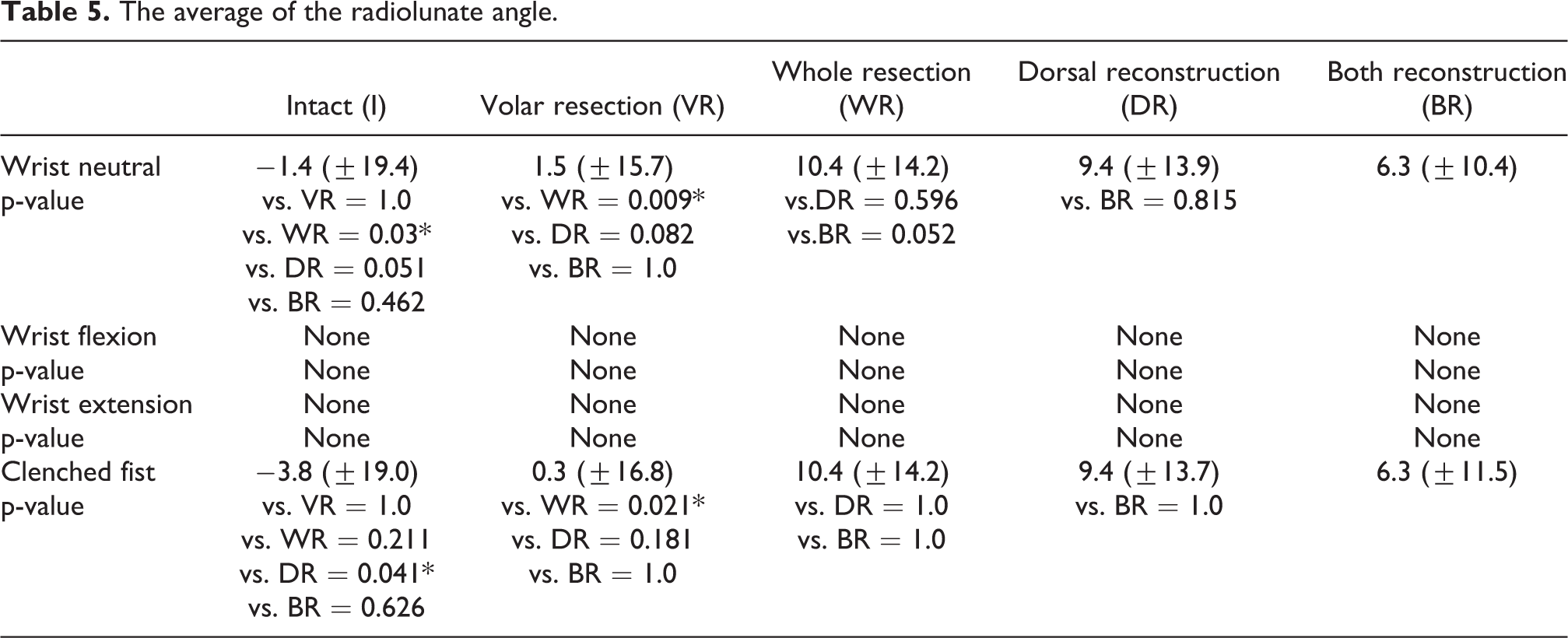
The radiolunate (RL) angle significantly increased after the whole SLIL resection condition in the neutral and CF positions compared with that after the volar SLIL resection condition (p = 0.021). The RL angle decreased without statistical significance after MBT in both the neutral and CF positions compared with that after the whole SLIL resection condition (p = 0.181 and p = 0.097, respectively). The RL angle after MHT tended to decrease compared with that after the whole SLIL resection condition in the neutral and CF positions, but without a statistically significant difference (p = 0.626 and p = 0.727, respectively) (Table 5 and Figure 8).
The average of the radiolunate angle.

The radiolunate (RL) angle.
Discussion
Garcia-Elias and colleagues evaluated SLIL injuries using several factors—”Is the dorsal SLIL intact?,” “Can it be repaired?,” “Is the scaphoid aligned normally?,” “Is the carpal malalignment easily reducible?,” and “Is the cartilage in both the radiocarpal and midcarpal joints normal?”—and proposed a classification system with six stages. 1 Treatment of stage 3 and 4 injuries should include sound reconstruction of the SLIL. Surgical procedures emphasized the reconstruction of the dorsal component of the SLIL after the research of Berger had been introduced. Although the outcomes of the MBT were reported to be favorable, volar component deficits inevitably resulted in low resistance to torsional and translational forces. 12 In this respect, the importance of the volar component has been emphasized by several researchers. 20,26 Chee and colleagues introduced an antipronation spiral tenodesis technique, which is a modification of the three-ligament tenodesis. 18 The FCR tendon is passed through the scaphoid tunnel from the volar side to the dorsal side and then brought from the dorsum of the triquetrum to the volar aspect through an interosseous tunnel to be inserted into the radial styloid process and used for reconstruction of the spiral ligaments around the carpal bones. Although long-term results are lacking, the antipronation technique is considered to be more reliable than existing techniques.
Ho and colleagues described an arthroscopic reconstruction technique repairing both the volar and dorsal SLILs using the palmaris longus tendon with favorable outcomes. 20 Furthermore, Henry reported favorable outcomes after reconstruction of both the volar and dorsal SLILs. 19 Kang et al. conducted load-to-failure tests between dorsal SLIL repair methods and Kakar and Greene conducted load-to-failure tests between 360° SLIL reconstruction with only tendon and 360° SLIL reconstruction with tendon and internal brace. 21,27 But there’s no biomechanical study between Dorsal SLIL reconstrudction method and 360° SLIL reconstruction. So we conducted a biomechanical comparative study between MBT and MHT to emphasize the volar SLIL. We used the MicroScribe system to measure the SL interval from both the volar and dorsal aspects.
We have assumed that there would be significant differences in the volar SL interval, the SL angle, and the RL angle when the volar and dorsal components of SLIL were both reconstructed compared with dorsal reconstruction only. However, after whole SLIL resection, the difference in the volar SL interval was statistically significant only in the extension position, but not in the neutral or CF position. After MHT, mean volar SL distance was more decrease than at MBT procedure, but it was not statistically significant. For this reason, we thought it was due to the physical characteristics of the collagen, tendon stretching.
The SL angle significantly increased after the whole SLIL resection condition compared with that after the intact condition. The SL angle tended to be reduced after MBT or MHT; however, no statistical significance was found.
The SL angle tended to be reduced more after MHT than after MBT, but without a statistically significant difference. The RL angle significantly increased after the whole SLIL resection condition compared with that after the volar SLIL resection condition. The RL angle was barely reduced after MBT but was insignificantly reduced after the MHT. The SL and RL angles were reduced more after MHT, but without a statistically significant difference. After the importance of the dorsal SLIL had been pronounced, the favorable results of the MBT were reported by several authors. The operative time can be reduced since the procedure is performed using a single skin incision, and secondary injury to the anterior structures can be avoided. However, resistance to torsional force may be weaker than MHT since MHT involves reconstruction of both the volar and dorsal components. In our study, the dorsal SL interval was extremely reduced after both MHT and MBT. There is no statistical difference in the volar SL interval between two techniques.
Although MHT may have advantages, MBT may be a more efficient technique in terms of operative time and injury of the anterior structures during surgery. Further clinical research is needed to compare the superiority of these two techniques.
This study has several limitations. First, since we used cadaveric models, the study may not reflect the actual clinical situations. Second, the markers of the SL bone may not have been in the exact same spot; thus, the SL or RL angle may have varied. We tried observing the changes under normal conditions, but the data we have obtained may not have been precisely observed. Third, all assessment is conducted without the influence of the extrinsic ligaments and, muscle pulling around the wrist joint, which also plays and important role for SL kinematics. Alternatively, the study strengths include that we recorded the volar and dorsal SL intervals separately, and we tried measuring the changes precisely using the MicroScribe system, in which the error limit is within 1 millimeter.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2020R1G1A110118511).