
Abstract
Purpose:
To assess the clinical value and feasibility of the dorsoulnar flap of the thumb combined with relay V–Y flaps for reconstruction of the thumb fingertip injuries.
Methods:
In this retrospective study, we retrospectively reviewed 20 patients (13 men, 7 women; June 2014–June 2016) with thumb fingertip defects who underwent reconstructive procedures with transfer of the dorsoulnar flap of the thumb. The average size of the defects ranged from 1.8 cm × 2.0 cm to 2.0 cm × 3.0 cm, whereas the reconstructed dorsoulnar flap of the thumb ranged in size from 2.0 cm × 2.2 cm to 2.2 cm × 3.0 cm. A V-Y flap was used to repair the donor site at the same time. Sensation within the reconstructed thumb, the aesthetic appearance of both the donor and recipient sites, functional recovery, and return-to-work (RTW) time were measured.
Results:
All 40 flaps survived without necrosis. The follow-up period ranged from 6 to 24 months. There were no complications reported. The mean static two-point discrimination values at the reconstructed thumb fingertip and donor site were 8.5 mm (range 8–10 mm) and 12.5 mm (range 12–14 mm), respectively. The average visual analog scores for the aesthetic appearance of the recipient and donor sites were 8.4 (range 8–9.5) and 9.6 (range 9–10), respectively. The average Michigan Hand Outcome Questionnaire score for the reconstructed hand was 9.4 (range 6–16). The average RTW time was 9.8 weeks (range 6–13 weeks). All patients were satisfied with the aesthetic outcome.
Conclusion:
The dorsoulnar flap of the thumb is an ideal alternative for reconstruction of the thumb fingertip injuries, and a V-Y flap was suitable for repairing the donor site with a reduced incidence of complications.
Introduction
Thumb fingertip reconstruction has been a common issue for hand surgeons. 1,2 Accordingly, a variety of reconstructive methods have been described in an effort to obtain satisfactory sensory recovery. 3 –6 Of those treatments, the neurovascular island pedicle flap obtained the satisfactory function and shape and getting more popular. The dorsoulnar flap of the thumb was first described by Brunelli et al. in 1991 and became widely used in 1993. 7 The ulnar dorsal digital artery of the thumb originates from the palmar arteries. Given the low incidence of anatomic variation in the ulnar dorsal digital artery and the simplicity of this reconstructive procedure, the dorsoulnar flap was widely applied to cases involving distal amputation, loss of the palmar surface, or loss of dorsal tissue. 8 However, long and/or large flaps result in notable increases in donor site suture tension, which produces a local scar. Skin grafting also generated complaints among patients because of its pitting shape and scar hyperplasia. 2,4 As a result, repair of the donor site has become an independent issue. Modification of the conventional surgical technique is essential to minimize the donor site complications. Therefore, in this study, we report our experience with using a dorsoulnar flap of the thumb for thumb fingertip reconstruction and performing surgical repair of the donor site using a V-Y flap pedicled with a dorsoulnar flap of the proximal thumb perforator. With this technique we achieved satisfactory appearance, sensory and functional recovery
Materials and methods
Patients
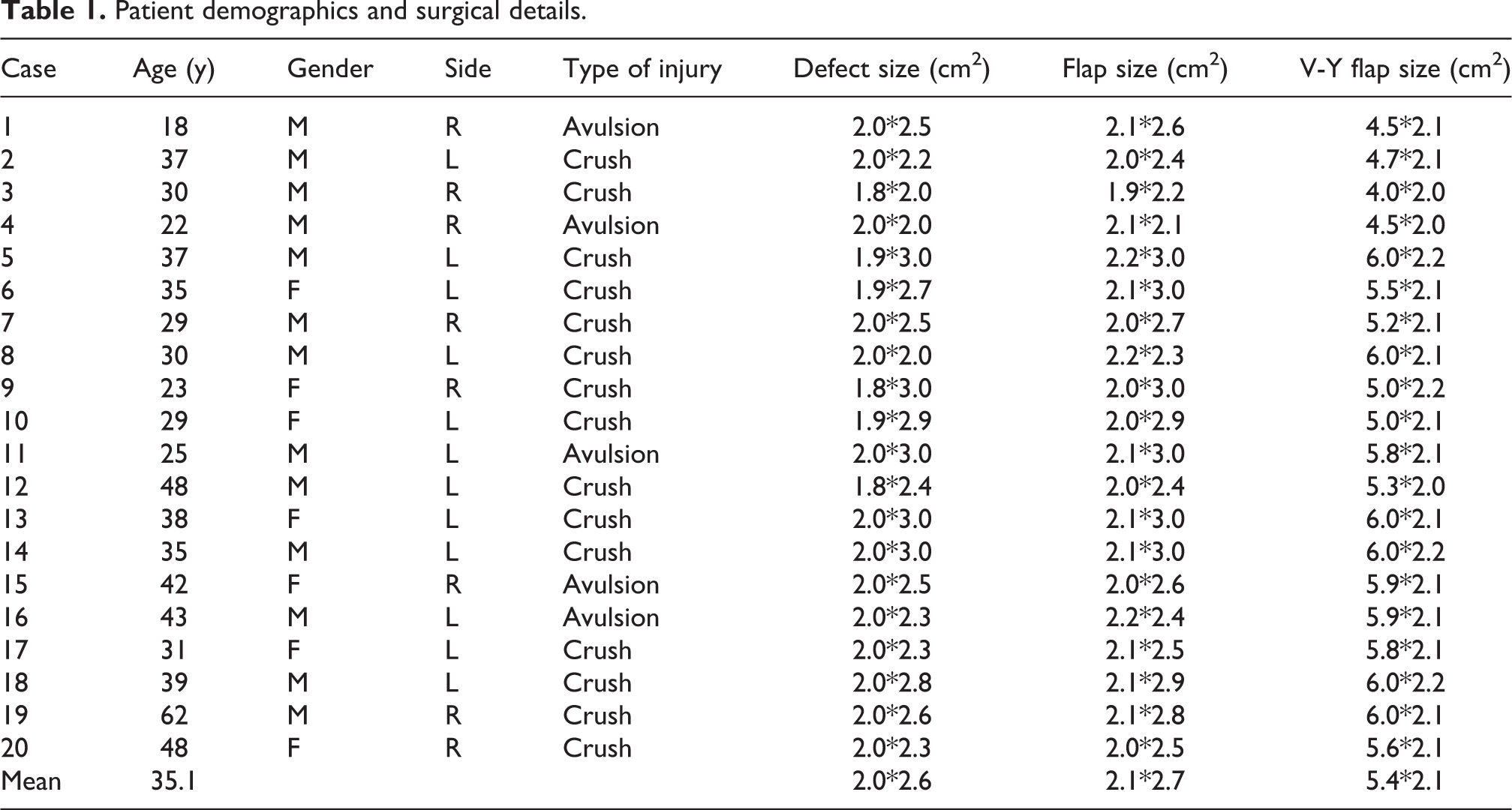
From June 2014 to June 2016, 20 patients with thumb fingertip defects underwent surgical reconstruction using dorsoulnar flap of the thumb transfer. Thirteen patients were male and seven were female, with an average age of 35.1 years (range, 18–62 years). Inclusion criteria were defect not beyond the distal interphalangeal joint, less than 65 years, responsible patient and with reasonable expectations. Exclusion criteria were dysvascular patients, heavy smoking, chemotherapy, or corticosteroid treatments. The causes of injury included 15 crush traumas and 5 avulsion traumas. The injuries were all located at the thumb pulp. The average size of the defects ranged from 1.8 cm × 2.0 cm to 2.0 cm × 3.0 cm and the flap sizes ranged from 2.0 cm × 2.2 cm to 2.2 cm × 3.0 cm. The V-Y flap pedicled with a dorsoulnar flap of the proximal thumb perforator ranged in size from 4.0 cm × 2.0 cm to 6.0 cm × 2.2 cm (Table 1).
Patient demographics and surgical details.
After surgery, the viability of flaps, presence of infection, appearance of flaps were observed. Sensibility of the flap was measured using the static 2-point discrimination (2PD) test. In addition, static 2PD of the donor site were also evaluated. The average visual analog (VAS) scores were used to evaluate the aesthetic appearance of the recipient and donor sites. Michigan Hand Outcome Questionnaire (MHOQ) score was used to evaluate the hand function. Cold intolerance of the flap was measured using the self-administered Cold Intolerance Severity Score questionnaire.
The clinical study was approved by the Ethical Committee of our institution, and all participants signed an exhaustive informed consent form after being informed of the benefits and risks of the procedure.
Regional anatomy of the dorsoulnar flap of the thumb
The dorsoulnar flap of the thumb exhibits a similar texture and thickness as the thumb pulp and provides tolerable scar contracture. The ulnar dorsal digital artery of the thumb originates from the palmar arteries at the head of the first metacarpal bone. Moreover, the ulnar dorsal artery was larger in diameter than the radial artery. The dorsoulnar artery formed extensive anastomosis with the palmar arch and dorsal digital artery arch, which provided the anatomical basis for the flap (Figure 1). Additionally, the presence of the dorsal digital nerve facilitated the restoration of sensation within the thumb.

(a) The ulnar dorsal digital artery. (b) The thumb dorsal perforator vessels.
Surgical technique
Surgery was performed under a brachial plexus block. Then, the wound was treated surgically with thorough irrigation and debridement. According to the area and shape of the wound defect, the flap was marked on the dorsoulnar surface of the metacarpophalangeal (MCP) joint. The axis of rotation was defined as being approximately 1 cm proximal to the MCP joint. The flap was then removed from the donor site in a proximal-to-distal direction along the dorsoulnar arterial axis in a subfascial dissection plane. The pedicle of the flap was elevated with the dorsal digital artery and the surrounding 3–4 mm fascia tissue. The dorsal perforator vein was identified when the flap was elevated near the axis. Then, the flap was rotated to cover the wound and the ulnar dorsal digital nerve was juxtaposed to one of the volar digital nerves. Since the donor site could not be closed primarily, we designed a V-Y flap pedicled with dorsoulnar of the thumb proximal perforator at the proximal end of the wound. The width of the V-Y flap was equal to the width of the wound, and the length of the flap was approximately 2.5 times the width. In this way, the donor site was resurfaced with the relay V-Y advancement flap and the flap was sutured without introducing excessive tension (Figure 2).

(a) The thumb fingertip defects. (b) The flap was marked on the dorsoulnar surface of the MCP joint. (c and d) The thumb fingertip defects and the donor site was resurfaced without tension. (e) The shape and function of the affected sites recovered well by the time of follow-up. MCP metacarpophalangeal.
During surgery, several items were considered. First, the rotation point was designed according to the location of the wound such that arterial supply, venous return, and postoperative functional recovery were guaranteed. Second, while harvesting the dorsoulnar flap of the thumb, the adipose tissue in the flap margin was ensured to be minimal and left in situ to ensure the proper appearance of the flap and prevent a thin thigh shape after repair of the donor site. Third, when dissecting the dorsoulnar flap of the thumb, all fibrous septa were removed, thereby leaving only two to three perforating branches and innervated nerves supplying the flap. This ensured that the surgeon could advance the extensive distance of the flap. The subcutaneous tissue of the flap was sutured to the wound, layer by layer at a time, to avoid high tension that could otherwise result in flap necrosis. Additionally, systemic postoperative rehabilitation training was required for functional recovery.
Results
All 20 flaps survived completely, without of vascular insufficiency or venous congestion and donor site healing was achieved in all cases. No infectious complication was observed. All the flaps displayed warmth, good texture matches and contour, and pink color 3 weeks after surgery. Follow-up ranged from 6 to 24 months, with an average of 13 months, and all 40 flaps in the 20 patients survived (Table 2).
Follow-up outcomes.

2PD, 2-point discrimination; CI, Cold intolerance; MHOQ, Michigan Hand Outcome Questionnaire; RTW, return-to-work; VAS, visual analog scores.
Discussion
The thumb accounts for 40–50% of the function of the hand. 9 Additionally, thumb fingertip injury is among the most common injuries in the upper limb. 10 The fingertips are also the most important organs for tactile sensation. Therefore, reconstruction of sensation of the thumb fingertip is considered essential by hand surgeons after a thumb fingertip injury. Ideal repair methods must restore both sensation and the contour of the thumb fingertip. 11 A dorsoulnar flap of the thumb meets the above conditions and, currently, has become a popular local island flap for use in thumb fingertip reconstruction. 12 Chen et al. 13 modified first dorsal metacarpal artery flap from the homodigital dorsum of the digit, but left a large linear scar. Liu et al. 4 showed that the neurovascular island pedicle flap obtained from long finger, but it caused injury to the long finger. In a study by Teran et al. 14 researchers modified the classic Brunelli flap to avoid vascular compromise and to enable primary closure of the donor site. Yet, these patients exhibited defects that were not extensive and the portions that were injured did not exhibit sufficient recovery of sensation. In our study, we successfully reconstructed the sensation of a relatively large defect at the thumb fingertip. Moreover, we also repaired the donor site with a relay V-Y flap pedicled with a dorsoulnar flap of the thumb perforator and achieved satisfactory clinical results. Compared with the previous reports, we have successfully reconstructed larger defects and have been confirmed in more cases. Sensory function recovered well in the follow-up, and returned to work after a short time (average 9.8 weeks).
In our previous study, we repaired the defect in the donor site following generation of a reverse digital artery island flap by generating a perforator V-Y flap from the dorsum of the proximal portion of the phalanx, which achieved satisfactory results. In our experience, the relay V-Y flap for repair of the donor site should meet the following conditions: (1) the procedure is easy to perform and does not greatly extend the duration of surgery; (2) the relay flap can be sutured directly to the donor site in the same operation without requiring further surgery.
For the recovery of the donor site for the dorsoulnar thumb flap, we made full use of the laxity of the skin of the proximal nasopharynx and combined the relative constant anatomy of the dorsoulnar of the proximal thumb perforator. In this way, we developed a V-Y flap pedicled with a dorsoulnar flap of the thumb perforator, which not only retains the characteristics of a traditional V-Y advancement flap, but also can be sutured directly and increases the size of the dorsoulnar flap. Based on our experience, the maximum length of the flap is 3.8 cm and width is 2.7 cm. This procedure takes about 20 min which is similar to skin grafting, or even less.
The operation described herein has several advantages. First, the operation and design is simple, introduces less trauma, and requires no sacrifice of the main vessel. Second, the thickness and texture of the flap more closely approximates the dorsum of the thumb. Moreover, the donor site is repaired using a V-Y flap pedicled with a dorsoulnar flap of the proximal thumb perforator, thereby reducing the complications associated with skin grafting. Third, when dissecting the dorsoulnar flap of the thumb, all the fibrous septa should be cut off, leaving only two to three perforating branches and innervated nerves connecting with the flap, to ensure the distance of the flap can be advanced. Therefore, the flap blood supply was sufficient and the incidence of postoperative vascular crisis was low. Fourth, the sensory function of the flaps recovered well. There are also limitations in the present study. Healing of the V-Y flap is usually accompanied by minimal scarring on the dorsum of hand. Our technique should be repeated in a larger population to ensure its efficacy and low incidence of complications. Further anatomical and clinical research is needed to corroborate and expand our findings.
Conclusion
Our study’s findings indicated that the dorsoulnar flap of the thumb is an ideal alternative for reconstruction of the thumb fingertip, and a V-Y flap was suitable for repairing the donor site with a reduced incidence of complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.