
Abstract
Purpose:
To clarify the biomechanical and radiological outcomes of superficial medial collateral ligament (sMCL) repair using suture anchors in a large animal model.
Methods:
The right sMCLs of nine male castrated pigs was completely detached at the femoral attachment. sMCL repair surgery was performed using two suture anchors. The same skin incision, sMCL exposure, and immediate wound closure were made at the left knee as a sham surgery. Magnetic resonance imaging was performed preoperatively and 4 weeks after surgery. The structural properties (upper yield load, maximum load, linear stiffness, and elongation at failure) of the femur-sMCL-tibia complex were determined.
Results:
During tensile testing, all the repaired sMCLs avulsed from the femoral attachment. There were no significant differences in the upper yield load, maximum load, linear stiffness, or elongation at failure between the groups 4 weeks after surgery or in the MRI-derived signal-to-noise quotients (SNQs) at the mid and tibial sMCL. The SNQs differed significantly at the femoral (2.7 ± 1.2 vs 0.3 ± 0.7; P = 0.00064) portions between groups.
Conclusion:
The injured sMCLs biomechanically recovered after surgery using suture anchors even though the SNQs were higher than those with native contralateral sMCLs. For clinical relevance, sMCL repair of grade 3 sMCL injuries using suture anchors was both safe and successful with less tissue dissection.
Introduction
The superficial medial collateral ligament (sMCL) serves as a primary restraint (40–54%) against knee valgus force. 1 Injury in this ligament is relatively common and accounts for up to 42% of all knee ligament injuries in young athletes. 2 Most patients with sMCL injuries of varying severity can achieve pre-injury activity levels with non-surgical treatment alone. 3 Patients with grades 1 and 2 sMCL injuries can expect good results with non-operative treatment. 4 Conversely, although good clinical results have been reported with the immediate application of splint immobilization 5 and because the sMCL displays a high self-healing potential, even in grade 3 injuries, 6 conservative treatment can sometimes result in remaining valgus and rotational instability with inferior outcomes in multiligamentous injuries 7 because nearly 78% of patients who sustain a grade 3 sMCL injury simultaneously have an injury to another associated structure. 8 The remaining sMCL laxity following conservative treatment may lead to abnormal knee contact stress and kinematics, 9 and an insufficient sMCL can lead to increased rotational knee laxity in both internal and external motions. 10 Therefore, primary repair of the sMCL is sometimes required in acute combined posteromedial and anterior cruciate ligament (ACL) injuries 11 and in cases of severe instability.
In a previous systematic review, DeLong and Waterman 12 described that repairing the sMCL of the knee might be an effective and reliable treatment for medial-sided knee injuries that can result in improved valgus stability and patient-reported functional scores with low rates of secondary failure. Primary repair of the sMCL is usually performed within 7–10 days of injury 2 ; this repair is performed with sutures alone or with sutures plus suture anchors. 13 The repair of acute grade 3 sMCL injuries using suture anchors is reportedly a successful procedure that requires less tissue dissection, thereby resulting in fewer complications. 14 Forkel et al. reported on the successful treatment of grade 3 sMCL injuries by reattachment to the anatomical insertion site using anchors. 15 Additionally, Ono et al. 16 and Khoschnau et al. 17 described the efficacy of suture anchors for sMCL fixation using a rabbit model. However, no previous in vivo biomechanical studies have used a large animal model to assess the efficacy of suture anchors for sMCL fixation.
Therefore, this biomechanical study aimed to evaluate the efficacy of suture anchors for the early repair of acute grade 3 sMCL injuries using a large animal (i.e., porcine) model. We hypothesized that the early repair of acute grade 3 sMCL injury with the use of suture anchors is both safe and effective.
Materials and methods
Study design
Nine male castrated pigs (average weight, 40.0 ± 5.2 kg; weight range, 33.0–48.0 kg) were purchased from San-S breeding (Funabashi, Japan). All experimental protocols were approved by Animal Care and Use Committee, Jichi Medical University (Approval no. 17004-03). All methods were carried out in accordance with relevant guidelines and regulations.
sMCL repair
A medial longitudinal skin incision of the right knee was made while the pigs were intubated under general anesthesia and aseptic conditions (Figure 1(a)). The sMCL was completely detached at the femoral attachment using a No. 15 scalpel to create an avulsion injury (Figure 1(b)). Two 2-mm guide wires were inserted into the femur at the center of the proximal MCL attachment (Figure 1(c)). Two 1.7-mm suture anchors (SUTUREFIX ULTRA XL, Smith & Nephew Endoscopy, Andover, MA, USA) were inserted via each guide hole in accordance with the manufacturer’s instructions. Then, the detached sMCL was stretched and re-anchored. The sMCL repair was performed using a No. 2 Ultra Blade attached to each suture anchor (Figure 1(d)). The incision was routinely closed in layers beginning with the deep fascia of the vastus medialis muscle. Dressing was applied and removed within 48 hours after surgery. An addition skin incision, exposure of the sMCL, and immediate wound closure were made to the left knee as a sham surgery.

(a) The superficial medial collateral ligament (sMCL) was exposed through a longitudinal skin incision. (b) sMCL was detached at the femoral attachment. (c) Guide wires insertion into the femur at the center of the proximal MCL attachment. (d) sMCL repair using two suture anchors.
Postoperative management
Postoperatively, the animals were returned to their cages (2 × 3 m) and allowed full weight bearing of the limbs without any movement restrictions. Each animal was observed once to twice each week to monitor the occurrence of protective limping or discharge of pus. All animals were sacrificed 4 weeks after surgery, and knee specimens were immediately retrieved after euthanasia.
Image assessment
Magnetic resonance imaging was performed using a 1.5-T instrument (MAGNETOM ESSENZA; Siemens Healthineers, Erlangen, Germany) with an extremity coil with the knee extended as much as possible both preoperatively and at 4 weeks after surgery just before euthanasia. Oblique coronal images parallel to the longest axis of the MCL were acquired using fast spin-echo T2-weighted imaging, with repetition and echo times of 1020 and 20 ms, respectively. The signal-to-noise quotients (SNQs) of the tibial, mid, and femoral portions of the injured MCL were calculated using the region of interest (ROI) technique. An ROI of the lateral collateral ligament (LCL) signal at the joint level and the background signal at approximately 2 cm medial to the MCL were measured to normalize the signal intensity of the MCL. All ROIs were circular with a diameter of 3.3 mm. All five ROI measurements were performed using a picture archiving and communication system (GE Healthcare, Barrington, IL, USA) (Figure 2). The following equation was used to quantify the SNQ of five ROI measurements: SNQ = (MCL femoral, mid, or tibial signal–LCL signal)/background signal. 18

Points of regions of interest for the signal-to-noise quotient calculation.
Structural properties of the femur-sMCL-tibia (FMT) complex
The prepared FMT complex specimens were mounted on a tensile tester (Tensilon RTG-1250; Orientec Co., Ltd., Tokyo, Japan.) with a set of specially designed grips so that a tensile load was applied to the repaired sMCL in parallel with the long axis. This measurement system was the same as that used in previous biomechanical studies with large animals. 19 The tibia was fully extended during this measurement. 20 Before testing, the specimens were preconditioned with a static preload of 5 N for 10 min, followed by 10 cycles of loading and unloading with 3% strain as determined from calculations obtained with this software (Tensilon Advanced Controller for Testing; Orientec Co., Ltd.) with a cross-head speed of 20 mm/min. Then, each specimen was stretched to failure using the same conditions as those of preconditioning at a cross-head speed of 50 mm/min (Figure 3). These measurement conditions have been frequently used in previous studies with large animal models. 19,21 –23 Failure modes were video-recorded. A load-elongation curve was created with this software (Figure 4). The structural properties (upper yield load, maximum load, linear stiffness, and elongation at failure) of the FMT complex were determined from calculations obtained with this software. The upper yield load represents the point at which a sudden leveling or drop in a load-elongation curve occurs as a material transitions from elastic to plastic deformation.

Femur-medial collateral ligament-tibia complex specimen mounted on a tensile tester with a set of specially designed grips. A tensile load was applied to MCL in parallel with its long axis.
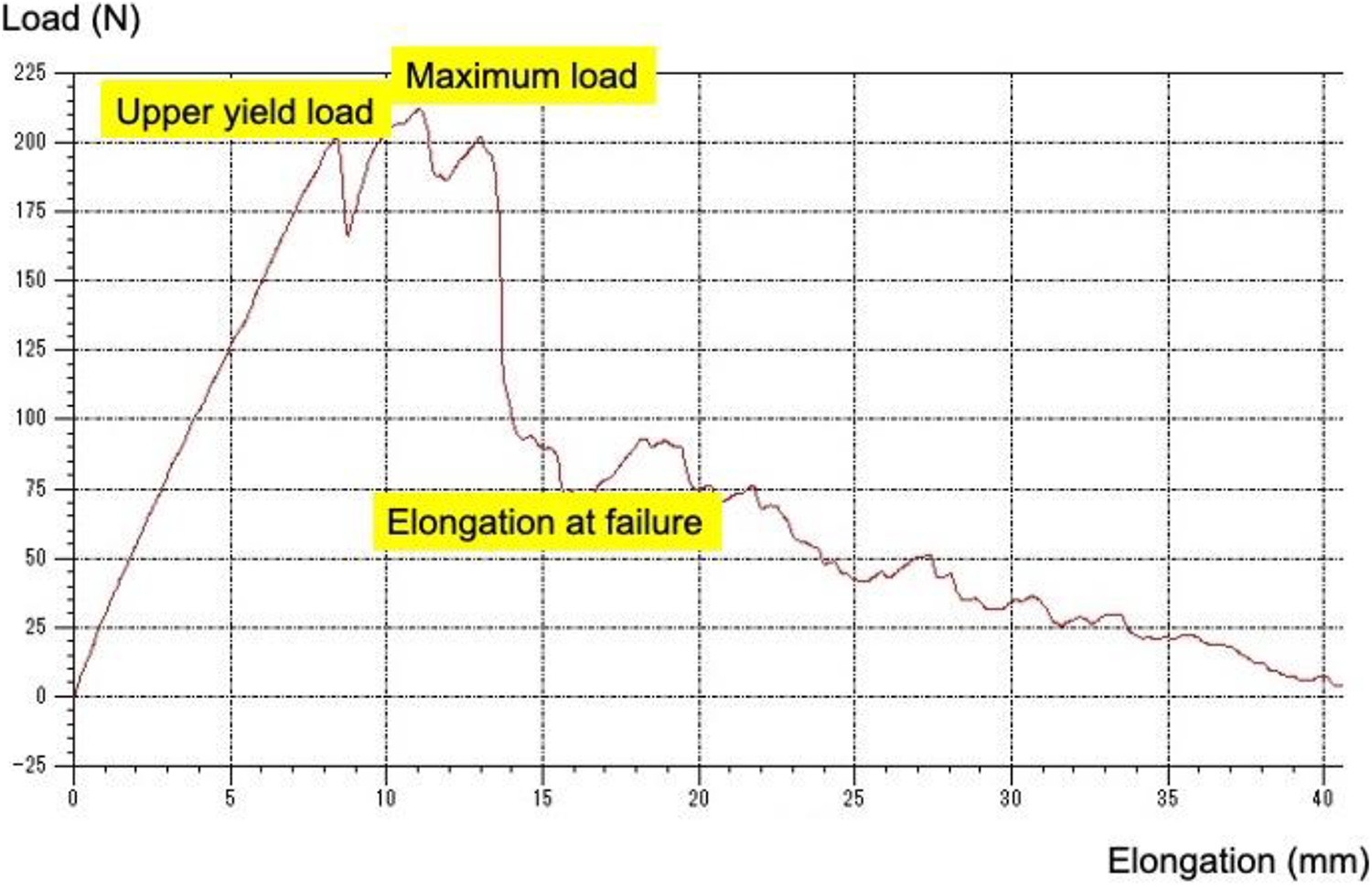
A schematic image of load-displacement curve obtained with this software. The following equation was used to quantify the linear stiffness: linear stiffness = (upper yield load)/elongation at upper yield load.
Statistical analyses
A priori power analysis was performed using G* Power 3.1 (Franz Paul, Kiel, Germany). The sample size was calculated with 70% power and a Cohen’s effect size of 0.80 24 to test the study hypothesis. All data from the statistical analyses are presented as the means ± standard deviations. The paired t-test with the Bonferroni correction was used to evaluate differences between groups. All statistical analyses were performed using EZR software (http://www.jichi.ac.jp/saitama-sct/SaitamaHP.files/statmed.html). 25 A probability (p) value of <0.0071 was considered statistically significant because seven total paired t-tests were performed in this study.
Results
Gross observations in the knee joint
No infectious symptoms such as pus from the joint, movement of the suture anchor, or sMCL ruptures were observed at the time of euthanasia.
Biomechanical evaluations of the femur-sMCL-tibia complex
During tensile testing, all the repaired sMCLs avulsed from the femoral attachment in each animal at 4 weeks, which is frequently observed in clinical settings (Figure 5). There were no significant differences in the upper yield load (181.5 ± 46.3 vs 229.8 ± 98.9 N), maximum load (250.1 ± 63.1 vs 267.8 ± 106.0 N), linear stiffness (26.9 ± 14.3 vs 26.8 ± 10.9 N/mm), or elongation at failure (13.4 ± 5.8 vs 13.0 ± 7.1 mm) between the repaired sMCL and native sMCL groups 4 weeks after surgery (Table 1).

Superficial medial collateral ligament avulsion after tensile testing.
Results of tensile testing.

Data are expressed as the mean (standard deviation).
* Student’s t-test.
Probability (p) value of <0.0071 was considered statistically significant with 70% power when Cohen’s effect size of 0.80 was applied.
Radiological evaluations of the SNQs using magnetic resonance imaging
There were no significant differences in the SNQs calculated using the ROI at the tibial sMCL (1.6 ± 1.4 vs 1.2 ± 0.9, respectively) and the mid portions (2.0 ± 1.7 vs 0.4 ± 0.7, respectively) between the repaired sMCL and native groups 4 weeks after surgery. Conversely, there were significant differences in the SNQ calculated using the ROI at the femoral portions (2.7 ± 1.2 vs 0.3 ± 0.7, respectively, P = 0.00064) between the repaired sMCL and the native sMCL groups (Table 2).
Results of signal-to-noise quotients.

Data are expressed as the mean (standard deviation).
* Student’s t-test.
Discussion
The present study first clarified how the injured sMCL biomechanically recovers with the use of suture anchors at 4 weeks after surgery. We used an ultimate load to failure test that represented the load increase in unintentionally performed movements. 26 Failure of the repaired sMCLs by tensile testing exhibited no ligament mid-substance tearing, but femoral attachment avulsion was observed in all model animals, as was failure of the sham sMCL repair. Additionally, there were no significant differences in structural properties (i.e., upper yield load, maximum load, linear stiffness, and elongation at failure) between the repaired and sham sMCL groups. However, there were significant differences in the SNQs of the femoral sMCL 4 weeks after surgery between groups; conversely, there were no significant differences in the mid and tibial SNQs.
The effects of suture anchors on the repaired sMCL after sMCL repair surgery were also assessed. The outcome of instability surgery of the knee is supposedly dependent on the secure fixation and healing of soft tissue to bone. 17 Suture anchors were first reported as an easier device to obtain secure stability for use in soft tissue fixation to bone without constructing transosseous suture tunnels. 27 A previous biomechanical study reported that sMCL repair using suture anchors results in better healing compared with fixation with screws or staples. 16 Khoschnau et al. performed bilateral knee sMCL repair in a rabbit model and compared two types of plates: one with a flat undersurface and a second with a pegged undersurface. 17 In that study, mechanical testing of pegged anchors, which mimic suture anchors, was performed 4 weeks after surgery and showed better maximum load, linear stiffness, and energy uptake. Louati et al. performed rotator cuff repair in a rabbit model and compared it with a contralateral native rotator cuff. 28 They noted that the repaired rotator cuff obtained a comparable maximum load as that of the native rotator cuff. However, these studies used a rabbit model, whereas the current study is the first to use a large animal model. The sMCL dimensions of a pig are reported to be comparable to those of the human sMCL. 29 Therefore, a porcine model was used in the present biomechanical study of sMCL repair.
The results of the present study demonstrated that the use of suture anchors for the repair of grade 3 sMCL injuries enabled early postoperative joint mobilization and weight bearing without deterioration of the structural properties of the repaired sMCL 4 weeks after surgery. However, the femoral SNQs of the repaired sMCLs were significantly higher than those of the sham sMCLs, indicating that healing and maturation of the repaired sMCLs was insufficient compared with the native group at 1–4 weeks after surgery.
The present study has several limitations. First, a porcine model was used in this study; thus, some of the findings may not be directly transferrable to clinical practice for human patients. Additionally, creating a negative control group with conservative treatment for grade 3 sMCL injury was realistically impossible in a porcine model because of the difficulty of splint immobilization. Second, only male castrated pigs were used in this study because of the limited availability of our animal experimentation facility. Gender differences might have influenced the mechanical properties of repaired sMCL, as was noted in a previous study on reconstructed ACL. 30 Third, the animals were not allowed to freely roam outdoors. This might have influenced the results. Fourth, the sMCL avulsion was made sharply using a scalpel at the femoral attachment. This type of injury is not the same as that caused by a valgus traction force, which is frequently observed clinically. The forces involved in sMCL tearing may change the properties of the torn ligament tissues. Fifth, the follow-up period was relatively short (4 weeks). However, in their finite element study, Wan et al. had described that a partially healed sMCL might be sufficient for providing restraints for the knee joints and would not lead to the occurrence of high strains in the sMCL. 26 Sixth, this study did not establish a minimal clinically important difference 31 of MRI-derived SNQs, and it remains unclear whether this surgical technique can recover the SNQ to that of the native sMCL after long-term follow-up. Determining this is necessary to clarify the effects on ligament healing and maturation. Despite these limitations, the results of this study provide valuable information concerning the efficacy of sMCL repair using suture anchors on ligament healing in grade 3 sMCL injuries. Further specific studies are necessary to overcome each limitation of the present study. Furthermore, clinical trials assessing this surgical procedure are necessary to validate the conclusions of the present study.
These results are clinically relevant because they suggest that sMCL repair using suture anchors may show similar structural properties and failure patterns as those of native sMCL.
In conclusion, the use of suture anchors is both safe and effective for the repair of grade 3 sMCL injuries.
Footnotes
Acknowledgments
We thank Shuji Hishikawa, MD, PhD, Takuya Ito, DVM, PhD, Kaori Igarashi, DVM, and the staff members in Center for Development of Advanced Medical Technology, School of Medicine, Jichi Medical University for technical support for our animal experiments. We also thank Tetsu Takahashi, M. Eng for insightful advices for our biomechanical experiments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported in part by the Grants-in-Aid for Scientific Research of Japan Society for the Promotion of Science, Grant Number JP 19K1853 from the Ministry of Education, Culture, Sports, Science and Technology, Japan. This work was also financially supported in part by a Grant from the Japan Sports Medicine Foundation, 2017.